Decreased Neck-Shaft Angle (less than 120°) | HE Angle is Key
- Definition: Neck-Shaft angle less than 120 degrees (Normal is 135).
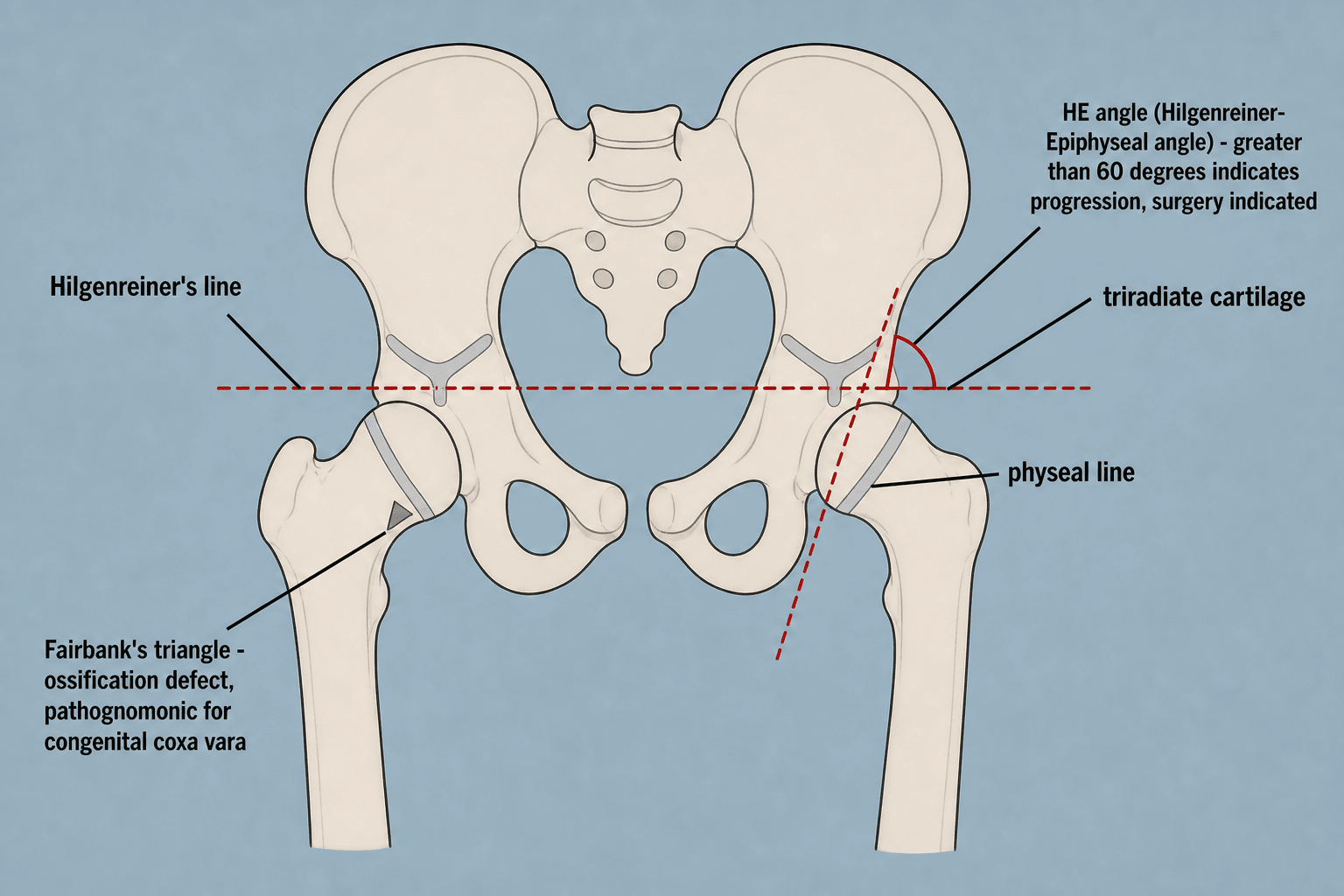
- Hilgenreiner's Epiphyseal Angle (HEA): The most important prognostic factor. Normal less than 25°. greater than 60° always progresses and needs surgery.
- Biomechanics: Coxa Vara shortens the lever arm of the abductors (Trendelenburg) and increases shear stress across the physis (slip risk).
- Fairbank's Triangle: Triangular bony fragment in the inferior femoral neck metaphysis - pathognomonic for congenital coxa vara.
- Treatment: Valgus Intertrochanteric Osteotomy is the gold standard for progressive curves.
- “Do NOT confuse with developmental dysplasia of the hip (DDH) - in Coxa Vara the head is IN the socket.
- “Trendelenburg gait is due to mechanical disadvantage (short neck), not nerve injury.
- “HEA less than 45° usually corrects spontaneously. HEA greater than 60° basically never does.
Key Distinction: In DDH, the femoral head is subluxed/dislocated. In Congenital Coxa Vara, the head is located centrally in the acetabulum, but the NECK is deformed.
Rotation Matters: Internal rotation of the leg can artificially simulate coxa valga. External rotation simulates coxa vara. Ensure standardized AP pelvis with patellae forward.
- Prognosis
- Benzoign / Spontaneous Correction
- Management
- Observation
- Prognosis
- Indeterminate / Grey Zone
- Management
- Close radiographic monitoring
- Prognosis
- Progressive / Malignant
- Management
- Valgus Osteotomy
SHORTFeatures of Congenital Coxa Vara
Hook:The leg is SHORT and the abductors are weak.
Overview and Epidemiology
Coxa Vara is defined as a femoral neck-shaft angle of less than 120 degrees. It is associated with a shortened femoral neck and relative overgrowth of the greater trochanter.
Key Concepts:
- The deformity is in the NECK, not the head or shaft.
- It is a progressive dysplasia if untreated.
- Incidence: Rare (1 in 25,000 live births).
- Bilaterality: 30-50% of cases are bilateral.
- Gender: No significant gender predilection.
- Race: More common in African American population.
- Genetics: Not clearly Mendelian, but familial clustering reported (AD with incomplete penetrance).
- Congenital (Developmental): Primary defect in enchondral ossification of the inferior aspect of the femoral neck.
- The inferior neck fails to lengthen while the superior neck continues to grow.
- This tilts the head into varus.
- The physis becomes more vertical, subjected to shear forces (Pauwels effect), which further inhibits growth (Hueter-Volkmann law).
Pathophysiology and Mechanisms
Normal Hip
- Neck-Shaft Angle: 135 degrees (Adult), 150 degrees (Infant).
- Neck Version: 15 degrees Anteversion.
- Physis: Generally horizontal, subjected to compressive loads. Compression stimulates growth (Heuter-Volkmann).
- Abductors: Gluteus Medius inserts on GT. Distance from center of rotation (Head) to GT provides the lever arm.
Normal mechanics favor joint stability.
This relationship is crucial for gait efficiency and prevention of abductor lurch.
PROMCauses of Acquired Coxa Vara
Hook:PROM date had bad hips.
Classification
1. Congenital (Present at birth):
- Associated with femoral dysplasia/PFFD.
- Short femur.
2. Developmental (Infantile):
- Normal at birth.
- Presents at walking age (waddle).
- Classic type with Fairbank's triangle.
3. Acquired:
- Trauma: Physis arrest, Malunion.
- Infection: Septic hip destroying head/neck.
- Metabolic: Rickets, Renal Osteodystrophy.
- Dysplasia: Fibrous Dysplasia (Shepherd's Crook), Osteogenesis Imperfecta.
- Perthes: Sequel of head collapse.
The etiology guides the recurrence risk.
Clinical Presentation (History)
-
Presenting Complaint: "Painless limp".
- Age: Usually noted after walking begins (2-5 years).
- Pain: Rare in childhood. If pain is present, suspect stress fracture or superimposed pathology.
- Family History: Ask about siblings or parents (hip issues).
History of premature hip replacement in parents is a clue.
Examination
- Gait: Trendelenburg gait (lurching to affected side). If bilateral, "Waddling gait".
- Stance: Positive Trendelenburg Test.
- Leg Length: True Leg Length Discrepancy (Shortening on affected side).
- ROM:
- Abduction: Restricted (finding of impingement of GT on ilium).
- Internal Rotation: Restricted (due to retroversion).
- Flexion: Usually preserved.
- Posture: Increased lumbar lordosis (if bilateral).
Investigations
Workup Pathway
AP and Frog Leg Lateral. Measure NSA and HEA. Check for Fairbank's triangle.
If suspicion of generalized dysplasia (e.g., Cleidocranial Dysostosis, Rickets). Look for clavicle absence, widended metaphyses.
Calcium, Phosphate, ALP, Vitamin D - only if Rickets suspected.
Rarely indicated. CT may help plan 3D osteotomy for complex rotation.


The Head-Shaft Angle (When the Neck Itself Is Bent)
The evidence cards target not only the HE angle but the head-shaft (HS) angle — Desai aimed for a postoperative HS angle of 130 degrees or more — yet this is a distinct measurement the topic relies on but never defines.
- Why the neck-shaft angle is unreliable in coxa vara. The standard neck-shaft angle is drawn from the femoral-shaft axis to the femoral-neck axis. In coxa vara the neck itself is short, bent and often carries an ossification defect, so a reproducible "neck axis" is hard to draw and the NSA becomes unreliable.
- The head-shaft angle avoids this by measuring from the femoral-shaft axis to a line along the base of the capital epiphysis / through the head, rather than the deformed neck — so it reports the true head-on-shaft orientation independent of neck shape.
- How the three angles work together:
- HE (Hilgenreiner-epiphyseal) angle — physeal obliquity; the shear/prognosis measure that decides whether to operate (over 60 degrees = operate).
- Head-shaft angle — the corrected head-shaft geometry; a surgical target (aim for about 130 degrees or more, per Desai).
- Neck-shaft angle — the classic definition (under 120 degrees) but the least reproducible once the neck is deformed.
- Practically: use the HE angle to decide whether to operate and the head-shaft (with HE) angle to judge how much you corrected. Desai's durable-result target was an HE angle of 35 degrees or less and a head-shaft angle of 130 degrees or more.
Q: Why is the head-shaft angle used alongside the neck-shaft angle in coxa vara? A: Because the neck is deformed, its axis (and therefore the NSA) is unreliable; the head-shaft angle measures head-on-shaft orientation from the capital epiphysis instead. Use the HE angle to decide to operate (over 60 degrees) and aim postoperatively for HE 35 degrees or less AND head-shaft 130 degrees or more for a durable correction.
Differential Diagnosis
- Key Discriminator
- Vertical physis, painless limp at walking age
- Femoral Head Position
- Reduced (in acetabulum)
- Pathognomonic / Classic Sign
- Fairbank's triangle; high HE angle
- Key Discriminator
- Subluxation/dislocation, Ortolani/Barlow in infancy
- Femoral Head Position
- Subluxed or dislocated
- Pathognomonic / Classic Sign
- Shallow acetabulum, broken Shenton's line
- Key Discriminator
- Adolescent, overweight, hip/knee pain, external rotation
- Femoral Head Position
- Slipped posteroinferiorly
- Pathognomonic / Classic Sign
- Klein's line not intersecting epiphysis
- Key Discriminator
- Older child, prior head necrosis, coxa magna/breva
- Femoral Head Position
- Reduced but deformed
- Pathognomonic / Classic Sign
- Fragmentation then coxa magna
- Key Discriminator
- Severe femoral shortening from birth
- Femoral Head Position
- May be absent/dysplastic
- Pathognomonic / Classic Sign
- Markedly short femur, Aitken classification
- Key Discriminator
- Bilateral bowing, biochemical abnormality
- Femoral Head Position
- Reduced
- Pathognomonic / Classic Sign
- Widened physes, low vitamin D / phosphate
Management Algorithm
Observation
- Indications:
- HEA less than 45 degrees.
- Asymptomatic.
- No progression on serial X-rays.
- Protocol: X-rays every 6-12 months.
- Outcome: The majority of curves with HEA less than 45 will spontaneously correct as the child grows.
Shoe lifts can be used for leg length discrepancy but do not correct the deformity.
Surgical Technique
Vascular Safety: The medial circumflex femoral artery (MCFA) is at risk during posterior approaches or aggressive medial dissection. The lateral approach is safer but requires deeper retraction. Avoid damaging the trochanteric apophysis in young children (less than 5 years) to prevent iatrogenic growth arrest.
Valgus Intertrochanteric Osteotomy
Principle: A closing wedge valgus osteotomy (remove lateral wedge) or opening wedge medial. Closing wedge is safer for union.
Steps:
- Setup: Supine on radiolucent table. Fluoroscopy.
- Approach: Direct lateral approach to proximal femur. Elevate Vastus Lateralis.
- Careful hemostasis of perforating vessels.
- Expose the flare of the greater trochanter.
- Guide Wire: Insert guide wire into femoral neck/head.
- The angle of insertion determines correction.
- If using a 130 deg blade plate, insert wire at predetermined angle to shaft to achieve desired valgus.
- Seating Chisel: Insert seating chisel over/parallel to wire.
- Osteotomy:
- Perform intertrochanteric bone cut.
- Remove a laterally based wedge of bone (calculated from preoperative tracing).
- Tip: The size of the wedge (in mm) roughly equals the degrees of correction needed on some plating systems, but templates are safer.
- Reduction: Abduct the shaft to close the osteotomy. The head/neck unit is now more valgus.
- Fixation: Insert Blade Plate or Pediatric Locking Plate (cannulated screw system).
- Rotation: Correct retroversion by internally rotating the distal fragment before plating (if needed).
- Adductor Tenotomy: Often required (percutaneous) as valgus lengthens the leg and tightens adductors.
Post-Op: Spica cast usually needed for younger children (less than 6-8). Protected weight bearing for older.
Pitfalls to Avoid:
- Under-correction (High recurrence rate).
- Anterior penetration of the plate (femoral neck is retroverted).
- Injury to the trochanteric apophysis (posterior approach).
Careful preoperative planning is the key to avoiding these pitfalls.
HAVSurgical Goals
Hook:HAV to fix the mechanics.
Greater Trochanteric Overgrowth and Trochanteric Advancement
Coxa vara repeatedly runs into the greater trochanter — Viva 4 asks about "trochanteric advancement if the GT is very high", the Desai series found trochanteric overgrowth with abductor weakness in 5 of 12 hips, the "articulo-trochanteric distance" is a named measurement, and premature capital-physis closure yields a short neck (coxa breva) with a relatively high trochanter. Here is the concept those references rely on.
- Why the trochanter matters. The abductors act through the lever arm from the hip centre to the greater trochanter. In coxa vara the short/varus neck plus trochanteric overgrowth brings the trochanter up to or above the centre of the femoral head, shortening the abductor lever arm and slackening the muscle — the mechanical basis of the Trendelenburg gait that can persist even after the neck angle is corrected.
- Measuring it — the articulo-trochanteric distance (ATD). The ATD is the vertical distance from the tip of the greater trochanter to the top of the femoral head on an AP film (normally the head sits roughly 1 to 2 cm above the trochanter tip). A reduced, zero or negative ATD (trochanter at or above the head) quantifies trochanteric overgrowth and abductor insufficiency.
- Two mechanisms:
- Absolute overgrowth — the trochanteric apophysis keeps growing while the capital physis is arrested (classically after premature capital-physis closure, giving coxa breva), so the trochanter overtakes the head.
- Relative overgrowth — the neck is simply short/varus, so the normally-growing trochanter sits relatively high.
- What to do about it:
- Distal (and lateral) trochanteric advancement/transfer — osteotomise the greater trochanter and move it distally to restore abductor length-tension and the lever arm; used for the high trochanter in an older child or after coxa breva.
- Greater trochanteric (apophyseal) epiphysiodesis — in a young child with growth remaining, arresting the trochanteric apophysis lets the neck "catch up" and prevents future overgrowth.
- This is exactly why the surgical warnings stress protecting the trochanteric apophysis: iatrogenic arrest tips the neck-trochanter balance the wrong way.
Q: A child has a persistent Trendelenburg gait after a technically adequate valgus osteotomy — why, and what measurement and procedure address it? A: A high-riding greater trochanter (absolute or relative overgrowth) keeps the abductor lever arm short. Quantify it with the articulo-trochanteric distance (trochanter tip relative to the head, normally ~1 to 2 cm below the head). Treat with distal trochanteric advancement/transfer in the older child, or prophylactic trochanteric apophyseal epiphysiodesis in the young child to prevent overgrowth.
Complications
- Risk Factor
- Under-correction (HEA greater than 35)
- Prevention
- Overcorrect to valgus
- Management
- Repeat Osteotomy
- Risk Factor
- Surgical trauma to physis
- Prevention
- Stay 1cm from physis
- Management
- Epiphysiodesis contralateral
- Risk Factor
- Vessel injury
- Prevention
- Careful dissection
- Management
- Bisphosphonates / Salvage
- Risk Factor
- Loss of fixation
- Prevention
- Spica cast augmentation
- Management
- Osteotomy
- Risk Factor
- Unilateral disease
- Prevention
- Shoe lifts
- Management
- Contralateral Epiphysiodesis
- Risk Factor
- Surgeon error
- Prevention
- Antibiotics
- Management
- Washout
Premature closure of the capital femoral physis is a devastating complication. It leads to a short femoral neck (Coxa Breva) and recurrence of varus if the troch continues to grow. It usually results from direct surgical trauma (drill/chisel) or vascular injury.
The most common cause of recurrence is under-correction. If the HEA is not restored to less than 40 degrees (ideally less than 30), the shear forces remain, and the deformity will recur via the Hueter-Volkmann principle.
Postoperative Care
- Immobilization:
- Age less than 6-8 years: Hip Spica Cast for 6 weeks. Fixation alone is often insufficient for active children.
- Age greater than 8 years: Touch weight bearing with crutches (if reliable).
- X-rays:
- Check at 6 weeks for union.
- Check at 3 months, 6 months, 1 year.
- Hardware Removal:
- Often required once healed (12-18 months) as the plate will become buried in bone and hard to remove later.
- Blade plates can act as stress risers.
- Spica cast or Non-weight bearing.
- Ensure cast comfort.
- Monitor for cast sores.
- Cast removal.
- X-ray to confirm union.
- Hydrotherapy / Pool walking.
- Gentle active ROM (Abduction/Flexion).
- Touch weight bearing.
- Full weight bearing.
- Abductor strengthening (Clamshells).
- Normalise gait.
- Monitor for leg length discrepancy.
Outcomes and Prognosis
- Natural History:
- HEA less than 45: 80% spontaneous resolution.
- HEA greater than 60: 100% progression. untreated leads to severe shortening, limp, and early OA.
- Surgical Outcomes:
- Success Rate: 90% correction if adequate valgus achieved.
- Limp: Usually resolves if biomechanics are restored.
- Leg Length: Osteotomy lengthens the leg (valgus gain), but pre-existing physeal arrest may result in permanent shortening (0.5 - 2 cm).
- Long Term:
- Even with correction, the hip is rarely "normal".
- Acetabular dysplasia usually remodels if head is centered.
- Mild risk of OA remains.
Guidelines, Registries & Global Practice
Global Epidemiology:
- Developmental/congenital coxa vara is rare (~1 in 25,000 live births) and far less common than DDH.
- Reported across all populations; some series describe higher frequency in populations of African descent and in Scandinavian cohorts (echoing the distribution of Blount disease).
- Often diagnosed late once the child is walking; delayed presentation is most marked in limited-resource and rural settings.
Guideline & Consensus Position (side by side):
- Position on Coxa Vara
- HE-angle-based decision: surgery for HE angle greater than 60 degrees; observe less than 45 degrees; serial review for the 45-60 grey zone
- Position on Coxa Vara
- Refer progressive, painful, or unilateral deformity to a tertiary paediatric orthopaedic unit; observation for non-progressive minor varus
- Position on Coxa Vara
- Valgus intertrochanteric osteotomy with fixed-angle (blade plate) or pediatric LCP; aim to convert vertical physis to horizontal
- Position on Coxa Vara
- Concordant with HE-angle thresholds; emphasise correction of version and trochanteric overgrowth in older children
There is broad international agreement: the HE angle drives the decision and valgus intertrochanteric osteotomy is the definitive operation. Differences are largely in implant preference and timing.
Registry & Implant Notes:
- No dedicated paediatric coxa-vara registry exists; this is a rare deformity managed in tertiary centres rather than tracked at population scale.
- Pediatric proximal femoral locking compression plates (LCP) have largely replaced fixed-angle blade plates in many units for ease of application; published series report high but reliable hardware-removal rates for trochanteric irritation.
- Fixed-angle blade plates remain a robust, low-cost option and are still widely taught.
High- vs Limited-Resource Practice Variation:
- High-resource: 3D CT planning for combined varus/version correction, image intensifier-guided osteotomy, modern locking implants, early mobilisation.
- Limited-resource: Reliance on plain radiographs and templating; blade plates or even smooth wires with hip spica for fixation; later presentation means larger corrections and more frequent need for concomitant trochanteric advancement.
- Across all settings, the principle is identical — overcorrect to valgus, restore a near-horizontal physis, and protect the construct until union.
Controversies & Areas of Uncertainty
Earlier osteotomy (before age 6) allows acetabular remodelling but smaller bones are technically harder and recurrence is higher if the physis remains sick. There is no consensus on the ideal age window; most operate once the HE angle reaches greater than 60 degrees or progression is documented, regardless of age.
How much valgus to aim for is debated. Targets range from a postoperative HE angle of 35 degrees or less to deliberate overcorrection to a neck-shaft angle of 150 degrees. Excess valgus risks abductor lengthening and a Trendelenburg lurch; under-correction risks recurrence.
Fixed-angle blade plates give predictable geometry but are unforgiving; pediatric LCPs are easier to apply but carry high hardware-removal rates for trochanteric irritation. No high-level trial demonstrates superiority of one over the other.
Hemiepiphysiodesis (guided growth) is attractive but the proximal femoral physis in coxa vara is intrinsically abnormal, so response is unpredictable. It is not an established substitute for corrective osteotomy in significant deformity.
Evidence is limited to small retrospective series (rarity of the condition precludes randomised trials). There is no validated threshold for the precise amount of overcorrection, no consensus on managing the grey-zone (45-60 degrees) HE angle, and no registry-level long-term arthritis data. Treat published "rules" as expert-derived guidance, not Level 1 evidence.
MCQ Practice Points
Q: The most reliable radiographic measurement for predicting progression in Congenital Coxa Vara is: A. Neck-Shaft Angle B. Hilgenreiner's Epiphyseal Angle (HEA) C. Acetabular Index D. Articulo-trochanteric distance Answer: B. The HEA measures the obliquity of the physis. A vertical physis (greater than 60 deg) predicts progression due to shear.
Q: Which feature distinguishes Congenital Coxa Vara from Developmental Dysplasia of the Hip (DDH)? A. Short leg B. Trendelenburg gait C. Head located in acetabulum D. Limited abduction Answer: C. In DDH, the head is subluxed/dislocated. In Coxa Vara, the head is reduced, but the neck is bent.
Q: An HE Angle of 70 degrees is an indication for: A. Observation B. Shoe lift C. Valgus Osteotomy D. Arthrodesis Answer: C. HEA greater than 60 degrees is the absolute indication for surgery as spontaneous resolution does not occur.
Q: Fairbank's triangle represents: A. A fracture B. A defect in ossification C. A tumor D. Infection Answer: B. It is a triangular cartilaginous defect in the inferior femoral neck ossification center.
Q: The primary biomechanical goal of osteotomy in Coxa Vara is to: A. Lengthen the leg B. Convert shear forces to compression C. Improve cosmesis D. Reduce the head Answer: B. By making the physis horizontal (HEA less than 30), shear forces (which inhibit growth) are converted to extensive/compressive forces (which stimulate growth).
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 3-year-old is brought in by parents for a waddling gait. Painless. Unremarkable birth history. Describe your assessment.”
“You see a 4-year-old with bilateral Coxa Vara. HE Angle is 50 degrees on the right and 55 on the left. Parents are worried. Plan?”
“You performed a osteotomy 1 year ago. X-rays now show the varus has returned. What happened and what now?”
“A 10-year-old presents with neglected coxa vara. Short leg (-3cm). HEA 70 degrees. Is it too late?”
“A 30-year-old presents with unilateral hip pain. X-rays show a pistol-grip deformity and mild OA. History of childhood osteotomy. What is this?”
Key Numbers
- Normal NSA: 135 deg
- Coxa Vara: less than 120 deg
- Severe Vara: less than 90 deg
- Normal HEA: less than 25 deg
- Surgery Indicator: HEA greater than 60 deg
- Grey Zone: 45-60 deg
Pathology
- Vertical Physis
- Ossification defect (Fairbank's Triangle)
- Shear forces inhibit growth
- Short neck + High Trochanter
Clinical
- Painless limp
- Trendelenburg Gait
- Short leg
- Limited Abduction/Int Rotation
Surgery
- Valgus Intertrochanteric Osteotomy
- Adductor Tenotomy
- Spica Cast (if young)
- Overcorrect (Valgus is good)
Evidence Base
HE Angle: The Prognostic Cornerstone
- Retrospective review of 42 coxa vara cases, 22 true congenital
- Introduced the Hilgenreiner-epiphyseal (HE) angle as the operative threshold
- HE angle greater than 60 degrees: indication for surgery
- HE angle 45-60 degrees: grey zone, observe; less than 45 degrees: generally corrects spontaneously
Valgus Osteotomy: 20-Year Outcomes
- 20 hips (12 patients) with congenital coxa vara, valgus subtrochanteric osteotomy, mean 20-year follow-up
- Mean preoperative HE angle 66 degrees, head-shaft angle 96 degrees
- Postoperative HE angle of 35 degrees or less AND head-shaft angle of 130 degrees or more correlated with satisfactory results
- Trochanteric overgrowth with abductor weakness in 5 of 12 hips with that finding
Valgus Osteotomy & Acetabular Remodelling
- 8 patients (12 hips), valgus intertrochanteric osteotomy, mean age 7.9 years
- Mean HE angle improved from 75 to 25 degrees; neck-shaft angle 95 to 137 degrees (125 degrees at follow-up)
- Only 3 hips maintained more than 80% correction at minimum 2-year follow-up — all developmental subtype
- Acetabular depth improved significantly when surgery was done before age 6
Classification & Management Review
- Classifies childhood coxa vara as developmental, congenital, dysplastic, or traumatic
- Evaluation must seek family history, trauma/infection, and associated skeletal dysplasia
- Surgery indicated when the deformity is progressive, painful, unilateral, or causes leg-length discrepancy
- Radiographs determine laterality and whether deformity is at or below the physis
Pediatric LCP for Proximal Femoral Osteotomy
- 13 hips (11 patients) using a low-profile pediatric proximal femoral locking compression plate
- All hips improved radiographic parameters, pain, and Merle d'Aubigne-Postel scores
- 11 of 13 hips (85%) required plate removal at mean 15.8 months, usually for greater-trochanter discomfort
- Lower profile than blade plates but lateral hip irritation remains common
Biomechanics of the Varus Hip
- Foundational biomechanical analysis of physeal loading in the varus hip
- Distinguished shear from compressive forces across the proximal femoral physis
- A vertical (varus) physis converts protective compression into growth-inhibiting shear
- Provides the rationale for converting a vertical physis to horizontal via valgus osteotomy