Chronic Childhood Inflammatory Arthritis
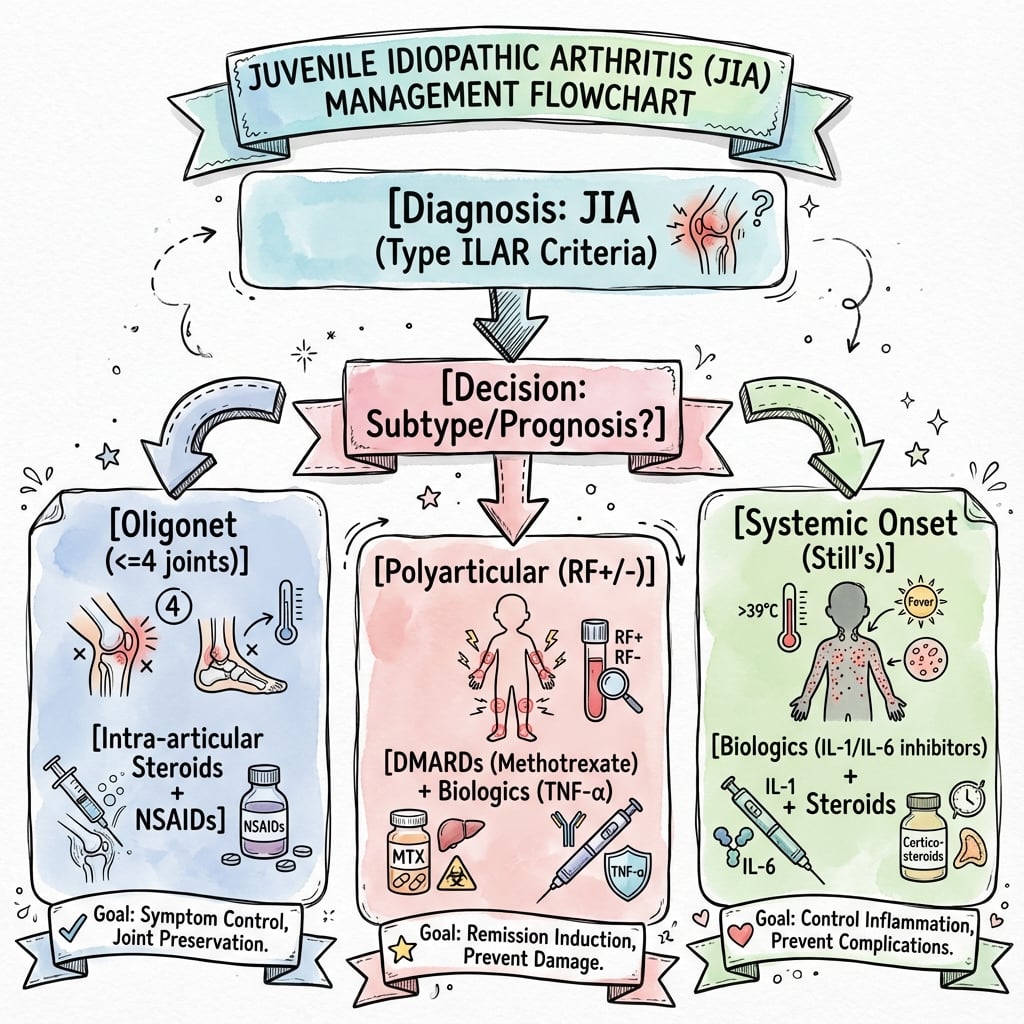
- Oligoarticular: Most common type. 4 or fewer joints.
- Polyarticular: 5 or more joints. More severe.
- Systemic (Still's): Fever, rash, serositis.
- Growth Disturbance: Initial overgrowth, then undergrowth.
- Biologics: Revolutionized medical treatment.
- “Oligoarticular most common
- “Knee overgrowth then undergrowth
- “Biologics are first-line
- “Surgery after medical optimization
JIA causes characteristic growth disturbance in the affected limb.
- Initial: Inflammation → hyperemia → physeal overgrowth (limb lengthening).
- Later: Physeal damage → premature closure → undergrowth (limb shortening).
- Net Effect: Often leg length discrepancy.
- Knee most affected: Valgus deformity common.
- Joints
- ≤4
- Features
- Most common, uveitis risk
- Joints
- ≥5
- Features
- Symmetric, moderate
- Joints
- ≥5
- Features
- Similar to adult RA
- Joints
- Variable
- Features
- Fever, rash, serositis
Overview/Epidemiology
Juvenile Idiopathic Arthritis (JIA) is chronic inflammatory arthritis in children.
- Definition: Arthritis in children under 16, lasting greater than 6 weeks, with no other cause.
- Incidence: 1-4 per 10,000 children.
- Classification: ILAR classification (7 subtypes).
Pathophysiology and Mechanism
Pathophysiology of Joint Damage
- Chronic synovitis leads to pannus formation.
- Pannus erodes cartilage and subchondral bone.
- Joint destruction progresses if inflammation uncontrolled.
Growth Disturbance Mechanism
- Early Phase: Chronic inflammation causes hyperemia around physis.
- Hyperemia increases blood flow → physeal overgrowth → limb lengthening.
- Late Phase: Prolonged inflammation damages physeal chondrocytes.
- Physeal damage → premature closure → limb shortening.
- Net Effect: Often initial lengthening followed by shortening.
Common Joint Involvement
- Knee: Most commonly affected. Valgus deformity, flexion contracture.
- Hip: Flexion-adduction contracture, coxa valga.
- Cervical Spine: C1-C2 instability in severe polyarticular JIA.
Classification Systems
ILAR Classification (International League of Associations for Rheumatology)
- Oligoarticular: ≤4 joints in first 6 months. Most common (50%). Uveitis risk.
- Polyarticular RF-negative: ≥5 joints, RF negative. Moderate severity.
- Polyarticular RF-positive: ≥5 joints, RF positive. Similar to adult RA. Worst prognosis.
- Systemic (Still's Disease): Quotidian fever, salmon-pink rash, hepatosplenomegaly. IL-1/IL-6 driven.
- Enthesitis-Related Arthritis: HLA-B27 associated. Axial involvement. Related to ankylosing spondylitis.
- Psoriatic Arthritis: Arthritis with psoriasis or dactylitis.
- Undifferentiated: Does not fit other categories.
Clinical Assessment
- Joint pain, swelling, stiffness.
- Morning stiffness (improves with activity).
- Systemic symptoms (fever, rash in systemic JIA).
- Eye symptoms (uveitis - especially oligoarticular).
- Joints: Swelling, warmth, effusion, ROM limitation.
- Gait: Antalgic.
- Leg Length: Discrepancy.
- Contractures: Hip, knee flexion.
- Eyes: Refer for slit lamp (uveitis).
Investigations
- ESR, CRP: Elevated.
- ANA: Positive in oligoarticular (uveitis risk).
- RF: Positive in RF+ polyarticular.
- HLA-B27: Enthesitis-related.
- X-ray: Soft tissue swelling, osteopenia, erosions (late).
- MRI: Synovitis, effusion.
Differential Diagnosis
- Distinguishing Features
- Acute, single joint, febrile, elevated WCC
- Distinguishing Features
- Post-infectious, self-limiting
- Distinguishing Features
- Endemic area, tick bite, Borrelia serology
- Distinguishing Features
- Night pain, bone pain, abnormal blood film
- Distinguishing Features
- Hip, resolves within 2 weeks, normal bloods
Management Algorithm
Medical Management
- NSAIDs: First-line for mild disease.
- Intra-articular Steroids: For oligoarticular.
- DMARDs: Methotrexate for polyarticular.
- Biologics: TNF inhibitors (etanercept, adalimumab), IL-1/IL-6 inhibitors for systemic JIA.
- Goal: Remission, prevent joint damage.
Surgical Techniques
Soft Tissue Releases
Indications: Fixed contractures not responding to physio/splinting.
Knee:
- Posterior capsular release.
- Hamstring lengthening.
- Post-op: Aggressive physio, night splinting.
Hip:
- Iliopsoas, rectus, adductor release.
- May need open release for severe contracture.
Complications
- Context
- Oligoarticular, ANA+
- Management
- Regular slit lamp screening
- Context
- Chronic inflammation
- Management
- Control disease, address LLD
- Context
- Uncontrolled synovitis
- Management
- Early biologic therapy
- Context
- Chronic inflammation
- Management
- Physio, splinting, release
- Context
- Severe polyarticular
- Management
- Cervical spine precautions
JIA-Associated Uveitis
The topic flags uveitis as the key extra-articular complication (the OAFY risk factors, slit-lamp referral, "regular screening"), but the nature of the disease and the screening logic are worth developing — it is the single most important reason JIA is co-managed with ophthalmology, and a recurrent exam point.
What it is. The classic JIA-associated eye disease is a chronic anterior uveitis (chronic iridocyclitis), often bilateral. Critically, it is typically asymptomatic and "white" — no pain, redness or photophobia — so the eye looks normal while sight-threatening inflammation progresses silently. This is the opposite of the acute, symptomatic anterior uveitis seen in HLA-B27 enthesitis-related arthritis (a painful red photophobic eye). The asymptomatic nature is exactly why screening, not symptoms, drives detection.
Who is at highest risk (the OAFY card). Young, ANA-positive, oligoarticular girls within the first few years of disease carry the greatest risk; risk is highest early and falls with time, but persists for years and is independent of joint disease activity (the eyes can be inflamed while the joints are quiet).
Screening. Asymptomatic high-risk children need regular slit-lamp examination by ophthalmology, with frequency risk-stratified by subtype, ANA status, age at onset and disease duration — as often as roughly every 3 months in the highest-risk early ANA-positive oligoarticular child, spacing out as risk declines, and continued for years after arthritis settles.
Complications if missed. Posterior synechiae, band keratopathy, cataract, glaucoma, macular oedema and permanent vision loss.
Treatment. Topical corticosteroids plus a mydriatic first; for steroid-dependent or refractory disease, systemic methotrexate and then an anti-TNF biologic. A high-yield distinction: the monoclonal antibodies adalimumab and infliximab are effective for uveitis, whereas etanercept is not — so the choice of biologic is driven partly by eye involvement.
JIA-associated uveitis is chronic anterior, bilateral, asymptomatic and "white" — found by screening, not symptoms (contrast the painful red eye of HLA-B27/ERA). Highest risk: young, ANA-positive, oligoarticular girls, screened by slit lamp as often as every 3 months early on. For refractory disease adalimumab/infliximab work but etanercept does not.
Postoperative Care
- Aggressive Physiotherapy: Essential to maintain gains.
- Splinting: Night splints to prevent recurrence.
- Continue Medical Therapy: Do not stop biologics/DMARDs.
- Rheumatology Co-management: Essential.
- Monitor for Recurrence: Contractures can recur.
Outcomes/Prognosis
- Biologics Era: Dramatically improved outcomes.
- Oligoarticular: Best prognosis.
- RF+ Polyarticular: Worse prognosis, similar to adult RA.
- Systemic: Variable, can be severe.
Guidelines, Registries & Global Practice
Global epidemiology
- JIA is the most common chronic inflammatory rheumatic disease of childhood. Population-based studies show wide variation: incidence roughly 1.6-23 per 100,000/year and prevalence 3.8-400 per 100,000.
- Oligoarticular onset predominates in European/North American cohorts; systemic and polyarticular onset are relatively more common in parts of Asia, Africa and Latin America.
- Female predominance overall (especially ANA-positive oligoarticular and uveitis); enthesitis-related arthritis is more common in older boys.
Major guidelines — side by side
- Scope
- Treatment by disease group + prognostic features
- Core position
- Stepwise escalation: NSAIDs/intra-articular steroid → methotrexate → biologic for poor-prognosis or refractory disease
- Scope
- Points to consider, systemic JIA & non-systemic
- Core position
- Treat-to-target to inactive disease; early biologic in systemic JIA; window-of-opportunity concept
- Scope
- Biologic eligibility & uveitis screening
- Core position
- Structured ophthalmology screening schedule; biologics for inadequate methotrexate response
- Scope
- Classification
- Core position
- Seven-category framework underpinning all guidelines
Registry & long-term data
- Pharmacovigilance registries (e.g. German BiKeR, UK BSPAR-ETN/BCRD, US CARRA Registry, Pharmachild/PRINTO) track biologic safety — malignancy and serious-infection signals have been reassuring at population scale.
- Joint-replacement registries show end-stage arthroplasty for JIA is now uncommon; when performed, survivorship is good but technically demanding (small implants, deformity, osteopenia).
High- vs limited-resource practice variation
- Well-resourced settings: early methotrexate, prompt biologic access, protocolised slit-lamp uveitis screening, MDT (rheumatology, ophthalmology, physiotherapy, orthopaedics, psychology), structured adolescent transition to adult services.
- Limited-resource settings: delayed diagnosis, reliance on NSAIDs/steroids and methotrexate due to biologic cost/availability, higher burden of established deformity, contractures and growth disturbance at presentation — raising the relative role of orthopaedic soft-tissue and reconstructive surgery.
- Universal priorities: control inflammation early, screen the eyes, preserve growth and function, and assess the cervical spine and TMJ before any anaesthetic in polyarticular disease.
Controversies and Areas of Uncertainty
- Classification in flux: A PRINTO consensus is moving toward a biology-based system (e.g. systemic JIA, RF-positive arthritis, enthesitis/spondylitis-related, early-onset ANA-positive arthritis) that may eventually replace the descriptive ILAR categories. Exam answers should acknowledge ILAR as current standard while noting the proposed revision.
- Systemic JIA as an autoinflammatory disease: Increasingly viewed as IL-1/IL-6-driven autoinflammation rather than classic autoimmune arthritis, supporting first-line IL-1/IL-6 blockade and a possible "window of opportunity" for early biologics.
- When to start biologics: Debate between early aggressive biologic use to prevent damage versus a step-up strategy after methotrexate failure, balancing cost, access and long-term safety.
- Treatment de-escalation: Optimal timing and method of tapering biologics after sustained remission remain unresolved; flare risk on withdrawal is significant.
- Surgical timing and choice: Diminishing role of synovectomy and arthroplasty in the biologic era; uncertainty over epiphysiodesis timing for inflammation-driven leg-length discrepancy that may partially self-correct once disease is controlled.
- Macrophage activation syndrome (MAS): A life-threatening complication of systemic JIA; thresholds for diagnosis and the role of anakinra in treatment continue to evolve.
Macrophage Activation Syndrome (MAS)
The controversies section names MAS as the life-threatening complication of systemic JIA but does not develop it — and it is a classic "spot-the-emergency" exam scenario, so it is worth setting out.
What it is. MAS is a form of secondary haemophagocytic lymphohistiocytosis (HLH) — an uncontrolled cytokine storm — that complicates systemic JIA (and adult-onset Still's disease, where the general HLH picture is developed in that topic). It may be the presenting feature or be triggered by infection, a disease flare or a medication change.
Clinical picture. Rapid deterioration: unremitting high fever (losing the quotidian pattern), hepatosplenomegaly, lymphadenopathy, encephalopathy / CNS dysfunction, bleeding and disseminated intravascular coagulation, progressing to multi-organ failure.
Laboratory hallmarks — and the paradoxes that catch people out:
- Markedly elevated ferritin — the hallmark; very high values are a major red flag.
- Falling cell counts — platelets, then white cells and haemoglobin (cytopenias from haemophagocytosis).
- A paradoxically falling ESR — fibrinogen is consumed, so the ESR drops while CRP and ferritin climb. A child who looks "less inflamed" by ESR may actually be deteriorating.
- Low fibrinogen, rising triglycerides, and rising transaminases / LDH (hepatic dysfunction and coagulopathy).
- Bone-marrow haemophagocytosis may be seen but is neither always present nor required for diagnosis.
The 2016 EULAR/ACR/PRINTO classification criteria for MAS in systemic JIA combine a febrile patient with a high ferritin plus two or more of: low platelets, high AST, high triglycerides, low fibrinogen.
Treatment. A medical emergency: high-dose corticosteroids (IV methylprednisolone), ciclosporin, and the IL-1 antagonist anakinra, with intensive-care support. Identify and treat any triggering infection.
In a febrile systemic-JIA child, a sudden fall in ESR with a rising ferritin, falling platelets and rising transaminases is macrophage activation syndrome (secondary HLH) until proven otherwise — not improvement. It is a medical emergency: high-dose steroids, ciclosporin and anakinra.
MCQ Practice Points
Q: What is the most common JIA subtype? A: Oligoarticular (≤4 joints).
Q: What causes initial leg lengthening in JIA? A: Hyperemia from inflammation causes physeal overgrowth.
Q: What eye complication is associated with oligoarticular JIA? A: Uveitis (especially if ANA positive).
Q: Which JIA subtype has the worst prognosis? A: RF-positive polyarticular - similar to adult rheumatoid arthritis.
Q: What is the characteristic rash in systemic JIA? A: Salmon-pink, evanescent rash that appears with fever spikes.
Q: What cervical spine concern exists in polyarticular JIA? A: C1-C2 instability - requires pre-operative assessment before intubation.
Self-Assessment Quiz
At a Glance Table
- Details
- Chronic arthritis in children under 16, lasting over 6 weeks
- Details
- Oligoarticular (4 or fewer joints)
- Details
- Joint inflammation with growth disturbance
- Details
- Initial overgrowth (hyperemia) then undergrowth (physeal damage)
- Details
- Biologics (TNF inhibitors, IL-1/IL-6 blockers)
- Details
- Reserved for refractory contractures or end-stage joints
JIAJIA Types
Hook:OPSEP - Oligo, Poly, Systemic, Enthesitis, Psoriatic.
OUGrowth Changes
Hook:OU - Overgrowth first, Undergrowth later.
OAFYUveitis Risk Factors
Hook:OAFY - Oligo, ANA+, Female, Young.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“10-year-old with oligoarticular JIA affecting the left knee. 3cm left leg lengthening noted.”
“Same patient has a 30-degree knee flexion contracture despite physiotherapy.”
“Teenager with long-standing polyarticular JIA needs tonsillectomy. What are the anaesthetic concerns?”
TYPES
- Oligoarticular (most common)
- Polyarticular RF+/-
- Systemic (Still's)
- Enthesitis-related
GROWTH
- Initial overgrowth (hyperemia)
- Later undergrowth (physeal damage)
- Leg length discrepancy
- Valgus knee common
UVEITIS RISK
- Oligoarticular subtype
- ANA positive
- Female
- Young onset
TREATMENT
- NSAIDs for mild
- DMARDs (methotrexate)
- Biologics (TNF, IL-1/6)
- Physio essential
SURGERY
- After medical optimization
- Contracture release
- Epiphysiodesis for LLD
- Arthroplasty (rare)
CERVICAL SPINE
- C1-C2 instability risk
- Pre-op imaging
- TMJ may limit mouth opening
- Communicate with anaesthesia
Evidence Base
- Landmark double-blind RCT: 69 children with methotrexate-refractory polyarticular JIA
- 74% responded in open-label phase; on withdrawal, disease flare in 28% (etanercept) vs 81% (placebo)
- Median time to flare over 116 days vs 28 days with placebo (less than 0.001)
- Defines the seven mutually exclusive ILAR categories used worldwide
- Arthritis onset under 16 years, persisting over 6 weeks, no other cause
- Categories: oligo (persistent/extended), poly RF-neg, poly RF-pos, systemic, ERA, psoriatic, undifferentiated
- Authoritative review of heterogeneous JIA arthritides of unknown cause
- Prognosis greatly improved by anticytokine agents for conventional-therapy-resistant disease
- Subtype-specific presentation, genetics and outcome
- Post hoc radiographic analysis of two RCTs (systemic and polyarticular-course JIA)
- Wrist/hand films scored by adapted Sharp-van der Heijde and Poznanski methods over 104 weeks
- Most patients showed no structural progression on IL-6 blockade
- Validated criteria for inactive disease, clinical remission on and off medication
- Built from 34-country Delphi survey and chart review of 437 JIA patients
- Patients reaching off-medication remission stayed disease-free longest
- 29 TKAs in 19 patients aged 20 years or younger (JIA the leading diagnosis)
- Implant survivorship 96% at 5 years and 94-95% at 10 years
- TKA volume for inflammatory arthritis has fallen with biologic therapy
- ACR recommendations on initiation and safety monitoring of JIA therapeutics
- Treatment by disease group and prognostic features rather than ILAR category alone
- Escalation to DMARDs/biologics for poor-prognosis or refractory disease
- Standard reference for ILAR classification detail
- Orthopaedic manifestations and growth disturbance
- Multidisciplinary management principles