Age 4-10 Years
- Malignant Progression: Very high risk of becoming severe before skeletal maturity.
- MRI Mandatory: 20% have intraspinal pathology (Arnold-Chiari, Syrinx, Tethered Cord).
- Lung Development: Alveolar multiplication continues until age 8 (avoid early fusion!).
- Casting Limit: Rarely effective after age 4 due to stiffness.
- Treatment Gap: Often requires 'Growth Friendly' surgery (growing rods).
- “Full neurological exam is critical (Abdominal reflexes)
- “Look for cafe-au-lait spots (NF1)
- “Assess flexibility (Bending films)
- “Check lung function (if cooperative)
Juvenile Scoliosis = MRI Spine.
- In Adolescent Idiopathic Scoliosis (AIS), MRI is reserved for "Red Flags".
- In Juvenile Scoliosis, the condition ITSELF is a red flag.
- Approximately 20% of patients with "Idiopathic" Juvenile Scoliosis have a neural axis abnormality (Chiari 1 malformation, Syringomyelia). These require neurosurgical decompression before scoliosis correction.
- Juvenile (4-10)
- High (20%)
- Adolescent (10+)
- Low (2-4%)
- Juvenile (4-10)
- Very High ('Malignant')
- Adolescent (10+)
- Variable (Depends on Risser)
- Juvenile (4-10)
- Female predominance (modest)
- Adolescent (10+)
- Female predominance (marked)
- Juvenile (4-10)
- Moderate (Age 4-8 critical)
- Adolescent (10+)
- Low (Lungs developed)
LPNRRed Flags in Juvenile Scoliosis
Hook:LPN-R (Licensed Practical Nurse - Rapid response).
Overview/Epidemiology
Juvenile Idiopathic Scoliosis (JIS) occupies the age range of 4 to 10 years.
- The "Grey Zone": It exists between the resolving potential of Infantile scoliosis and the predictable patterns of Adolescent scoliosis.
- Epidemiology:
- Accounts for approx 10-15% of all idiopathic scoliosis.
- Female Predominance: Similar to AIS, females are more commonly affected.
- Right Thoracic: The curve pattern begins to resemble AIS (Right sided).
- Malignancy: It is often termed "malignant" because the child has a huge remaining growth potential (the pre-pubertal growth spurt lies ahead). A 30 degree curve at age 5 will almost certainly be greater than 100 degrees by maturity if untreated.
Pathophysiology and Mechanisms
Lung Development
- Alveolar Phase: From birth to age 8, alveoli multiply in number.
- Hypertrophy Phase: After age 8, alveoli increase in size but not number.
- Implication: Early fusion (or severe deformity) before age 8 results in a permanent reduction in alveolar number (True pulmonary hypoplasia). Fusion after age 10 typically has minimal impact on pulmonary function.
Neuroaxis Abnormalities
- Chiari 1 Malformation: Herniation of cerebellar tonsils greater than 5mm.
- Syringomyelia: Fluid filled cyst in the spinal cord.
- Mechanism: The syrinx expands the cord preferentially on one side, damaging the anterior horn cells that innervate the paraspinal muscles. This creates a muscle imbalance that drives the scoliosis.
Classification Systems
Lenke Classification
- While the Lenke classification is designed for AIS, it is often applied to older juvenile patients (age 8-10) to describe the curve pattern.
- Utility is limited because "Triple Major" patterns are less common than long neurological C-curves or simple Thoracic curves.
Clinical Assessment
- Pain: Night pain, back pain. (Red flag for tumor/syrinx).
- Neurology: Headaches? Change in bowel/bladder? (Chiari/Tethered cord).
- Family Hx: Strong scoliosis history.
- Cutaneous Markers: Hairy patches, dimples, hemangiomas.
- Neurology:
- Abdominal Reflexes: Stroking the abdomen should cause umbilicus to deviate towards the stimulus. Asymmetry = Syrinx until proven otherwise.
- Lower Limb: Cavovarus feet (Charcot-Marie-Tooth or Dysraphism).
- Adams Forward Bend Test: Quantify the rib hump (Scoliometer).
Investigations
- PA and Lateral Whole Spine X-ray.
- Supine/Bending Films: To assess flexibility. This determines if bracing is viable (flexible) or if release is needed (stiff).
- MRI Whole Spine: Mandatory for all Juvenile Scoliosis greater than 20 degrees.
- Must image Brainstem to Sacrum.



Differential Diagnosis
A curve presenting in the 4-10 year window is "idiopathic" only after structural, neurological and syndromic causes are excluded. The discriminators below are high-yield in vivas.
- Key Discriminators
- Flexible, no congenital anomaly, normal neurology, right thoracic pattern emerging
- Decisive Test
- Diagnosis of exclusion after normal MRI
- Key Discriminators
- Left thoracic curve, asymmetric/absent abdominal reflexes, cavovarus feet, pain
- Decisive Test
- Whole-spine MRI
- Key Discriminators
- Short, sharp, rigid curve; failure of formation/segmentation; possible VACTERL
- Decisive Test
- Plain films plus CT; renal/cardiac screen
- Key Discriminators
- Cafe-au-lait spots/dystrophic curve (NF1), arachnodactyly (Marfan), disproportion
- Decisive Test
- Genetic/clinical phenotyping, MRI
- Key Discriminators
- Painful, rapidly progressive, night pain, constitutional symptoms, rigid
- Decisive Test
- MRI plus inflammatory markers
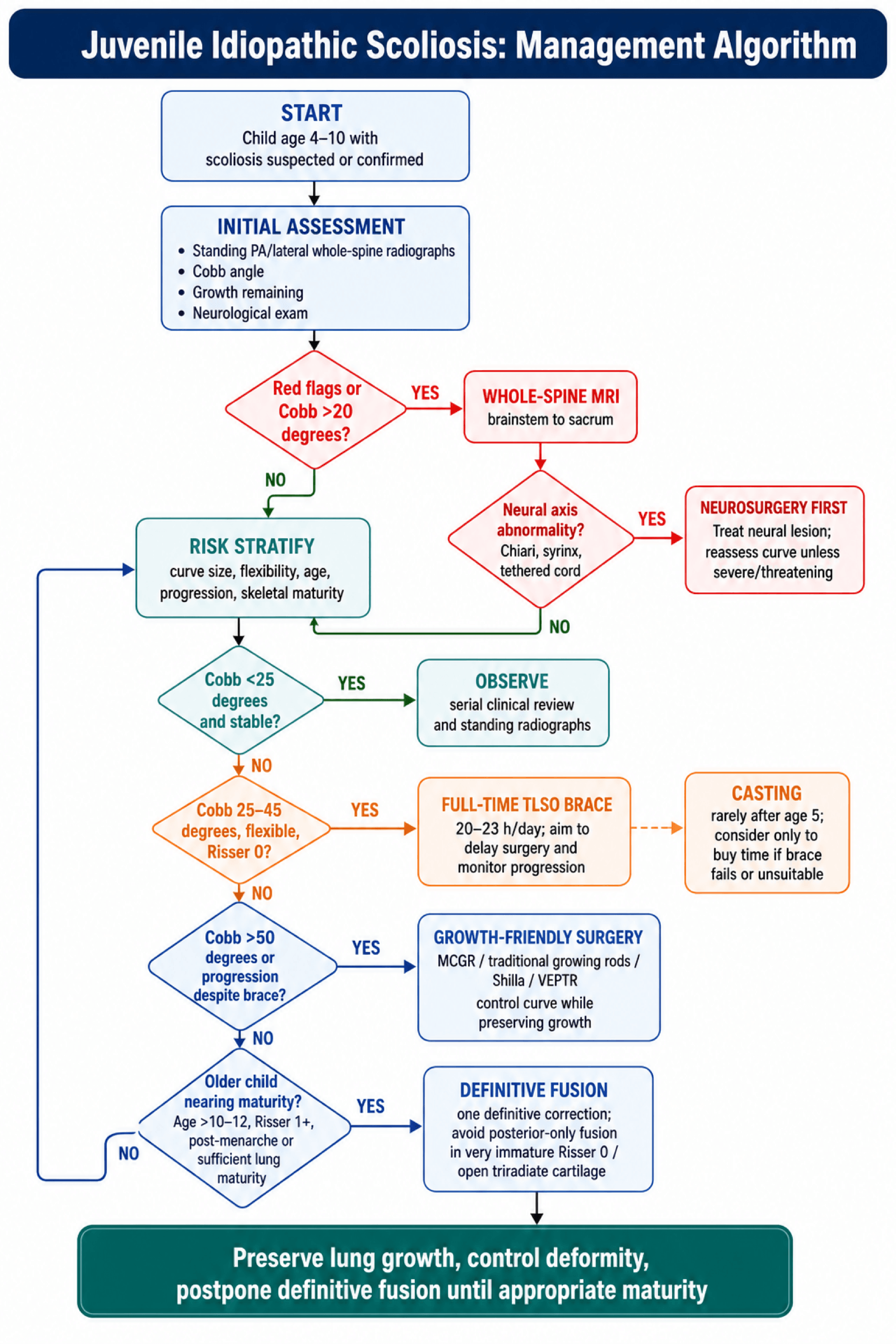
Management Algorithm
1. Bracing (TLSO)
- Indication: Curves 25-45 degrees, Risser 0, Flexible.
- Efficacy: Less effective than in AIS. "Part-time" bracing (night only) is useless. Requires 20-23 hours/day.
- Goal: Delay surgery. Usually cannot prevent surgery eventually, but delays it until age 10-12 (lung maturity).
2. Casting
- Indication: Rarely used after Age 5. Useful if failing brace to "buy time".
PPPGoals of Treatment
Hook:Triple P.
Timing Spinal Surgery After Neuraxis Decompression
Because roughly one in five juvenile curves harbours a Chiari, syrinx or tethered cord that should be treated first, a recurring question (posed directly in the viva) is how long to wait before instrumenting the spine.
- Decompress first, then reassess. When a neural-axis lesion is found, the neurosurgical procedure (foramen-magnum decompression for Chiari, cord detethering, or syrinx drainage/shunt) is generally performed before any scoliosis correction, because operating on a cord that is under tension or contains a syrinx risks neurological injury.
- Allow time for the curve to respond. After decompression the scoliosis may stabilise or partially improve, particularly in younger children with smaller, flexible curves, so a period of observation (commonly around 3-6 months, with interval radiographs) is used to see whether the curve settles before committing to instrumentation.
- Then treat the residual curve on its own merits. If the curve continues to progress or remains large despite decompression, proceed with the age-appropriate scoliosis treatment (brace, growth-friendly surgery, or fusion) — the neural axis having been made safe first.
- A monitoring caveat. Metallic growing-rod constructs create MRI artefact that hampers later syrinx surveillance, so the neural axis should be clarified and, where possible, addressed before definitive metalwork is placed. (Detail of each lesion sits in the Chiari, syringomyelia and tethered-cord topics.)
Q: A juvenile curve has a Chiari/syrinx on MRI — do you instrument the spine, and when? A: Treat the neural-axis lesion first (decompression/detethering), then observe the curve for roughly 3-6 months: it may stabilise or improve, avoiding or delaying spinal surgery. Instrument only the curve that still progresses or remains large afterwards. Clarify/address the syrinx before placing MRI-artefact-producing metalwork.
Surgical Techniques
Growing Rods (MCGR)
- Technique: Proximal anchors (T2/3 hooks/screws) and Distal anchors (L3/4 screws). Submuscular rods.
- Magnet: External magnet lengthens the rod 3-5mm every 3 months in clinic.
- Advantage: Avoids "Law of Diminishing Returns" (spontaneous autofusion from repeated open surgeries).
- Disadvantage: Metal artifact on MRI (makes monitoring syrinx difficult). Cost.
GSVTSurgical Options
Hook:GSVT (Great Spines Very Tall).
VEPTR and Thoracic Insufficiency Syndrome
The surgical-options list and the management algorithm both name VEPTR, and the must-know points repeatedly warn about thoracic insufficiency syndrome (TIS) — the two are linked and deserve explicit definition alongside the growing-rod, Shilla and VBT options above.
- Thoracic insufficiency syndrome (TIS). Defined by Campbell as the inability of the thorax to support normal respiration or lung growth. A short, stiff, deformed thorax (from a severe early curve, fused/absent ribs, or early spinal fusion) cannot expand, so the underlying lung cannot grow — the reason this whole topic stresses preserving thoracic height and avoiding early definitive fusion. It is assessed clinically (chest excursion, the thumb-excursion test of hemithorax expansion) and radiographically (space available for lung).
- VEPTR (Vertical Expandable Prosthetic Titanium Rib). Campbell's rib-based distraction device, anchored rib-to-rib (and rib-to-spine or rib-to-pelvis), designed to expand the thorax directly rather than only correct the spinal curve, and periodically lengthened as the child grows.
- Where VEPTR fits. Its classic indication is TIS with a chest-wall abnormality — fused ribs with congenital scoliosis, or other conditions where the thorax itself is deficient — rather than a purely spinal idiopathic curve, for which spine-based growing rods (MCGR) or the other options above are usually preferred.
- Shared limitation. Like all distraction-based systems it is subject to the law of diminishing returns (repeated lengthenings, autofusion) and to device/wound complications. The broader early-onset-scoliosis picture is developed in that topic.
Q: What is thoracic insufficiency syndrome, and which device was designed to treat it? A: TIS is the inability of the thorax to support normal respiration or lung growth (Campbell) — the endpoint the "avoid early fusion" and "preserve lung growth" rules exist to prevent. VEPTR, a rib-based expandable titanium device, was designed to expand a deficient thorax directly, classically for TIS with chest-wall/rib anomalies rather than a purely spinal idiopathic curve.
Complications
- Rate
- High
- Prevention/Management
- MCGR rods jam. Anchors pull out.
- Rate
- Moderate
- Prevention/Management
- Increased with multiple surgeries (less with MCGR).
- Rate
- Common
- Prevention/Management
- Proximal Junctional Kyphosis. Avoid stopping at kyphotic apex.
- Rate
- Unknown
- Prevention/Management
- Titanium debris from sliding rods (Shilla).
- Rate
- Rare
- Prevention/Management
- Monitor cord during lengthening.
Postoperative Care
- Bracing: Most growing rod patients require a brace post-op to protect the proximal anchors.
- Activity: Restricted contact sports.
- Lengthening: Strict adherence to lengthening schedule (usually every 3 months for MCGR).
Outcomes/Prognosis
- Untreated: Severe disability, restrictive lung disease, Cor Pulmonale.
- Treated:
- Most require definitive fusion at maturity.
- Goal is a "straight-ish" spine with adequate lung strings.
- Final height is usually short (short trunk), but functional.
- Pain: Adults with treated JIS have higher rates of back pain than AIS patients.
Guidelines, Registries & Global Practice
Global epidemiology
- Juvenile-onset (age 4-10) accounts for roughly 10-15% of all idiopathic scoliosis; infantile, juvenile and adolescent together form the "early-onset" (under age 10) spectrum that carries the highest pulmonary and progression risk.
- Female predominance increases with age at onset; the curve pattern transitions toward the adolescent right-thoracic pattern by the upper juvenile age range.
Society guidance — side by side
- Position relevant to juvenile / early-onset scoliosis
- Whole-spine MRI for early-onset and atypical curves; growth-friendly instrumentation (MCGR, traditional dual rods) preferred over early definitive fusion; C-EOS used for risk stratification.
- Position relevant to juvenile / early-onset scoliosis
- Specialist paediatric spinal MDT review; MRI before any intervention in young-onset curves; serial low-dose imaging to limit cumulative radiation.
- Position relevant to juvenile / early-onset scoliosis
- Endorses growth-sparing surgery to protect thoracic and pulmonary development; emphasises avoidance of repeated open lengthenings.
- Position relevant to juvenile / early-onset scoliosis
- Provides conservative-management (bracing / scoliosis-specific exercise) consensus; bracing in young-onset curves aims to delay surgery rather than guarantee avoidance.
Registry & device notes
- MCGR adoption was tempered worldwide by reports of metallosis and limited true distraction over time; several registries and national bodies (including UK device alerts) prompted closer surveillance and explant analysis.
- Vertebral body tethering carries device-specific regulatory status that differs by region (e.g. US FDA Humanitarian Device Exemption), and is offered selectively within specialist centres.
High- vs limited-resource practice
- Well-resourced settings: routine whole-spine MRI, EOS or other low-dose biplanar imaging for serial monitoring, MCGR and VBT availability, neuromonitoring for instrumented correction.
- Limited-resource settings: later presentation with larger, stiffer curves; greater reliance on bracing, casting and definitive fusion; halo-gravity traction used to reduce neurological risk when advanced imaging or neuromonitoring is unavailable.
- Radiation stewardship is universal: cumulative imaging over years of growth raises breast-tissue dose concerns, so low-dose biplanar systems and limited-frequency radiography are recommended wherever available.
Deep Dive: The Crankshaft Phenomenon
Definition: Progressive rotational and angular deformity that occurs after posterior fusion in skeletal immature patients.
Mechanism:
- Posterior elements are fused (tethered).
- Anterior vertebral bodies (neurocentral synchondrosis) continue to grow.
- Result: The spine bulges anteriorly and twists (rotates) around the posterior tether.
Prevention:
- In Risser 0 patients with open triradiate cartilage (Age less than 10), posterior fusion ALONE is contraindicated.
- Must perform Anterior and Posterior Fusion (circumferential) to stop all growth plates if definitive fusion is chosen.
The Law of Diminishing Returns With traditional distraction-based surgery (TGR):
- Every time you operate to lengthen the rods, the spine scars and stiffens ("Auto-fusion").
- The amount of length gained per surgery decreases over time.
- By the 5th or 6th lengthening, the spine may be completely stiff, yielding zero length gain, but all the risks of surgery remain.
- Solution: Minimise interventions (use MCGR) or delay initial implantation as long as possible.
Controversies & Areas of Uncertainty
- VBT durability: Vertebral body tethering offers fusionless correction but carries high reoperation rates (tether rupture, overcorrection). Long-term curve behaviour into adulthood and ideal patient selection remain unresolved.
- MCGR longevity and metallosis: Magnetically controlled rods reduce open lengthenings, but real-world distraction falls short of predicted gains over time and explant studies show titanium/metal wear debris (metallosis). The optimal lengthening frequency and total service life are debated, and device alerts have prompted closer surveillance.
- Bracing efficacy in JIS: Bracing can alter natural history and buy time, but it rarely prevents surgery in larger juvenile curves. The threshold and protocol (full-time versus night-time bending brace) are not standardised for this age group.
- When to obtain MRI: Universal MRI in juvenile curves is widely endorsed given the roughly 18-20% neural axis yield, yet cost-effectiveness, sedation risk in young children, and exactly which lower-magnitude curves warrant imaging are still discussed.
- Timing of definitive fusion: Balancing crankshaft and progression risk against pulmonary and spinal-height loss means the "right age" to convert from growth-friendly to definitive fusion is individualised, not fixed.
- Crankshaft relevance in the implant era: With modern segmental pedicle-screw constructs, the true incidence and clinical significance of the crankshaft phenomenon after posterior-only fusion is less certain than in the historical hook-and-wire literature.
Deep Dive: Vertebral Body Tethering (VBT)
The New Kid on the Block VBT is a "growth modulation" technique (like 8-plates for knees).
- Indication: Skeletally immature (Risser 0-2), Flexible curve, Age 8-12.
- Mechanism: Screws placed laterally in vertebral bodies on the convex side. A flexible polyethylene cord connects them. Tension is applied.
- Result: Compression of the convex growth plate slows growth. Concave side keeps growing. The spine straightens as the child grows.
- Controversy: High revision rate (tether rupture, over-correction). Long term results unknown. FDA approved (HDE) but still considered "innovative" in many guidelines.
MCQ Practice Points
Q: At what age does the risk of true pulmonary hypoplasia (loss of alveolar number) significantly decrease? A: Age 8. Fusion after age 8 generally affects lung volume (size) but not alveolar count.
Q: What is the most common cause of growing rod failure? A: Anchor failure (Hook/Screw pullout) or Rod Fracture.
Q: What clinical sign is most specific for a syrinx in a child with scoliosis? A: Absent abdominal reflexes. (Asymmetrical superficial abdominal reflex).
Q: A 5-year-old has a 60 degree congenital scoliosis (Unilateral unsegmented bar with contralateral hemivertebra). Treatment? A: Fusion. Congenital curves DO NOT respond to bracing. A short fusion of the congenital anomaly is required to stop the "evil" growth mismatch. Growing rods are for long curves (idiopathic/NM).
Q: What percentage of patients with juvenile idiopathic scoliosis have a neural axis abnormality (Chiari/Syrinx) on MRI? A: Approximately 20%. This is why MRI is mandatory for all juvenile scoliosis patients.
Self-Assessment Quiz
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“6-year-old female. Right Thoracic curve 35 degrees. MRI is normal. Risser 0.”
“8-year-old male. Left Thoracic curve. MRI shows a large thoracic syrinx.”
“A 9-year-old underwent posterior fusion for severe scoliosis 2 years ago. Now the deformity is recurring and she is twisting.”
BASICS
- Age 4-10
- High Progression
- MRI Mandatory
- The Grey Zone
RED FLAGS
- Left curve
- Pain
- Neuro Signs
- Rapid Increase
THE LUNGS
- Alveoli Age 8
- TIS Risk
- Avoid Early Fusion
- Volume is Life
SURGERY
- Growing Rods
- Shilla
- Tethering (VBT)
- Delay Fusion
Evidence Base
- 109 consecutive juvenile idiopathic scoliosis patients (67 girls, 42 boys; mean age 6 years 10 months)
- 104 of 109 curves were progressive; only 5 (5%) resolved spontaneously
- Progression was 1 to 3 degrees per year before age 10, accelerating to 4.5 to 11 degrees per year after age 10
- Single/double mid-thoracic curves (Groups 1 and 2) carried the worst prognosis; thoracolumbar and lumbar curves (Groups 3 and 4) were more benign
- Largest MRI series of 'presumed idiopathic' infantile/juvenile scoliosis (n=504)
- Neural axis abnormality found in 94 patients (18.7%); Arnold-Chiari with/without syringomyelia accounted for 64.8% of these
- Male sex, left thoracic curve and right lumbar curve were independently associated with intraspinal pathology
- Confirms a routine whole-spine MRI is warranted in scoliosis presenting before age 10
- Systematic review of early-onset scoliosis treated by definitive fusion
- Restrictive pulmonary disease (FVC less than 50% predicted) occurred in 43% to 64% of patients fused young
- Extensive and proximal thoracic fusions carried the highest pulmonary risk
- Post-fusion thoracic growth averaged only 50% of that in non-fused scoliotic children; reduced thoracic height correlated with reduced FVC
- Multicenter Growing Spine Study Group; 140 patients, 897 growing-rod procedures
- 81 patients (58%) sustained at least one complication
- Complication risk rose 24% with every additional surgical procedure and fell 13% for each year initial implantation was delayed
- Dual rods and submuscular placement reduced implant and wound complications versus single/subcutaneous rods
- Prospective multicenter series of MCGR with outpatient, anaesthesia-free distractions
- Mean Cobb angle corrected from 60 to 34 degrees after index surgery, maintained at 31 degrees at follow-up
- Dual rods achieved greater spinal height gain than single rods (T1-S1: 3.09 vs 1.27 mm/month)
- No neurological deficit or implant failure during early follow-up
- Prospective case series introducing the magnetically controlled growing rod (5 patients)
- In the 2 patients with 24-month follow-up, mean Cobb angle fell from 67 to 29 degrees
- Each non-invasive monthly distraction lengthened the instrumented segment by approximately 1.9 mm
- No MCGR-related complications; improved quality-of-life and cost-effectiveness versus traditional growing rods
- Retrospective review of JIS treated with a nighttime bending brace (curves over 20 degrees, Risser 0)
- 19 of 37 curves (51%) were successfully managed in-brace; 7 patients ultimately required fusion
- Success correlated with greater in-brace correction rather than initial curve magnitude
- Part-time bracing performed better than the natural history with psychosocial/compliance advantages
- First clinical cohort of anterior VBT in skeletally immature idiopathic scoliosis (11 patients)
- Thoracic Cobb angle corrected from 44 to 13.5 degrees (70% correction) over 2 years via growth modulation
- Axial trunk rotation improved from 12.4 to 6.9 degrees; no major complications
- 2 of 11 patients returned to theatre for tether loosening to prevent overcorrection