Rocker Bottom Foot | Irreducible Dorsal Dislocation
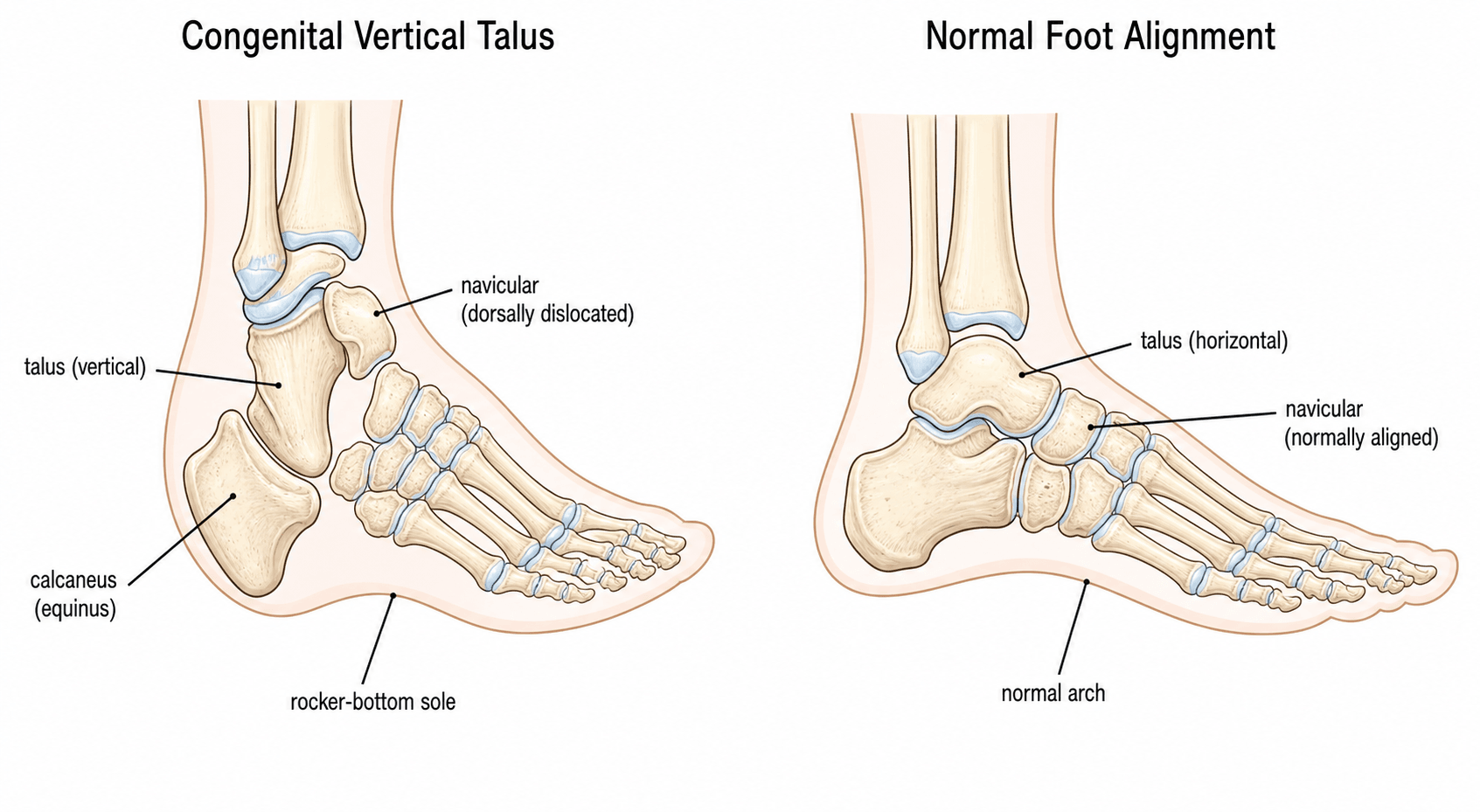
- Definition: Irreducible DORSAL dislocation of the navicular on the talus. The talus is 'vertical'.
- Deformity: Rigid Rocker Bottom Foot (Convex plantar surface). Heel in valgus and equinus.
- Key Differentiation: Differentiate from Oblique Talus (flexible) and Calcaneovalgus (flexible). CVT is RIGID.
- Diagnosis: Forces Plantarflexion Lateral X-ray. The talonavicular joint does NOT reduce (navicular stays dorsal to talus).
- Management: 'Reverse Ponseti' casting followed by minimal surgery (TN pin + Achilles tenotomy) is the new gold standard.
- “CVT is a DISLOCATION of the Talonavicular joint.
- “50% of cases are associated with syndromes (Arthrogryposis, Neural Tube Defects) - Check the spine!
- “On forced plantarflexion view, the axis of the talus passes BELOW the first metatarsal (does not align).
- “Traditional treatment was extensive release (PMR). Modern treatment is Dobbs method (Reverse Ponseti).
Check the Baby. 50% are syndromic. Exam for arthrogryposis, sacral dimple (spina bifida), and dysmorphism.
The Mimic. Oblique talus looks similar but REDUCES on plantarflexion X-ray. CVT does not reduce.
Flexible vs Rigid. Calcaneovalgus foot is flexible (dorsiflexes easily, usually packaging defect). CVT is rigid.
High Risk. Especially in teratologic cases. Maintenance bracing is crucial.
- Congenital Vertical Talus
- RIGID
- Oblique Talus
- FLEXIBLE
- Calcaneovalgus
- FLEXIBLE
- Congenital Vertical Talus
- Irreducible
- Oblique Talus
- Reducible
- Calcaneovalgus
- Reducible
- Congenital Vertical Talus
- Talus axis below 1st MT
- Oblique Talus
- Talus aligns with 1st MT
- Calcaneovalgus
- Normal alignment
- Congenital Vertical Talus
- Equinus + Valgus
- Oblique Talus
- Valgus
- Calcaneovalgus
- Calcaneus (Dorsiflexed) + Valgus
- Congenital Vertical Talus
- Surgery (Dobbs)
- Oblique Talus
- Orthotics/Obs
- Calcaneovalgus
- Stretching/Obs
ROCKERCVT Features
Hook:Rocker bottom foot features.
COPDifferential
Hook:COP the differential.
Overview & Epidemiology
Congenital vertical talus (CVT), or "congenital convex pes valgus", is a rigid, irreducible dorsal dislocation of the navicular on the head of the talus. The talus is locked in a near-vertical, plantarflexed position, producing the characteristic rocker-bottom foot.
- Incidence: Rare, approximately 1 in 10,000 live births. No strong sex predilection.
- Laterality: Bilateral in roughly half of cases.
- Associations: Around 50% are non-idiopathic (teratologic), occurring with neuromuscular or genetic disorders — arthrogryposis, myelomeningocele/spina bifida, trisomy 13/18, and chromosomal/single-gene syndromes. An autosomal-dominant familial form linked to a HOXD10 mutation has been described.
Pathophysiology & Pathoanatomy
The four key deformities:
- Hindfoot equinus: The calcaneus is fixed in plantarflexion, tethered by a contracted tendo-Achilles and posterior capsule.
- Hindfoot valgus: Increased talocalcaneal divergence.
- Midfoot dorsiflexion / dorsal dislocation: The navicular sits dorsal to the talar neck, held by contracted dorsal structures (tibialis anterior, extensor digitorum longus, extensor hallucis longus, peroneus tertius, and the dorsal talonavicular capsule). The peroneals and tibialis anterior become displaced and act as deforming dorsiflexors.
- Forefoot abduction and dorsiflexion.
The hindfoot equinus is masked by the dorsiflexed midfoot — the sole becomes convex (rocker-bottom), with the prominent talar head palpable medially in the sole. The deformity is rigid and irreducible, which is the cardinal feature separating CVT from its flexible mimics.
Classification Systems
- Idiopathic (~50%): Isolated deformity, no associated syndrome. Better prognosis; familial autosomal-dominant form linked to HOXD10.
- Teratologic / syndromic (~50%): Associated with arthrogryposis, myelomeningocele, trisomy 13/18 and other neuromuscular or chromosomal conditions. More rigid and resistant, with higher recurrence.
This idiopathic-versus-teratologic split is the clinically useful classification and guides prognosis and counselling.
Clinical Assessment
- Look:
- "Rocker Bottom" foot: Convex sole.
- Hindfoot Valgus and Equinus (Heel is up).
- Forefoot Abducted and Dorsiflexed.
- Deep creases on dorsolateral aspect.
- Feel:
- Head of Talus: Palpable in the medial sole (prominent because it points down).
- Rigid: The deformity is stiff. You cannot plantarflex the forefoot or dorsiflex the heel.
- Systemic: Check spine (spina bifida), hips (DDH), and general tone (Arthrogryposis).
- Calcaneovalgus Foot: Very common. Flexible. Heel is calcaneus (down), not equinus. Resolves with stretching.
- Oblique Talus: Less severe. Navicular reduces on talus with plantarflexion.
- Posteromedial Bowing: Apex is tibial shaft.
Investigations
X-rays (Simulated Weight Bearing / Forced Views):
- Lateral Forced Plantarflexion (KEY VIEW):
- Normal: Axis of talus lines up with 1st metatarsal.
- CVT: Axis of talus passes BELOW the 1st metatarsal. The navicular (and forefoot) remains dorsally dislocated and cannot be reduced onto the talar head.
- Lateral Forced Dorsiflexion:
- Shows fixed equinus of the calcaneus (calcaneus does not dorsiflex).
- AP View:
- Increased Talo-Calcaneal angle (Kite's angle) - indicating valgus.
Note: The navicular is not ossified until age 3, so you infer its position by the 1st metatarsal.

Radiographic Measurement and the Forced-View Protocol
The diagnosis rests on specific angles and, critically, on forced (stress) views — the topic above names the talar-axis–first-metatarsal relationship, "TAMBA", Kite's angle and Meary's, but the actual measurement protocol is worth setting out because it is the examinable crux and the way CVT is separated from its reducible mimic.
The angles (because the navicular is unossified, the first metatarsal is the surrogate)
- Talar axis–first metatarsal base angle (TAMBA): the lateral angle between the long axis of the talus and the first metatarsal. It is normally close to zero (the axes are roughly colinear — the lateral talo–first-metatarsal / Meary relationship); in CVT the talus is plantarflexed so this angle is grossly positive (plantar-apex) — treatment series report it improving from about 60 degrees toward 15 degrees with correction.
- Calcaneal axis–first metatarsal base angle (CAMBA): assesses the calcaneus-to-forefoot relationship and complements TAMBA.
- Talocalcaneal (Kite) angle: increased on both AP and lateral, reflecting the hindfoot valgus/divergence (series quote roughly 70 degrees correcting to about 31 degrees). General definition of Meary's angle is covered in the dedicated Meary angle topic.
The forced views make the diagnosis (a static film does not)
- Forced maximal PLANTARFLEXION lateral — the key view: this tests whether the talonavicular joint reduces. In a normal foot or an oblique talus the forefoot/first-metatarsal axis swings back into line with the talar axis (the navicular reduces). In CVT the talus stays vertical and the first-metatarsal axis remains dorsal — it does not align (irreducible). This single view is what separates CVT from the reducible oblique talus.
- Forced maximal DORSIFLEXION lateral: demonstrates the fixed hindfoot equinus — the calcaneus fails to dorsiflex and stays plantarflexed, confirming the rigid equinus that is clinically masked by the rocker-bottom midfoot.
Measure the talar-axis–first-metatarsal-base angle (normal near zero, grossly positive in CVT), but make the diagnosis on the forced plantarflexion lateral: the oblique talus reduces (axes realign) while CVT does not (talus stays vertical, forefoot stays dorsal). Add a forced dorsiflexion view to expose the fixed calcaneal equinus.
TAMBARadiographic Sign
Hook:TAMBA angle (though usually just 'Meary's').
Management Algorithm
Dobbs Method (Reverse Ponseti)
Gold Standard (Minimally Invasive).
- Serial Casting:
- Opposite to Ponseti clubfoot.
- Foot is Plantarflexed and Inverted (to reduce the navicular onto the talus).
- NOT dorsiflexed (this worsens the deformity by "breaking" the midfoot).
- Weekly casts (usually 5-8).
- Percutaneous Pinning:
- Once navicular reduced (confirmed on X-ray), a K-wire is passed through Talo-Navicular joint.
- Often done percutaneously or mini-open.
- Achilles Tenotomy:
- To correct the fixed equinus (which remains after casting).
- Post-op: Cast for 6-8 weeks. Pin removed.
- Bracing: Shoes/AFO long term.
Surgical Technique
Dobbs Technique Step-by-Step
Phase 1: Casting
- Counter-pressure on medial talar head (pushing it up).
- Hand creates 'mold' to plantarflex and invert forefoot.
- Goal: Stretch the tight dorsal structures (EHL, EDL, TC ligament) and reduce navicular.
Phase 2: Surgery
- Mini-Open: Small incision over TN joint.
- Pinning: Visualize reduction of navicular on talus. Drive 1.6mm K-wire from dorsal Navicular into Talus.
- Percutaneous Achilles Tenotomy: Corrects the heel equinus.
- Cast: Long leg cast in neutral.
Complications
- Risk Factor
- Neuromuscular cause, Poor bracing
- Management
- Repeat casting / Open surgery
- Risk Factor
- Extensive open release
- Management
- Fusion (salvage)
- Risk Factor
- Open surgery
- Management
- Observation
- Risk Factor
- Insufficient casting
- Management
- Revision
- Risk Factor
- Pin migration/removal
- Management
- Revision
Postoperative Care & Bracing
Protocol (Dobbs method):
- Immobilization: Long-leg cast in the corrected position for ~6-8 weeks. The talonavicular K-wire is typically removed at ~5-6 weeks.
- Bracing: After cast removal, an ankle-foot orthosis (AFO) or solid-ankle shoe is used to maintain correction. Many surgeons use a foot-abduction-style brace/AFO part-time for 1-2 years, mirroring the maintenance phase of Ponseti clubfoot care.
- Weight bearing: Permitted once the cast is removed and the foot is plantigrade; mobilisation is encouraged.
- Surveillance: Recurrence (especially in teratologic feet) is the dominant late problem, so children are followed until skeletal maturity. Early recurrence is managed with repeat casting; established relapse may need revision surgery.
Outcomes
- Dobbs Method: High success rate (greater than 90% initial correction). Reduced stiffness compared to open surgery.
- Untreated: Severe disability, painful calluses on sole (talar head), difficulty wearing shoes.
The Teratologic (Syndromic) Foot: Why It Is Different
About half of CVT is teratologic, and the topic repeatedly flags these feet as "more resistant" with "higher recurrence" — but what actually changes in management deserves to be explicit, because the teratologic foot is the one that relapses.
Why it behaves worse
- Teratologic CVT accompanies a persisting driver — the fixed contractures of arthrogryposis, the ongoing muscle imbalance and sensory loss of myelomeningocele/spina bifida, or a chromosomal syndrome (trisomy 13/18). Because the underlying neuromuscular cause keeps acting, these feet are more rigid at presentation and recur far more often than idiopathic feet (independent cohorts report recurrence well above the original idiopathic series).
How management adapts (the principle is the same; the threshold differs)
- Still start with reverse-Ponseti casting — it achieves initial correction even in syndromic and older feet — but expect more casts and a lower threshold to add a limited dorsal/talonavicular capsulotomy at the index operation (rather than tenotomy and pinning alone) to reduce relapse.
- Brace diligently and follow to skeletal maturity: maintenance bracing is not optional here, and surveillance must continue because relapse is the rule, not the exception.
- In the insensate (myelomeningocele) foot, watch the skin: cast pressure sores and plantar ulceration over the prominent talar head are real hazards.
- Salvage is needed more often: for repeated failures or neglected syndromic feet, tailored limited release or naviculectomy (and, at maturity, triple arthrodesis) is reached for sooner than in idiopathic disease.
- Treat the child, not just the foot: screen for and co-manage the spine, hips and the underlying condition (the syndrome itself is covered in the arthrogryposis and related topics).
A teratologic CVT still gets reverse-Ponseti casting first, but because the underlying neuromuscular cause keeps deforming the foot, expect more casts, a lower threshold for limited capsulotomy, near-mandatory long-term bracing, and a higher chance of needing salvage. Counsel families that recurrence is the expected problem, and protect the insensate foot's skin.
Guidelines, Registries & Global Practice
Global epidemiology:
- Rare congenital deformity, ~1 in 10,000 live births; bilateral in roughly half.
- Around 50% are teratologic, associated with arthrogryposis, myelomeningocele, trisomies (13/18) and other syndromes — proportions vary with referral pattern and access to prenatal screening.
Practice consensus (no single national guideline governs CVT):
- Prevailing position
- Reverse-Ponseti (Dobbs) serial casting then percutaneous Achilles tenotomy and talonavicular pinning — now standard across North America, UK/Europe, Australasia and increasingly worldwide
- Prevailing position
- Reserved for casting failure, neglected or rigid teratologic feet; superseded as primary treatment due to stiffness and AVN
- Prevailing position
- Naviculectomy / tailored release for complex ambulatory feet; triple arthrodesis at maturity for painful uncorrectable feet
- Prevailing position
- Examine spine (sacral dimple/myelomeningocele), hips and neuromuscular tone in every case; arrange genetics/family history in isolated familial CVT (HOXD10)
High- vs limited-resource variation:
- Where neonatal screening and paediatric orthopaedic services exist, most feet present and are cast in infancy with minimally invasive surgery.
- In limited-resource or remote settings, late/neglected presentation is more common, shifting the balance toward salvage procedures (naviculectomy, talectomy, later triple arthrodesis). Reverse-Ponseti casting is attractive globally because it is low-cost and avoids major open surgery.
- No dedicated implant registry exists for CVT (unlike arthroplasty); evidence rests on single-centre series, so practice is guided by consensus rather than registry data.
Controversies & Areas of Uncertainty
In the original Dobbs series every recurrence occurred in feet without talonavicular pinning, so most surgeons now pin routinely. The optimal pin construct, duration and whether to pin in very young infants remain debated.
Pure reverse-Ponseti relies on tenotomy plus pinning, but several groups add a limited dorsal/talonavicular capsulotomy at the index procedure to cut recurrence (Wright 2014). The line between "minimally invasive" and "selective release" is blurred and not standardised.
Independent cohorts report recurrence in up to ~40-50% of feet — well above the original series — particularly in teratologic feet. Reported success depends heavily on case mix and definition of recurrence.
For older ambulatory children, neglected feet, or repeated failures there is no consensus: options span late reverse-Ponseti, talectomy, naviculectomy (resection arthroplasty) and, at maturity, triple arthrodesis. Evidence is limited to small series.
MCQ Practice Points
Q: What represents the radiographic hallmark of CVT? A: Irreducible dorsal dislocation of the navicular on the talus, demonstrated on a forced plantarflexion lateral X-ray (talar axis passes below 1st metatarsal).
Q: What percentage of CVT cases are associated with other anomalies? A: Approximately 50% (Neural tube defects, Arthrogryposis, Genetic syndromes).
Q: How do you clinically differentiate CVT from Calcaneovalgus foot? A: CVT is RIGID and the heel is in equinus. Calcaneovalgus is FLEXIBLE and the heel is in calcaneus (dorsiflexed).
Q: In the Dobbs method for CVT, how is the foot manipulated? A: Plantarflexion and Inversion (to reduce the navicular). Dorsiflexion is AVOIDED as it causes a midfoot break.
Q: What happens to Kite's Angle (Talocalcaneal Angle) in CVT? A: It is increased (greater than 35-40 degrees), indicating severe hindfoot valgus.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is your diagnosis and differential?”
“Explain the casting and surgery.”
“How do you assess and manage recurrent / neglected CVT?”
Key Features
- Rocker Bottom Foot
- Rigid Deformity
- Talar Head in Sole
- 50% Syndromic
X-ray Sign
- Forced Plantarflexion View
- Irreducible TN joint
- Talus axis below 1st MT
- Kite's Angle greater than 40 (Valgus)
- Fixed Equinus on DF View
Management
- Dobbs Method (Gold Std)
- Cast: PF + Inversion
- Sx: Pin + Tenotomy
- Open Release (Historic)
Differential
- Calcaneovalgus (Flexible)
- Oblique Talus (Reducible)
- Clubfoot (Wait.. opposite)
- Review Spine/Hips
Complications
- Recurrence (Common)
- AVN (Open Surgery)
- Stiff Foot
- Navicular Subluxation
Evidence Base
Dobbs method (landmark)
- 11 patients (19 idiopathic CVT feet); reverse-Ponseti serial casting then percutaneous Achilles tenotomy and talonavicular pinning.
- Initial correction achieved in all 19 feet with a mean of 5 casts; no extensive releases needed.
- At minimum 2 years: mean ankle dorsiflexion 25 degrees, plantarflexion 33 degrees; all radiographic angles normalised.
- Dorsal navicular re-subluxation recurred in 3 patients, NONE of whom had undergone talonavicular pin fixation.
Minimally invasive vs extensive release (long-term comparison)
- 27 patients (42 feet) reviewed at mean 7 years (range 5-11.3): 24 feet minimally invasive vs 18 feet extensive soft-tissue release.
- Final ankle range of motion 42.4 degrees (minimally invasive) versus 12.7 degrees (extensive release), p less than 0.0001.
- PODCI pain and global function scores superior in the minimally invasive group; greater correction of hindfoot valgus.
- Benefit persisted in the isolated/idiopathic subgroup.
Reverse Ponseti: idiopathic vs teratologic & recurrence
- Prospective cohort of 13 children (21 feet); 12 idiopathic and 9 teratologic feet treated with reverse-Ponseti casting then percutaneous reduction/fixation.
- Initial correction achieved in ALL children with significant radiographic improvement.
- Recurrence occurred in 10 feet — higher than the original Dobbs series, in both idiopathic and teratologic groups.
- Authors suggest adding limited capsulotomy at the index operation may reduce recurrence; rates still lower than after open release.
Dobbs method in idiopathic AND syndromic / older children
- 15 feet in 10 patients aged 1 month to 9 years (idiopathic and syndromic) treated with the Dobbs method.
- Mean talocalcaneal angle improved 70.5 to 31 degrees; talar-axis-metatarsal-base angle 60 to 15 degrees (both p less than 0.001).
- All feet plantigrade and flexible with good radiographic correction at mean 2-year follow-up.