The Race Against Pulmonary Insufficiency
- Thoracic Insufficiency Syndrome (TIS): The inability of the thorax to support normal respiration.
- Mehta Angle (RVAD): The key predictor of progression in infantile scoliosis.
- MRI: Mandatory for all EOS cases (Neural axis abnormalities in 20-40%).
- C-EOS Classification: Etiology, Cobb, Kyphosis, Progression.
- Treatment: Delay fusion! Use Casting, Bracing, or Growing Rods.
- “Look for cutaneous stigmata (hairy patch, dimple) - Intraspinal pathology
- “Assess flexibility (Bending films)
- “Neurology is mandatory (Abdominal reflexes)
- “Plagiocephaly is often associated with Infantile Scoliosis
Standard of Care. 20-40% of EOS patients have neural axis abnormalities (Chiari/Syrinx) even with normal neuro exam.
Greater than 20° = Progressive. less than 20° = Resolving. Key predictor for Infantile Scoliosis.
Avoid Early Fusion. Fusing more than 4 thoracic segments before age 8 stunts lung development → Thoracic Insufficiency Syndrome.
- Infantile
- Male
- Juvenile
- Female
- Adolescent (AIS)
- Female
- Infantile
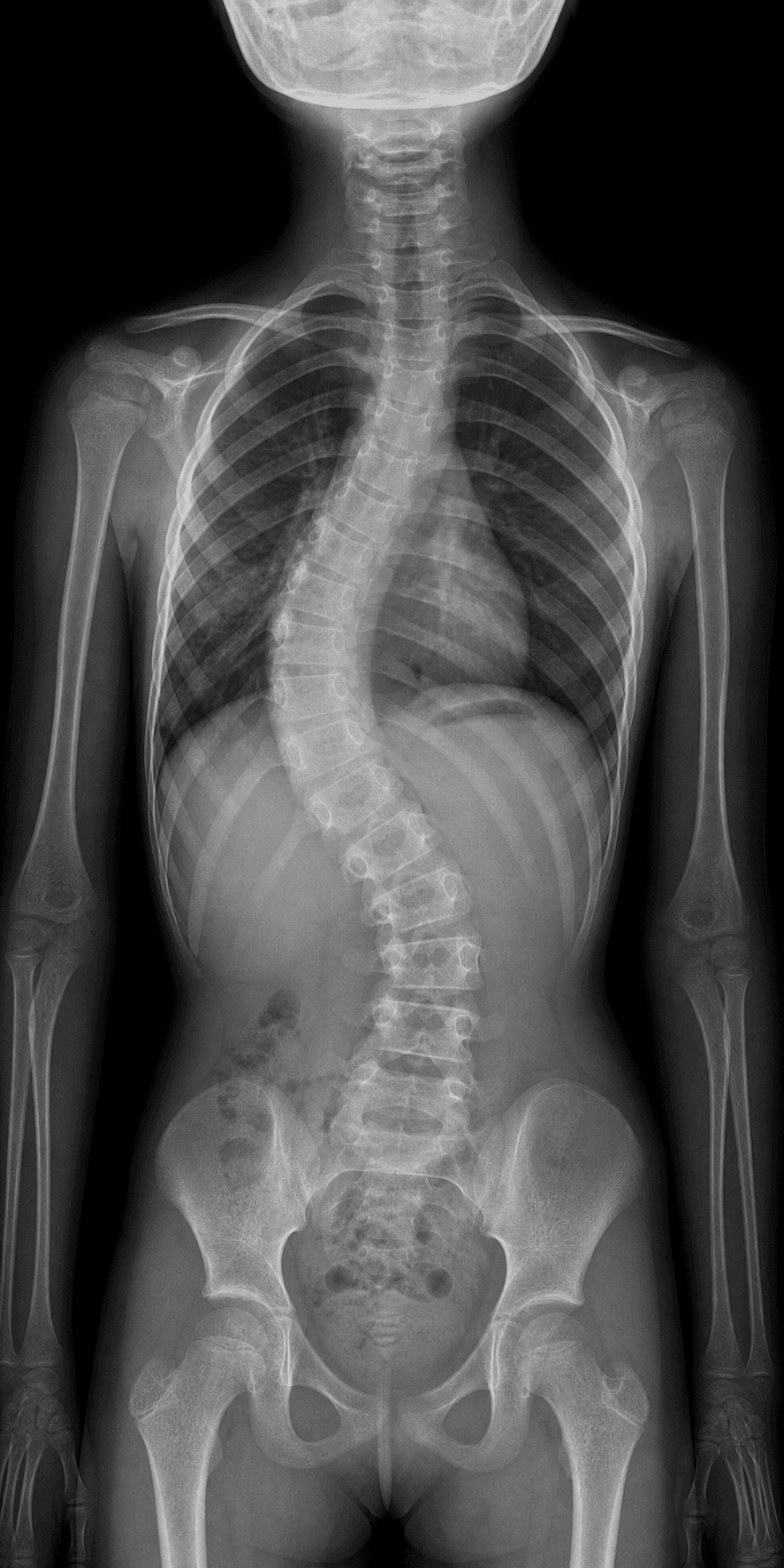
- Left Thoracic
- Juvenile
- Right Thoracic
- Adolescent (AIS)
- Right Thoracic
- Infantile
- High (MRI mandatory)
- Juvenile
- High (MRI mandatory)
- Adolescent (AIS)
- Low (MRI if red flags)
- Infantile
- Resolves (80%) or Severe
- Juvenile
- Often Progresses
- Adolescent (AIS)
- Variable
RPCRisk of Progression (Infantile)
Hook:RPC (Rapid Progression Criteria).
Overview/Epidemiology
Early Onset Scoliosis is a time-based definition (Age less than 10). It encompasses a heterogeneous group of diagnoses.
- Pulmonary Impact: The primary concern is Thoracic Insufficiency Syndrome (TIS).
- Alveoli multiply rapidly until age 8.
- Severe deformity restricts lung volume, leading to restrictive lung disease to Pulmonary Hypertension to Cor Pulmonale to Early Death.
- Epidemiology:
- Infantile Idiopathic: Rare (under 1% of all idiopathic scoliosis in most series). Male predominance. Left-sided thoracic curves are typical. Higher incidence historically reported in Europe than North America.
- Juvenile Idiopathic: Female predominance. Right-sided thoracic curves (like AIS). Progression is common and often relentless without treatment.
Pathophysiology and Mechanisms
The Mehta Angle (Rib-Vertebral Angle Difference - RVAD) This is the angle between the rib neck and the vertebral body.
- Measured at the apical vertebra.
- Calculation: RVAD = Angle on Concave side - Angle on Convex side.
- Significance:
- Less than 20 degrees: 80% chance of spontaneous resolution. (Resolving).
- Greater than 20 degrees: 80% chance of progression. (Progressive).
Rib Head Phases (Mehta)
- Phase 1: Prominent gap between rib head and vertebral body.
- Phase 2: Rib head overlaps the vertebral body. Indicates progression.
EOSC-EOS Etiology Categories
Hook:CNSI (Central Nervous System Injury? No, just the list).
Classification Systems
C-EOS Classification (2014)
1. Etiology (CNSI):
- Congenital, Neuromuscular, Syndromic, Idiopathic.
2. Cobb Angle:
- Current magnitude of the major curve.
3. Kyphosis:
- Hyperkyphosis (greater than 50) is a major negative predictor for pulmonary function.
4. Progression Modifier:
- P0: Stable (less than 10 deg/year).
- P1: Progressive (greater than 10 deg/year).
- P2: Malignant (greater than 20 deg/year).
Clinical Assessment
- Birth Hx: Prematurity? NICU admission?
- Development: Walking age? Milestones? (Neuromuscular).
- Family Hx: Neurofibromatosis? Marfan?
- Skin: Café-au-lait spots (NF1), Hairy patch (Spinal dysraphism), Laxity (Ehlers-Danlos).
- Neurology: Full exam. Abdominal reflexes are critical for Syringomyelia.
- Spine: Assess flexibility. Can you correct it with traction/bending?
- Chest: Pectus deformities? Rib hump?
Investigations
- Whole Spine X-ray (PA and Lateral): Measure Cobb, Kyphosis.
- Bending Films / Traction Films: Assess flexibility.
- Mehta Angle (RVAD): Calculate on apical vertebra.
- Mandatory for all patients.
- Look for: Chiari Malformation, Syrinx, Tethered Cord, Diastematomyelia, Intraspinal tumors.
Genetic Testing:
- Consider if syndromic features present (Microarray).
Management Algorithm
1. Serial Casting (Mehta/Cotrel)
- Indication: Idiopathic Infantile, Progressive, Flexible.
- Goal: Cure? (Possible if started young less than 2 years) or Delay surgery.
- Technique: Under GA, traction and derotation, plaster jacket applied. Changed every 2-3 months.
2. Bracing (TLSO)
- Indication: Juvenile cases, older children, or maintenance after casting.
- Efficacy: Less effective than casting for true infantile curves.
LSGGoals of Management
Hook:LSG (Life Support Growth).
Surgical Techniques
Magnetically Controlled Growing Rods
Concept: Implant proximal and distal anchors (screws/hooks) spanning the deformity. Connect with a rod that has a magnetic actuator. Procedure:
- Limited exposure at top and bottom.
- Sub-muscular passage of rods.
- Lengthening: Done in clinic using an external magnet every 3 months. Pros: No repeated surgeries for lengthening. Cons: Metal artifacts on MRI. Actuator failure.
Complications
- Rate
- High (Repeat surgeries)
- Prevention/Management
- Sub-muscular placement. MCGR reduces rate.
- Rate
- Common
- Prevention/Management
- Dual rods better than Single rods. Diameter increase.
- Rate
- Common
- Prevention/Management
- Hooks usually safer than screws in osteoporotic/small bone.
- Rate
- Common
- Prevention/Management
- Don't stop at the apex of kyphosis.
- Rate
- Inevitable
- Prevention/Management
- Delay open surgery as long as possible.
Postoperative Care
- Bracing: Most growing rod patients wear a brace post-op to protect the anchors.
- Physio: Essential to maintain flexibility (auto-fusion prevention).
- Follow-up: Lengthening schedule (MCGR: Clinic every 3 months. TGR: Surgery every 6 months).
Outcomes/Prognosis
- Pulmonary: The main goal is survival. Early fusion (less than age 5) results in severe TIS and death. Delaying fusion until age 10-12 significantly improves pulmonary volume.
- Deformity: complete correction is rarely the goal. "Control" is the goal.
- Final Fusion: Usually performed at skeletal maturity (Age 12-14 females, 14-16 males) to lock in the correction.
Guidelines, Registries & Global Practice
Global epidemiology
- EOS is a heterogeneous, time-based group (onset under age 10). Idiopathic infantile scoliosis accounts for under 1% of idiopathic curves in most series, with historically higher reported rates in Europe than North America. Congenital and neuromuscular aetiologies dominate the structural/progressive end of the spectrum worldwide.
Society guidance, side by side
- Emphasis
- C-EOS classification (Aetiology–Cobb–Kyphosis–Progression); growth-friendly principles; final fusion at maturity
- Emphasis
- Whole-spine MRI mandatory in EOS; serial casting first-line for flexible idiopathic infantile curves; MCGR favoured to cut reoperations
- Emphasis
- Tertiary-centre management; RVAD/serial monitoring of infantile curves; casting and growth-friendly surgery pathways
- Emphasis
- Strong casting tradition (EDF/Cotrel); emphasis on lung growth and avoiding early fusion
Registry and multicentre evidence
- Practice is driven largely by multicentre prospective EOS registries (e.g. the Pediatric Spine Study Group / Growing Spine Study Group datasets) rather than national arthroplasty-style registries, given device diversity and small numbers. These cohorts underpin the data on dual-rod growth rates, MCGR diminishing returns, and complication profiles.
High- vs limited-resource practice variation
- High-resource settings: ready access to whole-spine MRI, MCGR (avoiding repeated open lengthenings), VEPTR, intraoperative neuromonitoring and multidisciplinary paediatric pulmonology/spine teams.
- Limited-resource settings: greater reliance on serial casting and traditional growing rods (lower implant cost but repeated GA), with MRI and MCGR access constrained. Halo-gravity traction is a valuable low-cost adjunct for severe rigid curves. Late presentation with established thoracic insufficiency is more common.
Deep Dive: Surgical Pearls
1. The Law of Diminishing Returns With traditional growing rods, every time you go in to lengthen (every 6 months), the spine gets stiffer (auto-fusion). By the time you do the final fusion, the spine may already be fused in a less-than-perfect position. MCGR helps avoid this "Law of Diminishing Returns" by avoiding open surgery.
2. Crankshaft Phenomenon If you fuse the posterior elements (or they auto-fuse) but the anterior vertebral body growth plates remain open, the spine will twist and rotate as it grows anteriorly.
- Prevention: In young children (less than 10), definitive fusion often requires Anterior and Posterior fusion to stop all growth centers.
3. Hemiepiphysiodesis For a congenital hemivertebra:
- You can fuse the convex side (epiphysiodesis). The concave side continues to grow, potentially correcting the curve over time.
- Or: Resect the hemivertebra entirely (more aggressive, better correction).
The Three Categories of Growth-Friendly Surgery
The topic lists growing rods, MCGR, VEPTR, Shilla and convex hemiepiphysiodesis as a flat menu, but the examiner's organising framework - that every growth-friendly implant works by one of three mechanisms - is never assembled. Knowing the category explains how each device behaves over time and how to choose between them.
- How it works
- Periodically lengthened to push the spine/thorax apart and outgrow the deformity
- Examples
- Traditional growing rods (surgical lengthening), MCGR (external magnet), VEPTR (rib-based, expands thorax)
- Trade-off
- Workhorse, but repeated procedures/auto-fusion and the law of diminishing returns
- How it works
- Anchors fixed at the apex/foundations; the spine slides and grows along the rod without repeated lengthenings
- Examples
- Shilla (apex fixed, sliding end screws), Luque trolley
- Trade-off
- Avoids repeated lengthening surgery but gives less deformity control and generates metal debris
- How it works
- Tether/staple the convex side to slow convex growth so the concave side catches up (Hueter-Volkmann)
- Examples
- Convex hemiepiphysiodesis, vertebral body stapling, anterior vertebral body tethering
- Trade-off
- Only for smaller, flexible curves with substantial growth remaining
So the device choice follows the curve: a large, progressive curve needs the corrective power of distraction; a curve where repeated surgery is undesirable may suit growth-guidance; and a small, flexible curve with lots of growth left is the candidate for compression/growth-modulation. The distinction also explains the named behaviours elsewhere in this topic - the "law of diminishing returns" and auto-fusion belong to the distraction category, while convex hemiepiphysiodesis (used for the congenital hemivertebra) is the compression category.
Every growth-friendly implant is distraction-based (growing rods/MCGR/VEPTR - lengthened to outgrow the curve, prone to diminishing returns and auto-fusion), growth-guidance (Shilla/Luque trolley - the spine slides along fixed-apex rods, fewer surgeries but less control), or compression/growth-modulation (convex hemiepiphysiodesis/stapling/tethering - slow the convex side, only for small flexible curves with growth left). Name the category and the behaviour follows.
Foundations and Anchors: Where the Construct Holds
The topic repeatedly relies on the concept of "anchors" - anchor pull-out, hooks versus screws, "rib-to-rib or rib-to-spine", the rib-based versus spine-based debate, "extending fixation to ribs or pelvis", and avoiding proximal junctional kyphosis - but never explains the foundation concept that ties them together. A growth-friendly construct needs a stable proximal foundation and a stable distal foundation, each with several anchor points, bridging the deformity.
- Options
- Upper thoracic pedicle screws/hooks (claw construct)
- Trade-off
- Better deformity control, but risks proximal junctional kyphosis and proximal auto-fusion - do not end at the apex of a kyphosis
- Options
- Rib cradles/hooks (VEPTR-type)
- Trade-off
- Spares the immature proximal spine and expands the thorax, but rib migration/cut-out is common
- Options
- Lower lumbar pedicle screws
- Trade-off
- Preserves distal motion segments; used when the pelvis is level and distal bone is adequate
- Options
- Iliac / S-hook pelvic fixation
- Trade-off
- Needed for neuromuscular curves with pelvic obliquity or poor distal bone stock
The foundation choice is a series of trade-offs: rib versus spine proximally (spare the spine and gain thoracic expansion but risk migration/cut-out, versus hold better but risk PJK) and spine versus pelvis distally (preserve motion versus control pelvic obliquity in neuromuscular disease). The common failure modes map onto the foundations: anchor pull-out in small/osteoporotic bone (where hooks may hold better than screws), rib migration/cut-out with rib cradles, and PJK when the proximal foundation is too low or ends at a kyphotic apex. This is why a foundation uses multiple anchor points and why a salvage of failed rods often means moving the foundation (to ribs proximally, or to the pelvis distally).
A growing construct spans the deformity between a proximal and a distal foundation, each with several anchors. Proximally choose spine (better control, but PJK/auto-fusion - never end at a kyphosis apex) or ribs (spares the spine and expands the thorax, but migrates/cuts out); distally choose lumbar spine (preserves motion) or pelvis (for neuromuscular pelvic obliquity/poor bone). Pull-out, rib cut-out and PJK are the foundation failure modes, and salvage usually means re-siting the foundation.
Controversies and Areas of Uncertainty
- RVAD threshold: The classic 20-degree Mehta cut-off is challenged — long-term data suggest an optimal threshold nearer 17 degrees and warn against relying on a single index measurement (Lloyd et al, 2020). Serial RVAD and Cobb trends are more reliable than any one value.
- MCGR metal ions and reliability: Magnetically controlled rods reduce open lengthenings, but elevated serum titanium, actuator/pin failure, and progressive loss of distraction (a residual "law of diminishing returns") generate ongoing debate about long-term safety and true cost-effectiveness.
- Casting vs early surgery: When to abandon casting for a growth-friendly construct is not standardised. Casting can be curative if started under age 2, but late or stiff curves respond poorly.
- Rib-based vs spine-based anchors: VEPTR (rib-based) directly expands the thorax but has high migration/cutout rates; spine-based anchors give better deformity control but less direct chest-wall benefit. The optimal hybrid is unsettled.
- Graduation strategy: Whether to perform definitive fusion, "watchful waiting" with retained rods, or remove implants at skeletal maturity remains individualised, with no consensus on the best endpoint.
- Crankshaft prevention: The need for anterior growth arrest (combined anterior/posterior fusion) in very young children is debated in the era of all-pedicle-screw posterior constructs.
Deep Dive: EDP (Early Derotation Plastering)
The Mehta Technique Min Mehta revolutionized the treatment of infantile scoliosis.
- Principle: The spine grows rapidly in the first 2 years. If you can hold it straight, the growth will correct the deformity (Hueter-Volkmann law).
- Technique:
- General Anaesthesia.
- Risser Table (Traction frame).
- Derotation: Correct the rotation, not just the lateral bend. Mold over the apical rib hump.
- Window: Cut a large anterior "mushroom" window for belly breathing (infants are diaphragmatic breathers).
- Result: Can result in a permanent cure for idiopathic curves if started early.
MCQ Practice Points
Q: What is the most reliable predictor of progression in infantile idiopathic scoliosis? A: The Mehta Angle (Rib-Vertebral Angle Difference - RVAD). Greater than 20 degrees = Progression.
Q: At what age does the multiplication of alveoli (lung development) plateau? A: Age 8. (This is why fusion before age 8 is so dangerous for lung function).
Q: What is the rate of neural axis abnormalities in "idiopathic" early onset scoliosis? A: 20-40%. (Hence MRI is mandatory for all).
Q: What is the typical pattern of Infantile Idiopathic Scoliosis? A: Male gender, Left-sided Thoracic curve. (Opposite of Adolescent Idiopathic).
Q: What is the Crankshaft Phenomenon? A: Rotational deformity progression after posterior fusion, due to continued anterior growth.
Self-Assessment Quiz
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“18-month-old boy. Left thoracic curve 35 degrees. Parents are worried.”
“3-year-old. L1 Hemivertebra noticed on X-ray. Fully segmented. Curve is 30 degrees.”
“8-year-old with SMA (SMA Type 2). Has growing rods. Now has proximal hook pull-out and skin breakdown.”
DEFINITIONS
- Age less than 10
- Infantile (0-3)
- Juvenile (4-10)
- Congenital / NM / Syndromic / Idiopathic
RED FLAGS
- Left curve (check MRI)
- Hairy Patch
- Pain (Osteoid Osteoma)
- Neuro Deficit
KEY NUMBERS
- Mehta greater than 20 deg (Progressive)
- RVAD less than 20 deg (Resolving)
- Alveoli age 8
- MRI 40% abnormal
MANAGEMENT
- Cast (Mehta)
- Brace (maintenance)
- Grow (Rods/VEPTR)
- Fuse (Final)
Evidence Base
- Defined the Rib-Vertebral Angle Difference (RVAD) at the apical vertebra
- RVAD greater than 20 degrees identifies the progressive (vs resolving) infantile curve
- Phase 2 rib-head relationship (rib head overlaps vertebral body) indicates progression
- Retrospective UK tertiary-unit cohort of infantile idiopathic scoliosis
- Progressive curves had significantly higher index Cobb and RVAD than resolving curves
- Optimal RVAD threshold for predicting progression was 17.1 degrees, lower than the classic 20 degrees
- Authors advise caution in relying on a single index RVAD measurement
- Defined Thoracic Insufficiency Syndrome (TIS): inability of the thorax to support normal respiration or lung growth
- Characterised the 3D thorax — volume (rib-cage width/depth and spinal height) and function (diaphragm, accessory muscles)
- Described the thumb-excursion test and Space Available for Lung as clinical/radiographic markers
- Treatment should expand thoracic volume and stabilise the chest wall without spinal fusion
- Multicentre series of 23 children treated with dual growing rods (no prior surgery, minimum 2-year follow-up)
- Mean scoliosis improved from 82 to 36 degrees and was maintained
- T1-S1 length increased an average of 1.21 cm/year; Space Available for Lung ratio improved from 0.87 to 1.0
- Complications in 11 of 23 patients (48%) over the treatment period
- Prospective series of 31 children with fused ribs and TIS treated with VEPTR
- Spinal deformity controlled and thoracic-spine growth continued at near-normal rates in 30 patients
- Increased hemithorax and total lung volume were maintained at follow-up
- Complications included device migration, infection and brachial plexus palsy
- 28 patients fused before age 9 with minimum 5-year follow-up and pulmonary function testing
- Average forced vital capacity only 57.8% of age-matched normal; FVC under 50% in 12 of 28
- Extent of spine fused correlated inversely with FVC; proximal (T1-T2) fusions did worst
- Patients needing fusion of more than 4 segments, especially with rib anomalies, were at highest risk of restrictive disease
- Systematic review and meta-analysis of 18 studies
- No significant difference in latest-follow-up Cobb angle vs other distraction implants
- Significantly lower complication rate (OR 0.42) and better EOSQ-24 quality-of-life scores with MCGR
- Serum titanium higher with MCGR; MCGR became cost-neutral/cost-effective by ~4 years postoperatively
- Describes the elongation-derotation-flexion (EDF/Cotrel) serial casting technique with modifications
- Serial casting avoided spinal fusion in two-thirds of progressive idiopathic infantile cases
- Argues surgery is not the universal gold standard; casting remains the centerpiece for benign (Mehta) curves
- Success depends on meticulous casting technique under anaesthesia