Collagen Defect and Fragile Bones
- Type I: Mildest. Normal stature. Blue sclerae.
- Type II: Lethal. Perinatal death.
- Type III: Severe deforming. Progressive.
- Type IV: Moderate. Variable sclerae.
- Bisphosphonates: Increase bone density, reduce fractures.
- Rodding: Bailey-Dubow or Fassier-Duval telescoping rods.
- “Sillence classification
- “Collagen I defect
- “Bisphosphonates reduce fractures
- “Telescoping rods for deformity
Osteogenesis Imperfecta vs Non-Accidental Injury (NAI)
- Multiple fractures in OI can mimic NAI.
- Look for: Blue sclerae, wormian bones, family history, dentinogenesis imperfecta.
- Metaphyseal corner fractures are NOT typical of OI (they are specific for NAI).
- OI does NOT exclude the possibility of concurrent abuse.
Overview/Epidemiology
Osteogenesis Imperfecta (OI) is a genetic bone fragility disorder.
- Genetics: Most are autosomal dominant. COL1A1 or COL1A2 mutations (Type I collagen).
- Incidence: 1 in 10,000-20,000.
- Pathophysiology: Defective Type I collagen leads to weak bone matrix.
Pathophysiology, Anatomy and Pathomechanics
Collagen Abnormalities
- Type I collagen is the main organic component of bone.
- Defective collagen leads to poor bone quality despite normal mineral.
Why Fractures Occur
- Bones are structurally weak.
- Minimal trauma causes fractures.
- Bones may bow and deform due to repeated microfractures.
The Molecular Basis: Quantitative vs Qualitative Defects
The topic states the defect is in COL1A1/COL1A2 and that "defective collagen leads to poor bone quality" without explaining the genotype-phenotype link that examiners probe - why a Type I patient is mild and a Type II/III patient is devastated.
Normal type I collagen is a triple helix of two pro-alpha-1 (COL1A1) and one pro-alpha-2 (COL1A2) chains, with a glycine at every third residue (Gly-X-Y) that lets the helix pack tightly.
- Quantitative defect (→ mild, Type I). A null/loss-of-function COL1A1 allele produces about half the normal amount of structurally NORMAL collagen (haploinsufficiency). Less-but-normal collagen gives the mildest phenotype - the classic Type I.
- Qualitative / structural defect (→ severe, Types II-IV). A glycine substitution (or other structural mutation) produces an abnormal chain that is still incorporated into the triple helix, where it disrupts folding of the whole molecule - a dominant-negative ("protein suicide") effect. Abnormal collagen is worse than too little collagen, which is why structural mutations cause the lethal (II) and severely deforming (III) forms. Substitutions nearer the carboxy-terminus tend to be more severe.
- Recessive OI. A minority are autosomal recessive, caused by defects in genes handling collagen post-translational modification and folding - CRTAP, P3H1 (LEPRE1) and PPIB (the prolyl-3- hydroxylation complex) and chaperones - producing severe phenotypes without a primary collagen-gene mutation; these are over-represented in consanguineous populations.
This is why the field is moving from the purely clinical Sillence types toward a gene-based classification. (The biochemistry of collagen synthesis itself is developed in our Proteoglycans & Collagen topic.)
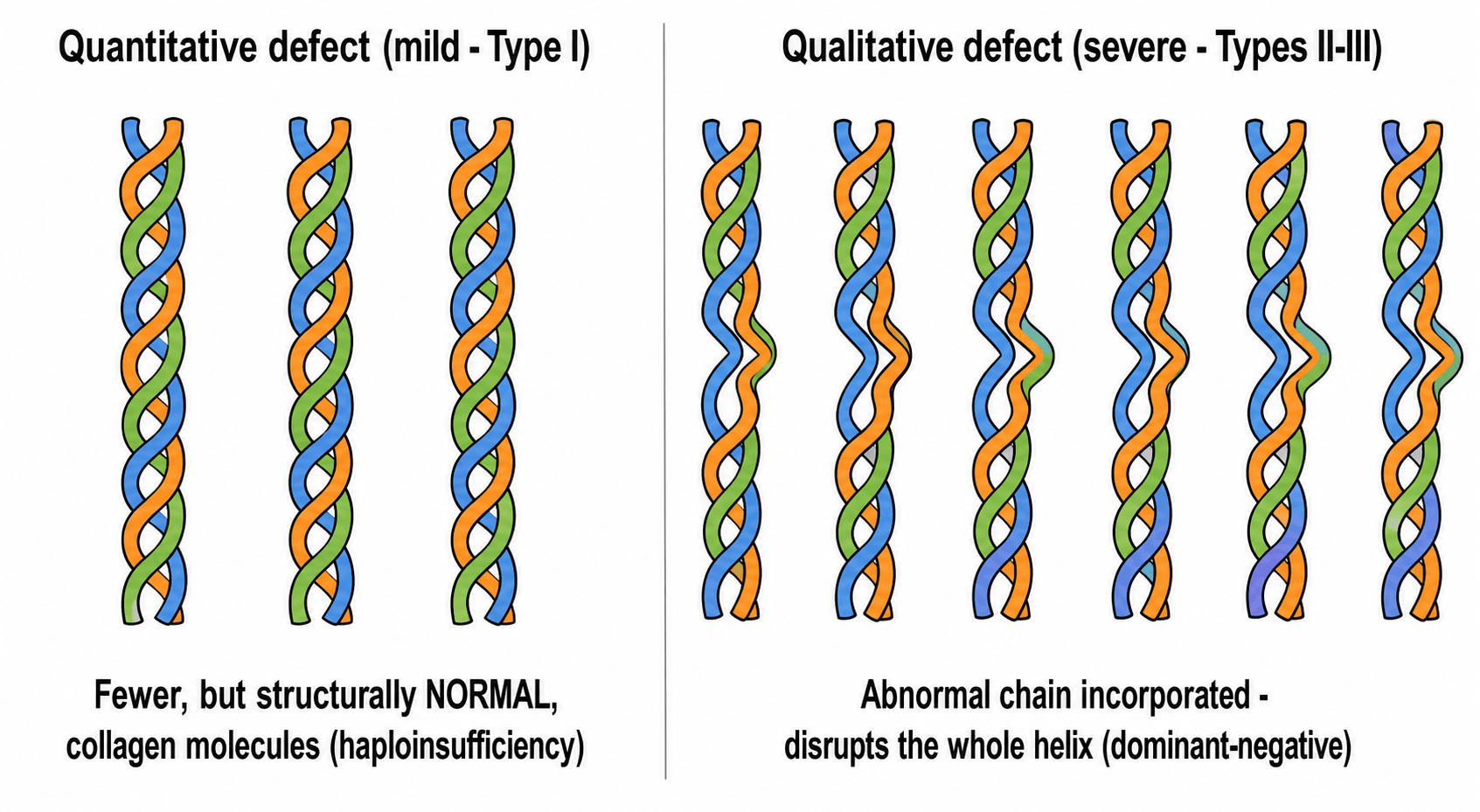
Less normal collagen = mild; abnormal collagen = severe. A COL1A1 null allele (haploinsufficiency, quantitative) gives the mild Type I; a glycine-substitution structural mutation is incorporated and exerts a dominant-negative effect, giving the lethal/severe Types II-III. Recessive OI (CRTAP, P3H1/ LEPRE1, PPIB) disrupts collagen post-translational modification/folding without a collagen-gene mutation.
Classification Systems
Sillence Classification
- Type I: Mild. Blue sclerae. Normal stature. Fewer than 20 fractures typically. Near-normal life.
- Type II: Lethal. Perinatal death. Severe bone fragility. Multiple intrauterine fractures.
- Type III: Severe deforming. Progressive. Blue/gray sclerae. Short stature. Often wheelchair-bound.
- Type IV: Moderate. Normal or gray sclerae. Variable short stature.
Clinical Assessment
- Fracture history (number, age of first).
- Family history.
- Mobility and function.
- Sclerae: Blue (Types I, II, III) or normal/gray (Type IV).
- Teeth: Opalescent, weak (dentinogenesis imperfecta).
- Hearing: May be impaired.
- Stature: Normal (Type I) or short (Types III, IV).
- Limbs: Bowing, deformity.
- Skin: Thin, easy bruising.
Investigations
- COL1A1/COL1A2 mutations: Confirmatory.
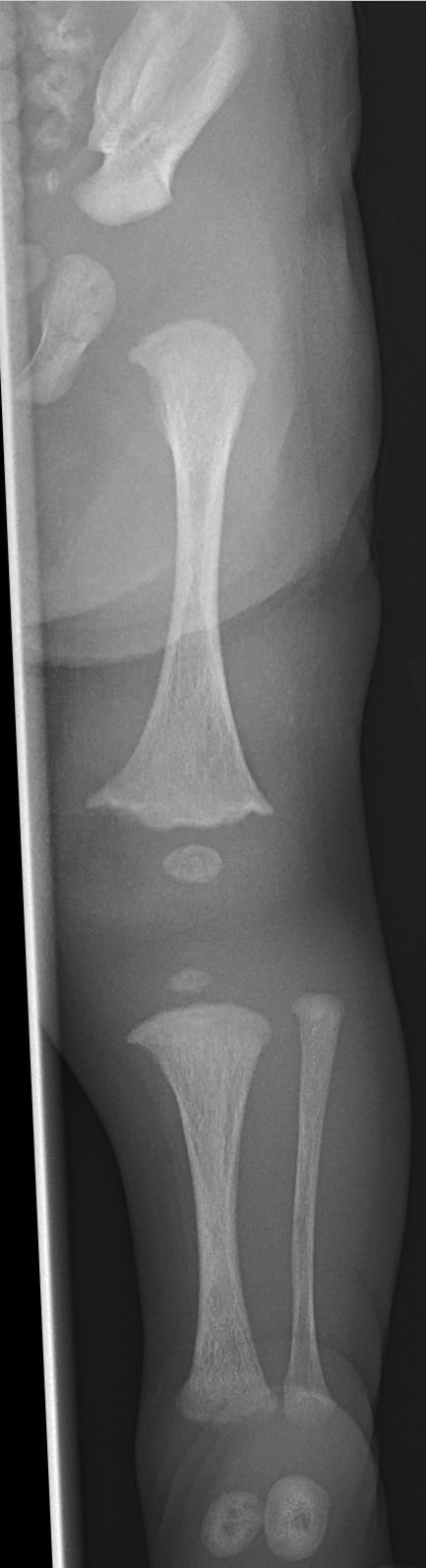
- X-rays: Osteopenia, wormian bones (skull), bowing, callus.
- DEXA: Low bone density.
- Audiometry: Hearing assessment.
- Dental: Dentinogenesis imperfecta.
Differential Diagnosis
- Distinguishing Features
- Metaphyseal corner fractures, posterior rib fractures, inconsistent history
- Distinguishing Features
- Widened physes, cupping, bowing - but normal bone quality
- Distinguishing Features
- Low alkaline phosphatase, premature tooth loss
- Distinguishing Features
- No blue sclerae, no dentinogenesis imperfecta
- Distinguishing Features
- Hypermobility predominant, not bone fragility
Management Algorithm
Bisphosphonates
- Pamidronate (IV) or Zoledronate: Most common in children.
- Mechanism: Inhibit osteoclast activity → increase bone density.
- Benefits: Reduce fracture rate, improve vertebral shape, reduce pain.
- Timing: Start early in moderate-severe OI.
Surgical Techniques
Fassier-Duval Rodding
Indications: Progressive bowing, recurrent fractures in femur or tibia.
Technique: Multiple osteotomies (sofield procedure) to correct bowing. Telescoping rod inserted (two components that slide apart as child grows).
Post-op: Protected weight bearing, then full.
Complications: Rod migration, failure to telescope, peri-implant fractures.
Perioperative & Anaesthetic Considerations
This topic describes rodding, osteotomies and scoliosis surgery without addressing the OI-specific perioperative and anaesthetic risks that make any operation hazardous - high-yield because these patients return to theatre repeatedly.
- Airway & cervical spine. Fragile, brittle teeth (dentinogenesis imperfecta) are easily damaged at laryngoscopy; a relatively large head and short neck, cervical-spine fragility and possible basilar invagination mean the neck must be handled gently (avoid forceful extension/manipulation) - anticipate a potentially difficult airway.
- Positioning is dangerous. An anaesthetised OI patient can fracture from handling alone - careful padding and gentle positioning, avoid a standard automated blood-pressure cuff (repeated inflation can fracture the humerus - use the lowest cuff/least frequent cycling or an arterial line), avoid forceful limb manipulation and tourniquets where possible, and consider that suxamethonium fasciculations may provoke fractures/hyperthermia.
- Intra-operative hyperthermia. OI carries a recognised tendency to intra-operative hyperthermia and a hypermetabolic response (a metabolic phenomenon distinct from classic malignant hyperthermia, though the two can be confused) - monitor temperature, avoid over-warming, and treat hyperthermia actively.
- Bleeding. A mild platelet dysfunction and capillary/vessel fragility give an increased bleeding tendency - anticipate blood loss in osteotomy/spinal surgery.
- Regional anaesthesia & continuing therapy. Spinal deformity, short stature and fragile bone make neuraxial/regional technique harder (not absolutely contraindicated); continue bisphosphonate therapy perioperatively (it need not be postponed around rodding - see the Azzam evidence), and plan within the multidisciplinary team. (General anaesthetic and regional technique are covered in our General Anaesthesia in Orthopaedics and Regional Anaesthesia topics; the craniocervical problem in our Basilar Invagination topic.)
Plan for a difficult airway (fragile teeth, short neck, cervical/basilar fragility - gentle neck handling), fracture-from-positioning (pad carefully, avoid the automated BP cuff, no forceful manipulation), a tendency to intra-operative hyperthermia (monitor temperature; distinct from malignant hyperthermia), and an increased bleeding tendency. Continue bisphosphonates perioperatively.
Complications
- Context
- Disease-related
- Management
- Bisphosphonates, rodding
- Context
- Telescoping rods
- Management
- Revision
- Context
- Weak bone
- Management
- Careful technique
- Context
- Severe OI
- Management
- Neurosurgical assessment
- Context
- Otosclerosis
- Management
- Audiology
Postoperative Care
- Protected Weight Bearing: Then progress.
- Physiotherapy: Maintain strength.
- Continue Bisphosphonates: Per protocol.
Outcomes/Prognosis
- Type I: Near-normal lifespan and function.
- Type II: Lethal.
- Type III: Wheelchair-dependent. Significant disability.
- Type IV: Variable. Many ambulatory.
- Bisphosphonates + Surgery: Improved outcomes in modern era.
Guidelines, Registries & Global Practice
Global epidemiology
- Birth prevalence approximately 1 in 15,000-20,000; Type I (mild) is the most common form worldwide.
- Autosomal dominant COL1A1/COL1A2 mutations account for the majority; recessive (e.g. CRTAP, P3H1/LEPRE1) and other rare forms are over-represented in consanguineous populations.
Side-by-side practice across major settings
- Consensus / Society Position
- Cyclic IV bisphosphonates (pamidronate or zoledronate) are standard for moderate-severe OI across North American, European and international metabolic bone units; oral agents used in milder disease
- Consensus / Society Position
- Telescopic intramedullary rodding (Fassier-Duval, Sheffield/Bailey-Dubow) with Sofield-type osteotomies is the global standard for deforming long-bone disease
- Consensus / Society Position
- International OI consensus and specialist centres advocate multidisciplinary clinics (orthopaedics, endocrinology/metabolic bone, genetics, rehab, dental, audiology)
- Consensus / Society Position
- Anti-sclerostin antibodies (e.g. setrusumab) and combination anabolic strategies are in later-phase trials, not yet routine
Registry & cohort evidence
- No dedicated implant registry equivalent to arthroplasty registries exists for OI; the evidence base is single-centre series (e.g. Shriners network) and natural-history cohorts.
- Key practical signal from cohorts: high lifetime revision burden for telescopic rods (around half of patients), driven mainly by growth.
High- vs limited-resource practice variation
- High-resource settings: early genetic confirmation, cyclic IV bisphosphonates from infancy, telescopic rodding, DXA surveillance, allied-health teams.
- Limited-resource settings: diagnosis is largely clinical/radiographic; bisphosphonate access and telescopic implants may be constrained, with greater reliance on bracing, non-telescopic rods (Rush rods/K-wires) and conservative fracture care.
Controversies & Areas of Uncertainty
- Do bisphosphonates actually reduce fractures? They reliably raise BMD, but the Cochrane review found fracture reduction is not conclusively proven and clinical-function benefits are inconsistent. BMD gain is a surrogate, not a guaranteed clinical endpoint.
- Optimal agent, dose and duration. Pamidronate vs zoledronate, IV vs oral, and how long to continue (risk of over-suppression, atypical fractures, delayed osteotomy healing) remain unresolved.
- Bisphosphonates and surgery. Whether to pause therapy around osteotomy/rodding is debated; some series (Azzam et al) continued therapy without postponement and reported acceptable union rates.
- Telescopic vs non-telescopic rods. Telescopic rods reduce re-operation for growth but carry their own failure modes (failure to telescope, migration); high overall revision rates persist regardless of implant.
- Emerging anabolics. Anti-sclerostin antibodies and other Wnt-pathway/anabolic agents show biochemical and BMD benefit in early trials, but fracture-reduction efficacy and paediatric safety are not yet established.
- OI and child protection. A genetic OI diagnosis does not exclude concurrent non-accidental injury; the threshold for safeguarding work-up remains a clinical judgement.
MCQ Practice Points
Q: Which OI type is lethal? A: Type II.
Q: What collagen type is affected in OI? A: Type I collagen (COL1A1/COL1A2).
Q: What is the mechanism of bisphosphonates? A: Inhibit osteoclasts → reduce bone resorption → increase bone density.
Q: What is the advantage of Fassier-Duval rods? A: Telescoping - they grow with the child.
Q: Which OI type has normal sclerae? A: Type IV - moderate severity with normal or gray sclerae.
Q: What fracture pattern is NOT typical of OI and suggests NAI? A: Metaphyseal corner fractures (bucket-handle) - these are specific for NAI.
Self-Assessment Quiz
At a Glance Table
- Details
- Genetic bone fragility disorder due to Type I collagen defect
- Details
- COL1A1/COL1A2 mutations, autosomal dominant (most)
- Details
- Sillence Types I-IV (expanded to VIII+)
- Details
- Fractures, blue sclerae, dentinogenesis imperfecta, hearing loss
- Details
- Bisphosphonates, telescoping rods, multidisciplinary care
- Details
- Type I near-normal, Type II lethal, Types III/IV variable
- Severity
- Mild
- Sclerae
- Blue
- Stature
- Normal
- Severity
- Lethal
- Sclerae
- Blue
- Stature
- N/A (perinatal death)
- Severity
- Severe
- Sclerae
- Blue/gray
- Stature
- Short
- Severity
- Moderate
- Sclerae
- Normal/gray
- Stature
- Short
OIOI Features
Hook:BBDH - Brittle Bones, Blue sclerae, Dentinogenesis, Hearing loss.
IIIIIIIVSillence Types
Hook:I-II-III-IV: Mild, Lethal, Severe, Moderate.
MFPIRTelescoping Rod Complications
Hook:MFPIR - Migration, Failure, Peri-implant, Infection, Revision.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“5-year-old with Type III OI. Fourth femur fracture in 2 years. Progressive bowing. On bisphosphonates.”
“Infant presents with multiple fractures. Parents claim OI. How do you differentiate from NAI?”
“How do bisphosphonates work in OI?”
GENETICS
- COL1A1/COL1A2
- Type I collagen
- Autosomal dominant
- Wormian bones
CLASSIFICATION
- I: Mild, blue sclerae
- II: Lethal
- III: Severe deforming
- IV: Moderate
FEATURES
- Fractures
- Blue sclerae
- Dentinogenesis
- Hearing loss
TREATMENT
- Bisphosphonates
- Telescoping rodding
- Protected mobilization
- Multidisciplinary
OI vs NAI
- Blue sclerae suggests OI
- Wormian bones suggests OI
- Metaphyseal corners = NAI
- OI does NOT exclude abuse
RODDING PEARLS
- Fassier-Duval = telescoping
- Sofield osteotomies correct bowing
- Complications: migration, failure
- Continue bisphosphonates post-op
Evidence Base
- Foundational genetic-clinical classification of OI into four types (I-IV)
- Distinguished phenotypes by severity, sclerae, inheritance and fracture pattern
- Established variable expressivity vs genetic heterogeneity framework
- Uncontrolled observational study, 30 children with severe OI on cyclic IV pamidronate
- Mean BMD rose 41.9% per year; z-score improved from -5.3 to -3.4
- Fracture incidence fell by 1.7 per year (p less than 0.001); healing and growth unaffected
- Authoritative seminar; expanded the four classical types to seven distinct phenotypes
- Most cases due to COL1A1/COL1A2 mutations; some have no detectable collagen mutation
- Bisphosphonates are an adjunct, not a cure; gene therapy remains preclinical
- Systematic review of 14 trials (819 participants), oral and IV bisphosphonates
- Consistently increase lumbar-spine BMD in children and adults
- Fracture reduction not conclusively proven; zoledronate vs pamidronate showed no clear superiority
- Single-surgeon series: 58 children, 179 lower-limb Fassier-Duval telescopic rods
- Revision required in 53% (mean 52 months), mostly growth-related; nonunion 14.5%
- Bisphosphonates continued perioperatively without postponement; mobility improved
- Randomised phase 2a trial, 14 adults with moderate OI, anti-sclerostin antibody (setrusumab/BPS804)
- Stimulated bone formation markers (P1NP +84%) and reduced resorption (CTX-1 -44%)
- Lumbar-spine aBMD increased 4% (p=0.038); generally well tolerated