More Than Just an Extra Toe
- Post-axial (Lateral) is common and often isolated.
- Pre-axial (Medial) is rare and associated with Hallux Varus recurrence.
- Central is rare and often syndromic.
- Syndromes: Ellis-van Creveld (Post-axial), Polydactyly-Syndactyly syndromes.
- Surgery: Ideally before walking age (9-12 months) for shoe fit.
- “Look for hands (often present in hands too)
- “Check for syndactyly (webbing)
- “Assess function (does the extra toe move?)
- “Palpate the metatarsal head (is it wide or duplicated?)
Don't treat Pre-axial Polydactyly lightly.
- Duplication of the Hallux (Pre-axial) is fraught with complications.
- The medial collateral ligament is often anomalous or absent.
- Ablating the medial duplicate without securing the ligament or correcting the alignment almost ALWAYS leads to Hallux Varus.
- The remaining toe drifts medially, making shoe wear impossible.
- Post-axial (Lateral)
- Common (80%)
- Pre-axial (Medial)
- Rare (15%)
- Post-axial (Lateral)
- Autosomal Dominant (African)
- Pre-axial (Medial)
- Sporadic / Syndromic
- Post-axial (Lateral)
- Simple (often skin tag)
- Pre-axial (Medial)
- Complex (Shared joints)
- Post-axial (Lateral)
- Residual bump
- Pre-axial (Medial)
- Hallux Varus
FASTSurgical Goals
Hook:Act FAST.
TEMPSyndromes to Consider
Hook:TEMP (Temperature check for syndromes).
Overview/Epidemiology
Polydactyly refers to the presence of supernumerary digits. It is the most common congenital foot deformity.

- Epidemiology: 1.7 per 1000 live births.
- Race: Significantly higher in African American populations (10-15x higher), where it is often purely Autosomal Dominant and Post-axial.
- Gender: Male predominance (Male greater than Female).
- Laterality: 50% bilateral.
- Association: While foot polydactyly can be isolated, hand polydactyly is more often syndromic. Always check the hands!
Pathophysiology and Mechanisms
- Skin Tag: Only soft tissue attachment (Type B post-axial).
- Partial: Duplication of phalanx only, sharing a metatarsal head.
- Complete: Complete duplication of the entire ray (phalanx + metatarsal). This essentially creates a "6th ray" and widens the foot significantly.
- Syndactyly: The extra digit is often webbed to the adjacent digit (Polysyndactyly).
- Bracket Epiphysis: Can be present in the duplicated parts, causing curvature.
- Tarsal Coalition: Rare but can occur in complex pre-axial cases.
Classification Systems
Anatomical Classification
Pre-axial: Medial side (Tibial). Involves the Hallux.
- Associated with tibial hemimelia, Carpenter syndrome.
- High risk of Hallux Varus outcome.
Central: 2nd, 3rd, or 4th rays.
- Rare. Usually syndactyly prevents separation.
- Often involves a "T-shaped" metatarsal.
Post-axial: Lateral side (Fibular). Involves the 5th toe.
- Type A: Well-formed digit. Articulates with metatarsal or phalanx.
- Type B: Rudimentary skin tag. Pedunculated.
PPCClassification (Temtamy and McKusick)
Hook:PPC hierarchy.
Clinical Assessment
- Family Hx: Anyone else in the family? (Suggests AD inheritance).
- Pregnancy: Any complications?
- Syndrome Review: Heart defects? Kidney issues? (Ellis-van Creveld, Patau).
- Count: Count the toes. Identifying which one is the "extra" one can be hard. Usually, the outer/marginal one is the extra one, but sometimes the inner one functions better.
- Function: Tickle the foot. Which toe flexes/extends better? Keep the functional one.
- Palpation: Feel the metatarsal head. Is it wide?
- Neurovascular: Ensure the digit to be kept has good perfusion.
Investigations
Plain Radiographs (AP and Oblique):
- Mandatory for surgical planning.
- Determine Level: Is the duplication at the PIP, MTP, or TMT joint?
- Determine Connection: Is it a bifid head? A bracket epiphysis? A completely separate ray?
- Ossification: Remember that in infants, much of the bone is cartilaginous and won't show. The X-ray underestimates the deformity.
Genetic Testing:
- Indicated if Central Polydactyly, Bilateral Pre-axial, or other dysmorphic features are present.
The Longitudinal Epiphyseal Bracket
The pathophysiology and imaging sections both flag a "bracket epiphysis", and the Belthur pre-axial series found one in 4 of 28 feet — but because it decides whether a reconstruction stays straight, it deserves to be understood in its own right.
A longitudinal epiphyseal bracket (LEB) is an abnormal C-shaped epiphysis that wraps around one side and tethers the whole length of a short tubular bone — most often the proximal phalanx of the hallux or a metatarsal. When it deforms a phalanx into a trapezoidal shape the result is the delta phalanx. Instead of growing only from the two ends, the bracketed bone grows along a longitudinally-oriented physis down one side, so it elongates asymmetrically and becomes progressively wedge-shaped, driving an angular deformity — classically the medial deviation that produces or worsens hallux varus in pre-axial duplication.
Why it matters in polydactyly:
- It is a frequent companion of pre-axial / great-toe duplication and a recognised cause of recurrent or residual angulation after an otherwise correct ablation.
- It is easy to miss because the infant bracket is largely cartilaginous and underestimated on plain films — the same caveat the imaging section gives for the deformity as a whole.
Management (according to PubMed, Belthur et al., in the Evidence Base): early detection and adequate excision of the longitudinal bracket affecting the phalanx or metatarsal reduces residual deformity and the need for revision surgery. The options are a central physiolysis / bracket resection — excising the abnormal longitudinal portion of the physis and interposing fat so it cannot re-tether, restoring more normal end-growth — and, for an established wedge, a corrective opening- or closing-wedge osteotomy of the bracketed bone, combined with the collateral-ligament and abductor-hallucis reconstruction the topic already describes.
Q: A toe drifts back into varus after a technically sound hallux-duplication ablation — what underlying bony anomaly should you suspect? A: A longitudinal epiphyseal bracket (delta phalanx) tethering the bone along a C-shaped physis and causing progressive wedging. Recognise it on imaging and address it (bracket resection/physiolysis or corrective osteotomy), because reconstructing the soft tissues alone will not hold against an unresected bracket.
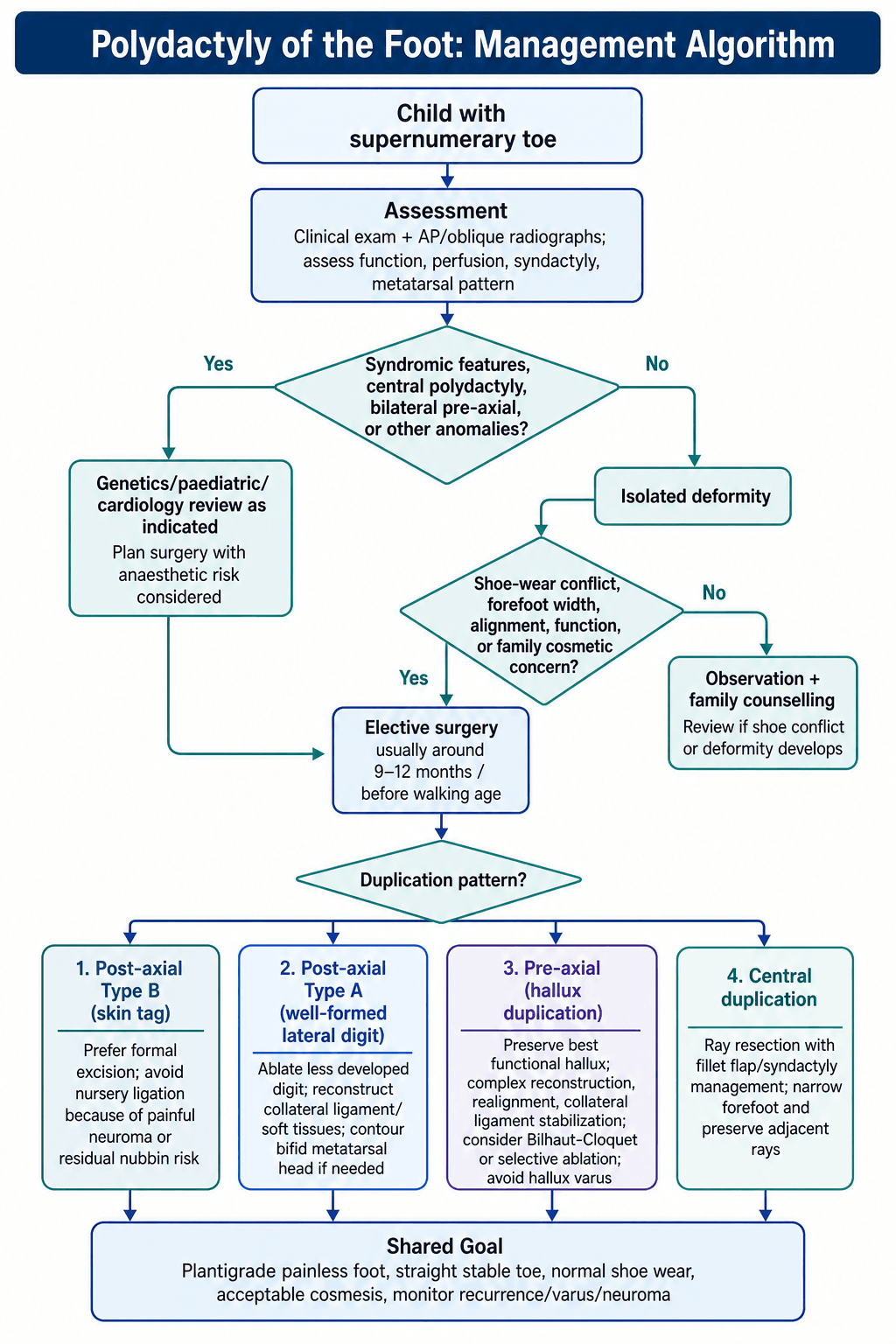
Management Algorithm
1. Observation / Suture Ligation
- Observation: Rarely indicated unless the extra digit is not causing shoe conflict (e.g., small central nubbin).
- Suture Ligation: Historically used for Type B Post-axial (skin tags) in the nursery.
- Current view: Discouraged. Can leave a painful neuroma or residual "nubbin" of cartilage. Surgical excision is cleaner.
Surgical Techniques
Post-Axial Ablation (Type A)
- Incision: Racket-shaped or elliptical incision around the base of the extra digit.
- Dissection: Trace the tendons. Often the abductor digiti minimi inserts on the extra toe. This must be transferred to the remaining 5th toe.
- Capsulotomy: Open the joint.
- Resection: Remove the extra phalanx. If the metatarsal head is bifid, shave down the prominent condyle (The "Block Test" - make sure it's not too wide for shoes).
- Reconstruction: Repair the Lateral Collateral Ligament using the periosteum sleeve from the amputated toe.
- Closure: Z-plasty if needed to prevent scar contracture.
This ensures a cosmetically acceptable narrowing of the foot.
Complications
- Rate
- Common
- Prevention/Management
- Angulation of remaining toe. Osteotomy correction.
- Rate
- High (Pre-axial)
- Prevention/Management
- Proper tendon transfer/capsule repair.
- Rate
- Common
- Prevention/Management
- Especially with Bilhaut-Cloquet procedure.
- Rate
- Common
- Prevention/Management
- Failure to narrow the metatarsal head.
- Rate
- Rare
- Prevention/Management
- Bury the nerve endings deep.
Postoperative Care
- Cast: Below-knee cast or soft bandage depending on stability. K-wires are protected for 4-6 weeks.
- Walking: If walking age, casts are essential to protect the reconstruction/wire.
- Shoe Wear: Resume normal shoes once swelling subsides (6-8 weeks).
- Follow-up: Essential to watch for growth deviation (physeal arrest/tether).
Outcomes/Prognosis
- Cosmesis: Generally excellent for post-axial ablation.
- Function: Normal gait is expected.
- Nail: Nail appearance is the most common complaint after Bilhaut-Cloquet.
- Retained Ray: Sometimes parents notice "the foot is still wide" if the metatarsal wasn't narrowed.
Guidelines, Registries & Global Practice
Global epidemiology
- Polydactyly is one of the most common congenital limb anomalies worldwide. Type B postaxial polydactyly is the single commonest form.
- Birth prevalence varies strikingly by ancestry. In US surveillance, postaxial polydactyly was roughly 26 times more frequent in infants of African ancestry than White infants (0.91 vs 0.035 per 100); Texas registry data show a prevalence ratio of about 4.4 for non-Hispanic Black versus non-Hispanic White births. Hand involvement is more common than foot involvement.
- Around 95 percent of postaxial type B cases are isolated and autosomal dominant; foot polydactyly is bilateral in about half of cases.
Guidance across societies (no formal single guideline exists) There is no dedicated international guideline for foot polydactyly; practice is governed by classification-led principles and society/textbook consensus rather than randomised evidence.
- Practical stance
- Individualise by classification; ablate the less functional/marginal ray; reconstruct collateral ligaments; operate near walking age
- Practical stance
- Discourage routine bedside ligation of type B digits in favour of formal excision; refer complex/pre-axial and syndromic cases
- Practical stance
- Surgeon-led individualised reconstruction; multidisciplinary input for syndromic disease
- Practical stance
- Watanabe / Venn-Watson / Blauth-Olason for pre-axial; Rotterdam foot classification for medial duplication; morphologic systems for central
Registry note: unlike arthroplasty, congenital toe deformities are not captured in implant registries (NJR/AJRR/AOANJRR). Population-level data come from birth-defect surveillance programmes (e.g. EUROCAT in Europe, US National Birth Defects Prevention Network, Texas Birth Defects Registry).
High- vs limited-resource practice variation
- Well-resourced settings: elective day-case surgery near walking age, formal excision over ligation, microsurgical/reconstructive options (on-top plasty, lengthening) for hypoplastic rays, and genetics input for syndromic disease.
- Limited-resource settings: later presentation is common; bedside suture ligation of type B digits in the newborn period persists for access/cost reasons despite the higher nubbin/neuroma rate; complex pre-axial and central reconstruction may be referred to tertiary centres.
Cultural sensitivity: in some communities an extra digit is regarded as auspicious; families may decline or delay surgery. Counsel on function, shoe-wear, and cosmesis without coercion.
Deep Dive: Surgical Pearls
1. The "Nubbin" Problem If you or a paediatrician ties off a Type B skin tag in the nursery, often a small "nubbin" of cartilage or nerve remains. This becomes painful in shoes later.
- Recommendation: Formal excision under local anaesthetic (if older) or GA (around 6-12 months) is superior. You can dissect out the nerve and ensure the bone is flush.
2. The Shared Epiphysis In Type A post-axial digits, the extra toe joint might share a common epiphysis with the normal toe.
- Risk: If you simply disarticulate, you leave an exposed, wide joint surface.
- Technique: You may need to perform an intra-articular osteotomy to narrow the metatarsal head, preserving the collateral ligament origin.
3. Pre-axial Hallux Varus The classic complication of removing the medial hallux.
- Cause: You have removed the medial buttress and the insertion of the Abductor Hallucis.
- Solution: You MUST reattach the Abductor Hallucis to the base of the remaining proximal phalanx. Often, a K-wire is needed to hold the toe in neutral / slight valgus for 4-6 weeks while this heals.
Controversies & Areas of Uncertainty
- Ligation vs formal excision for type B digits. The dominant evidence (Chopan systematic review: 23.5 vs 3 percent complications) favours excision, yet Ganju's patient-reported data suggest ligation is acceptable in selected cases with similar long-term pain — the trade-off is a higher rate of residual bumps and raised scars. There is no randomised trial.
- Optimal timing. "Before walking age (9-12 months)" is convention, not evidence-based dogma; some advocate early newborn excision of simple type B digits, others delay complex reconstructions until structures are larger. Anaesthetic safety, surgeon preference and complexity all weigh in.
- Which classification to use. Pre-axial duplication is variably described by Venn-Watson, Blauth-Olason and Watanabe; medial duplication now has the Rotterdam system. None is universal, and inter-observer reliability is only moderate, complicating cross-study comparison.
- Bilhaut-Cloquet's place. Effective for two equal hypoplastic digits but near-universally produces a nail ridge and stiffness; many surgeons now prefer ablation-plus-reconstruction or on-top plasty, reserving Bilhaut-Cloquet for narrow indications.
- Role of advanced imaging. Plain films underestimate the cartilaginous infant skeleton; the added value of routine ultrasound/MRI versus operative assessment is unsettled.
Deep Dive: The Genetics of Polydactyly
SHH Pathway The Sonic Hedgehog (SHH) gene is the master regulator of limb anterior-posterior patterning.
- Zone of Polarizing Activity (ZPA): Located on the posterior margin of the limb bud. It secretes SHH.
- Gradient: High concentrations of SHH on the posterior side specify "Little Finger/Toe". Low concentrations on the anterior side specify "Thumb/Hallux".
- Mutation: Ectopic anterior expression of SHH (often via ZRS regulatory mutations) causes Pre-axial Polydactyly and, in the extreme, mirror foot.
- GLI3: A key downstream effector, normally processed into a repressor anteriorly to oppose SHH. GLI3 haploinsufficiency causes both pre- and post-axial polydactyly and underlies Greig cephalopolysyndactyly and Pallister-Hall syndrome — i.e. GLI3 is not exclusively a "post-axial" gene.
According to PubMed, Quinn et al (Hum Mol Genet 2012) showed that loss of Zic3 rescues the polydactylous phenotype of Gli3-haploinsufficient mice by normalising the Gli3-repressor/activator ratio and abolishing ectopic anterior Shh — confirming GLI3 dosage as the pivotal regulator of digit number (DOI).
MCQ Practice Points
Q: Which population has the highest incidence of Polydactyly? A: African Ancestry (Post-axial, Autosomal Dominant).
Q: What is the most common complication of simple ablation of a medial (pre-axial) supernumerary digit? A: Hallux Varus (due to loss of medial stabilizers).
Q: Ellis-van Creveld syndrome is associated with which type of polydactyly? A: Post-axial (Lateral).
Q: In central polydactyly, what is the most appropriate surgical management? A: Ray Resection (Filleting) helps narrow the foot and remove the duplicated ray.
Q: What is the Bilhaut-Cloquet procedure? A: Sharing procedure combining halves of two hypoplastic digits to form one normal digit.
Self-Assessment Quiz
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“Neonate with Type B post-axial polydactyly (skin tag). Paediatrician asks if they can just tie it off with a suture.”
“1-year-old with duplicated Hallux. Medial toe is smaller. Lateral toe is normal. Plan?”
“Child with bilateral post-axial polydactyly, short stature, and a heart murmur. Diagnosis?”
CLASSIFICATION
- Pre-axial (Medial)
- Post-axial (Lateral - Common)
- Central (Rare)
- Type A / Type B
SYNDROMES
- Ellis-van Creveld
- Trisomy 13 (Patau)
- Carpenter Syndrome
- Greig Cephalopolysyndactyly
KEY RISKS
- Nubbin formation (Ligation)
- Hallux Varus (Pre-axial)
- Nail Dystrophy (Bilhaut-Cloquet)
- Dehiscence
MANAGEMENT
- Observation
- Suture Ligation (Avoid)
- Formal Ablation
- Ray Resection
Evidence Base
- 125 patients, 194 supernumerary toes; post-axial accounted for 79 percent
- Most common pattern: proximal phalangeal duplication on a block or wide metatarsal head
- At mean 15.1-year follow-up, 94 percent excellent or good results; poor results clustered around pre-axial duplications and persistent hallux varus
- 21 children (28 feet) over 30 years; all had associated anomalies of the affected foot
- Congenital hallux varus was the most common association (20 of 28 feet); a longitudinal epiphyseal bracket was present in 4 feet
- Watanabe classification judged more useful than Venn-Watson for surgical planning; good-or-better results in all feet at final follow-up
- PRISMA systematic review (1950–2017), 10 studies on type B postaxial digits
- In the largest cohort analysis, complication rate was 23.5 percent for suture ligation versus 3 percent for surgical excision
- Ligation complications were residual remnants ('nubbins') and neuromas
- 258 type B postaxial digits; raised/sensitive scar in 51.5 percent after ligation vs 35.4 percent after excision
- Odds of a residual bump or raised scar were significantly higher after ligation (p = 0.001)
- Long-term pain/sensitivity was similar between groups
- 73 feet classified by duplication type, syndactyly, hypoplastic ray, and hallux deviation
- A hypoplastic ray was present in 75 percent and complete metatarsal duplication in 29 percent
- Moderate-to-good intrarater and interrater reliability (kappa up to 0.79)
- 11 central duplications among 136 feet with polydactyly (central is rare)
- Stratified into type I (independent digits), II (equal-size duplicates), III (unequal duplicates)
- Tailored Bilhaut-Cloquet, bone-removing flap, or simple ablation by morphologic type for best cosmesis
- 545 affected infants in surveillance of 289,365 births
- Isolated in 95 percent; Black infants affected far more often than White (0.91 vs 0.035 per 100)
- Hand involvement much more common than foot; autosomal dominant with variable expressivity postulated