NF1 Orthopaedic Challenges
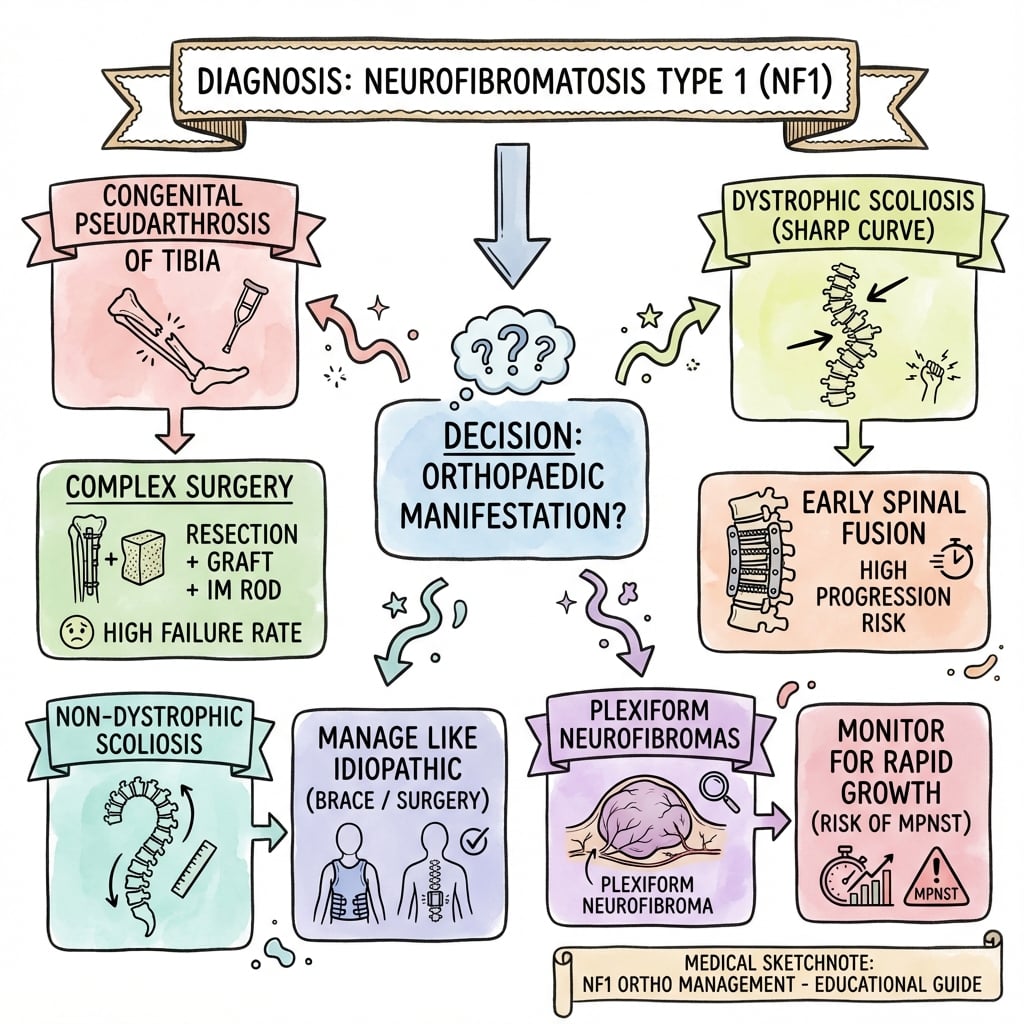
- Dystrophic Scoliosis: Sharp, angular curve with poor prognosis.
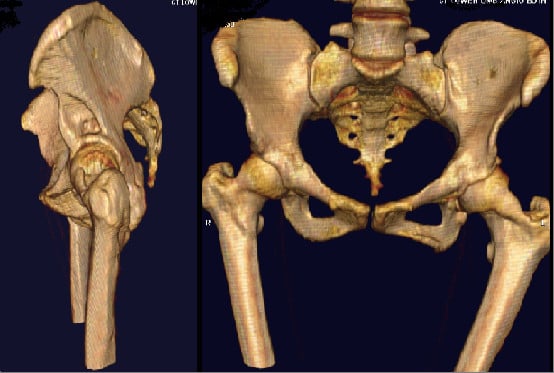
- Tibial Dysplasia: Anterolateral bowing → pseudarthrosis risk.
- Cafe-au-lait Spots: greater than 6 spots greater than 5mm (prepubertal).
- NF1 Gene: Tumor suppressor (neurofibromin).
- Surgery is challenging: High failure rates.
- “Dystrophic vs non-dystrophic scoliosis
- “Anterolateral tibial bowing
- “6 cafe-au-lait spots diagnostic
- “NF1 is a tumor suppressor
Dystrophic scoliosis in NF1 has a POOR prognosis.
- Features: Short segment, sharp angular curve, vertebral scalloping, rib penciling, dural ectasia.
- Progresses rapidly, even after fusion.
- Early combined (anterior + posterior) fusion may be needed.
- Monitor closely.
- Dystrophic
- Short, sharp, angular
- Non-Dystrophic
- Similar to idiopathic
- Dystrophic
- Scalloping, wedging, rotation
- Non-Dystrophic
- Minimal
- Dystrophic
- Poor - rapid progression
- Non-Dystrophic
- Better - like idiopathic
- Dystrophic
- Early combined fusion
- Non-Dystrophic
- Standard scoliosis Rx
SSRDDystrophic Scoliosis Features
Hook:SSRD - Sharp, Scalloping, Rib, Dural.
HARDNF1 Surgery Challenges
Hook:NF1 surgery is HARD - plan for complications and counsel families accordingly!
Overview/Epidemiology
Neurofibromatosis Type 1 (NF1) is a common genetic disorder.
- Genetics: Autosomal dominant. NF1 gene on chromosome 17 (encodes neurofibromin, a tumor suppressor).
- Incidence: 1 in 3,000.
- 50% new mutations: Often no family history.
- Key Features: Cafe-au-lait spots, neurofibromas, Lisch nodules.
- Malignancy Risk: 8-13% lifetime risk of malignant peripheral nerve sheath tumor (MPNST).
Pathophysiology, Anatomy & Pathomechanics
NF1 Gene Function
- Neurofibromin is a tumor suppressor (Ras-GAP).
- Loss leads to uncontrolled cell proliferation (neurofibromas).
- Affects Schwann cells, melanocytes, bone.
Why Scoliosis in NF1?
- Dystrophic features suggest mesodermal dysplasia.
- Vertebral scalloping from dural ectasia and abnormal bone.
- Non-dystrophic curves likely from neurofibromas affecting paraspinal muscles.
Why Tibial Pseudarthrosis?
- Local mesodermal defect in tibial periosteum/bone.
- Reduced blood supply and poor bone healing.
- Anterolateral bowing progresses to fracture and non-union.
Classification Systems
Crawford Classification (Tibial Dysplasia)
- Type I: Anterolateral bowing with increased cortical density.
- Type II: Anterolateral bowing with sclerotic medullary canal.
- Type III: Anterolateral bowing with cystic lesion.
- Type IV: Anterolateral bowing with frank fracture/pseudarthrosis.
Prognosis: Types III and IV have worst outcomes.
Clinical Assessment
- ≥6 cafe-au-lait spots (≥5mm prepubertal, ≥15mm postpubertal).
- ≥2 neurofibromas or 1 plexiform neurofibroma.
- Freckling in axillary or inguinal region.
- Optic glioma.
- ≥2 Lisch nodules.
- Bony lesion (sphenoid dysplasia, tibial dysplasia).
- First-degree relative with NF1.
- Skin: Cafe-au-lait spots, neurofibromas, freckling.
- Spine: Scoliosis assessment.
- Lower Limbs: Tibial bowing.
- Eyes: Slit lamp for Lisch nodules.
The 2021 Revised Diagnostic Criteria
The criteria listed above are the classic 1988 NIH set, and the Guidelines section notes a 2021 international revision — worth setting out, because it is the current standard and a recurring exam update.
What the 2021 revision added to the seven NIH criteria:
- Two or more choroidal anomalies — bright, patchy nodules seen on near-infrared reflectance imaging or OCT of the fundus (a new, fairly specific sign).
- A heterozygous pathogenic NF1 variant with a variant allele fraction of around 50 percent in apparently normal tissue (e.g. leukocytes) — i.e. a confirmed constitutional NF1 mutation now counts as a diagnostic criterion in its own right.
The decision rule was also formalised: in a person with no parent meeting the criteria, two or more criteria are required; in a child with an affected parent, one criterion suffices. The café-au-lait and freckling definitions were tightened (count, size, and intertriginous distribution).
The caveat that matters most clinically (and links to the differential below): a young child whose ONLY features are café-au-lait macules plus intertriginous freckling — especially with a normal NF1 genetic test — should prompt consideration of Legius syndrome (SPRED1), which shares the pigmentary signs but lacks neurofibromas, Lisch nodules, optic glioma and the skeletal and malignant complications. Distinguishing them changes prognosis and the entire surveillance pathway, so genetic testing is the discriminator.
The 2021 revision adds two or more choroidal anomalies and a constitutional pathogenic NF1 variant to the 1988 NIH list, and formalises the rule: two criteria if no affected parent, one if a parent has NF1. If a child has only café-au-lait macules and freckling, think Legius syndrome (SPRED1) and test — it lacks the neurofibromas, Lisch nodules and bony/tumour complications that drive NF1 surveillance.
NF1NF1 Diagnostic Criteria
Hook:CFNOLBR - 2 or more criteria.
Investigations
- NF1 mutation testing (available but not always needed for clinical diagnosis).
- Spine X-ray: Scoliosis, vertebral changes.
- MRI Spine: Pre-op for scoliosis (dural ectasia, intraspinal neurofibromas).
- Lower Limb X-ray: Tibial bowing.
- MRI Brain: Optic pathway glioma screening.
- Slit lamp for Lisch nodules.

Dural Ectasia in NF1
Dural ectasia is invoked throughout this topic — in the dystrophic-feature lists, as a reason for pre-operative MRI, and as an intra-operative challenge — but it is worth explaining, because it is the single pathology that underlies most of the "dystrophic" radiographic signs and most of the surgical difficulty.
What it is. Dural ectasia is a progressive circumferential dilatation of the dural sac. It is a hallmark dystrophic feature of NF1 (and is also seen in Marfan and Ehlers-Danlos syndromes, covered in their own topics) and is thought to arise from a combination of mesodermal dysplasia of the dura and chronic cerebrospinal-fluid pulsation against a structurally weak dura.
Why the "dystrophic features" are really dural ectasia. The expanding dura erodes the surrounding bone, producing the classic signs:
- Posterior vertebral body scalloping (the dura pressing on the back of the vertebral body).
- A widened interpedicular distance and enlarged spinal canal.
- Enlarged, scalloped neural foramina and spindled (thinned) transverse processes and pedicles.
- Frank lateral (thoracic) meningoceles — out-pouchings of dura herniating through the widened foramina.
MRI best demonstrates the dilated thecal sac and meningoceles; CT shows the bony erosion.
Why it matters surgically (the punchline). The same ectasia that scallops the bone leaves thin, dysplastic, eroded pedicles and a dilated, attenuated dura, so:
- Pedicle-screw purchase is poor and screws can breach into the enlarged canal — a major reason instrumentation fails.
- Lateral meningoceles and a thinned dura raise the risk of dural tear and CSF leak.
- Together these drive the high implant-failure and pseudarthrosis rates that make dystrophic curves so difficult — which is exactly why a pre-operative MRI is mandatory and why many surgeons add anterior-column support. (Scoliosis instrumentation technique is developed in the scoliosis topics.)
Dural ectasia is the circumferential dilatation of the dural sac behind the classic dystrophic signs — posterior vertebral scalloping, a widened canal and foramina, thin spindled pedicles, and lateral meningoceles. It is why pre-operative MRI is mandatory and why dystrophic curves fail: thin pedicles give poor screw purchase, the attenuated dura tears easily, and pseudarthrosis rates are high.
Differential Diagnosis
Cafe-au-lait Spots and Related Conditions:
- Key Features
- Multiple CAL spots, neurofibromas
- Differentiator
- NIH criteria, Lisch nodules
- Key Features
- Bilateral acoustic neuromas
- Differentiator
- Different gene (NF2), no CAL spots
- Key Features
- CAL spots, polyostotic FD
- Differentiator
- Coast-of-Maine borders, precocious puberty
- Key Features
- CAL spots, freckling
- Differentiator
- No neurofibromas, SPRED1 mutation
- Key Features
- CAL spots
- Differentiator
- Short stature, cardiac defects
Key Distinguishing Points:
- NF1 vs NF2: NF1 has CAL spots and peripheral neurofibromas; NF2 has acoustic neuromas
- NF1 vs McCune-Albright: NF1 has smooth-bordered CAL spots; McCune-Albright has "coast of Maine" irregular borders
- NF1 vs Legius: Very similar but Legius lacks neurofibromas (SPRED1 mutation)
Management Algorithm
Dystrophic Scoliosis
- Bracing: Limited effect.
- Surgery: Early combined (anterior + posterior) fusion for curves greater than 20-25 degrees because of rapid progression.
- Pre-op MRI: Exclude intraspinal pathology (dural ectasia, neurofibromas).
BIVATibial Dysplasia Management
Hook:BIVA - Brace, Ilizarov, Vascularized graft, Amputation.
Surgical Techniques
Combined Anterior-Posterior Fusion
Indications: Dystrophic scoliosis with curves greater than 20-25 degrees.
Technique:
- Anterior release and fusion.
- Posterior instrumented fusion.
- Address dural ectasia intra-op.
Challenges: High pseudarthrosis rate, dural ectasia, thin pedicles.
Complications
- Context
- Post-scoliosis surgery
- Management
- Combined fusion, revision
- Context
- Multiple surgeries
- Management
- Ilizarov, amputation if fails
- Context
- Despite fusion
- Management
- Revision, extend fusion
- Context
- Plexiform neurofibroma
- Management
- Oncology, wide excision
- Context
- Scoliosis surgery
- Management
- Primary repair
Postoperative Care
- Scoliosis: Bracing post-op, close follow-up for pseudarthrosis.
- Tibial Surgery: Protected weight-bearing, external fixator care.
- All Patients: Long-term surveillance for malignancy.
Outcomes/Prognosis
- Dystrophic Scoliosis: Challenging. High failure rate even with combined fusion.
- Tibial Pseudarthrosis: Healing is difficult. Multiple surgeries often needed.
- Life Expectancy: Reduced due to malignant transformation (MPNST), other complications.
Guidelines, Registries & Global Practice
Global epidemiology
- NF1 affects roughly 1 in 2,500-3,000 births worldwide with no major ethnic or geographic variation — it is one of the most common single-gene disorders.
- About half of cases are de novo mutations, so a negative family history is common.
- Scoliosis is the commonest skeletal manifestation (around 10-30%); congenital pseudarthrosis of the tibia is rare but disproportionately associated with NF1 (NF1 implicated in roughly half of all cases, Hefti EPOS series).
Side-by-side guidance
- Focus
- Clinical diagnosis
- Practical emphasis
- Two or more of the seven criteria; the 2021 international revision added the choroidal anomaly and an NF1 pathogenic variant as criteria
- Focus
- Diagnosis + lifelong surveillance
- Practical emphasis
- Structured monitoring of spine, optic pathway and MPNST; multidisciplinary clinics
- Focus
- Dystrophic scoliosis
- Practical emphasis
- Pre-operative MRI mandatory; early instrumented fusion for dystrophic curves; growth-friendly constructs in the very young
- Focus
- Tibial dysplasia
- Practical emphasis
- Protect with bracing until union attempted; combine biological (vascularized fibula, autograft, BMP) and mechanical (intramedullary rod, Ilizarov) strategies
Registry and surveillance notes
- There is no single global NF1 implant registry, but national NF registries (e.g. UK regional registers used by Evans et al) provide the population-level MPNST and cancer-risk data.
- Spinal deformity and limb-reconstruction outcomes are tracked through specialist paediatric spine and pseudarthrosis databases rather than arthroplasty registries.
High- vs limited-resource practice variation
- Well-resourced settings: genetic confirmation, MRI surveillance, MEK inhibitors (e.g. selumetinib) for symptomatic inoperable plexiform neurofibromas, and microvascular fibular transfer for tibial pseudarthrosis.
- Limited-resource settings: diagnosis remains clinical (NIH criteria), surveillance is examination-based, and tibial reconstruction relies more on Ilizarov/autograft techniques; refractory cases more often proceed to amputation and prosthetic fitting.
- Universal principles: multidisciplinary care (genetics, neurology, orthopaedics, ophthalmology, dermatology, oncology) and a low threshold for sarcoma-MDT referral when a lesion enlarges or becomes painful.
Controversies & Areas of Uncertainty
- Timing of dystrophic curve surgery: Most agree dystrophic curves need early instrumented fusion, but the threshold (Cobb angle, age, degree of modulation) and whether to perform combined anterior-posterior versus posterior-only with modern pedicle-screw constructs remain debated.
- Combined vs posterior-only fusion: Historically combined fusion was standard for high pseudarthrosis rates; modern segmental instrumentation has led some centres to favour posterior-only, though dural ectasia, thin dystrophic pedicles and bone quality still drive failures.
- Best biology for tibial pseudarthrosis: No technique reliably prevents refracture. Vascularized fibula, Ilizarov, intramedullary rodding, autograft and BMP are all used, often in combination; the optimal sequence is unsettled and recurrence to skeletal maturity is the rule rather than the exception.
- Role of BMP: Bone morphogenetic protein is used off-label as an adjunct in congenital pseudarthrosis, but evidence is low-level and theoretical oncological concerns in a tumour-predisposition syndrome are unresolved.
- MEK inhibitors and bone: Selumetinib transformed management of inoperable plexiform neurofibromas; whether MEK-pathway modulation can aid bone healing in pseudarthrosis is an active research question.
- Surveillance intensity for MPNST: Whole-body MRI and FDG-PET can detect malignant transformation early, but cost, radiation and false positives mean there is no universal consensus on routine imaging surveillance versus symptom-triggered investigation.
MCQ Practice Points
Q: What gene is mutated in NF1? A: NF1 gene on chromosome 17 (neurofibromin).
Q: What type of scoliosis has a poor prognosis in NF1? A: Dystrophic scoliosis (short, sharp, angular).
Q: What tibial deformity is associated with NF1? A: Anterolateral bowing with risk of pseudarthrosis.
Q: What malignancy are NF1 patients at risk for? A: MPNST (malignant peripheral nerve sheath tumor) - 8-13% lifetime risk. Arises from plexiform neurofibromas.
Q: What is the Crawford classification for? A: Tibial dysplasia in NF1. Types I-IV based on bowing characteristics and presence of fracture/pseudarthrosis.
Q: What eye finding is seen in NF1? A: Lisch nodules (iris hamartomas) - seen on slit lamp exam.
Self-Assessment Quiz
Additional Quiz Questions
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“12-year-old with NF1 has a 30-degree thoracic curve with vertebral scalloping and rib penciling on X-ray.”
“6-month-old with NF1. X-ray shows anterolateral bowing of the tibia.”
“25-year-old with NF1 presents with rapid growth and pain in a previously stable plexiform neurofibroma on the thigh.”
GENETICS
- NF1 Gene
- Chromosome 17
- Autosomal Dominant
- Tumor suppressor
DIAGNOSIS
- ≥6 cafe-au-lait spots
- Neurofibromas
- Lisch nodules
- Tibial dysplasia
SCOLIOSIS
- Dystrophic = poor prognosis
- Sharp angular curve
- Combined fusion
- Non-dystrophic = better
TIBIA
- Anterolateral bowing
- Pseudarthrosis risk
- Brace to protect
- Ilizarov if fractured
DYSTROPHIC FEATURES
- Vertebral scalloping
- Rib penciling
- Dural ectasia
- Spindling TP
MALIGNANCY
- MPNST 8-13% risk
- Arises from plexiform
- Rapid growth = concern
- Wide excision
Evidence Base
- Foundational review describing the spectrum of skeletal NF1 (scoliosis, kyphosis, tibial pseudarthrosis, sphenoid dysplasia)
- Source of the Crawford classification of anterolateral tibial bowing / congenital pseudarthrosis
- Distinguishes dystrophic from non-dystrophic spinal deformity
- 91 NF1 patients: deformities 'modulate', acquiring dystrophic features over time, so the dystrophic/non-dystrophic label is not fixed
- Curves diagnosed under age 7 modulated in 81% vs 25% if diagnosed after age 7
- Three or more penciled ribs (or three or more dystrophic features) predicts near-certain progression (≈85-87%)