Fixed Pronation Deformity | Congenital vs Post-Traumatic | Cleary and Omer Classification
- Congenital failure of segmentation (longitudinal)
- Fixed pronation deformity is classic presentation
- Functional deficit determines treatment (eating, hygiene)
- Derotation osteotomy is treatment of choice
- Mobilization (excision) has high recurrence rate and is contraindicated in congenital
- “Bilateral in 60% of cases
- “Associated with Apert, Carpenter, Klinefelter syndromes
- “Shoulder abduction compensates for pronation loss
- “Look for posterior radial head dislocation (Type III)
Patients compensate for fixed pronation with shoulder abduction and wrist hypermobility. Assess function (hand-to-mouth, keyboard use) rather than just angles.
Excision of synostosis in congenital cases has excessively high recurrence rates and poor outcomes. Do NOT offer this in the viva.
Derotation osteotomy carries risk of compartment syndrome and neurovascular compromise if correction is extreme (over 80°). Prophylactic fasciotomy may be indicated.
In bilateral cases, fix dominant arm in less pronation (10-20°) for writing/eating, and non-dominant in neutral/slight supination for hygiene.
- Key Feature
- Functional adaptation
- Management
- Observation
- Key Feature
- Difficulty eating/typing
- Management
- Derotation Osteotomy
- Key Feature
- Acquired stiffness
- Management
- Excision (once 'cold')
- Key Feature
- Posterior head dislocation
- Management
- Osteotomy (Avoid head reduction)
HEAD P-ACleary and Omer Classification
Hook:Think of the Radial Head Position: Reduced to Reduced to Posterior to Anterior
NO CUTContraindications to Excision
Hook:NO CUT - Do not excise congenital synostosis!
BADIndications for Surgery
Hook:Surgery is BAD - Bilateral, Angle, Deficit!
Overview and Epidemiology
Pathophysiology
- Failure of Segmentation: Radius and ulna share a continued cartilaginous anlage (perichondrium).
- Longitudinal Separation: Normally occurs from distal to proximal during weeks 5-8 of gestation.
- Arrest: Failure of proximal separation results in synostosis.
- Genetic: Associated with FGFR2 mutations (Apert), HOXD13 (Polysyndactyly).
Anatomy
Anatomical Defects
- Radius: Often larger, bowed, and longer than normal.
- Radial Head: May be absent, hypoplastic, or dislocated (posterior more often than anterior).
- Muscles: Supinators may be absent or fibrotic. Pronator teres often shortened/fibrotic.
- Neurovascular: PIN position may be aberrant.
Pathophysiology
Embryological Development
Radioulnar synostosis occurs due to failure of longitudinal segmentation of the cartilaginous anlage:
- Week 5-7 gestation: Common cartilaginous mass differentiates into radius and ulna
- Segmentation begins proximally and proceeds distally
- Interzone apoptosis separates the two bones
- Complete separation by week 8
- Congenital: Failure of interzone formation → bones remain fused
- Post-traumatic: Bone bridging across the interosseous space after fracture healing
Molecular Mechanisms
Risk Factors for Post-Traumatic Synostosis
- Monteggia fractures - Highest risk
- Both-bone forearm fractures - Especially same-level fractures
- High-energy trauma - Extensive soft tissue injury
- Delayed surgery - More periosteal reaction
- Open approach to both bones through same incision
- Bone grafting - Graft material in interosseous space
- Head injury patients - Increased heterotopic ossification risk
Classification
Cleary & Omer Classification
Based on radiographic appearance and radial head position.
- Description
- Fibrous synostosis (no bone bridge)
- Head Position
- Reduced
- Description
- Bony synostosis
- Head Position
- Reduced
- Description
- Bony synostosis
- Head Position
- Posterior Dislocation
- Description
- Bony synostosis
- Head Position
- Anterior Dislocation
Type III is the most common pattern.
Clinical Presentation
History
- Age: Usually noted at 2-5 years when complex hand tasks accumulate.
- Complaint: "Difficulty holding soup bowl" (supination deficit) or "awkward running style".
- Pain: Unusual. Pain suggests radial head instability or post-traumatic etiology.
- Function: Difficulty typing, using cutlery, hygiene (wiping requires supination).
Examination
Physical Exam
- Forearm Position: Usually fixed in 15-60° of pronation.
- ROM: Block to rotation. Assess elbow flexion/extension (often normal).
- Compensatory Motion: Assess shoulder ROM. High demand on shoulder rotation.
- Radial Head: Palpate for dislocation (posterior prominence).
- Neurology: Rule out associated neurological conditions.
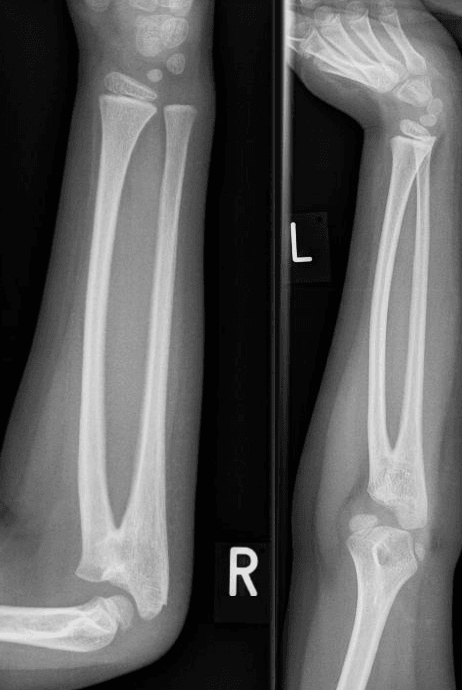
Investigations
-
X-ray: PA and Lateral extended forearm.
- Proximal radius/ulna fusion.
- Radial head position (Types III/IV).
- Radial bowing.
-
CT: Rarely needed for diagnosis but useful for surgical planning (osteotomy site).
-
MRI: Identifying fibrous band in Type I (rarely indicated).
Differential Diagnosis
The hallmark of synostosis is a fixed block to forearm rotation with preserved elbow flexion/extension. Distinguish it from other causes of limited supination/pronation:
- Distinguishing Feature
- Painless, fixed pronation, often bilateral
- Key Discriminator
- Bony/fibrous bridge proximally on radiograph
- Distinguishing Feature
- Limited rotation but NO synostosis bridge
- Key Discriminator
- Convex, dome-shaped radial head; no fusion
- Distinguishing Feature
- Acquired stiffness after Monteggia/both-bone fracture
- Key Discriminator
- History of trauma; discrete bridge across interosseous space
- Distinguishing Feature
- Distal radius growth arrest, wrist deformity
- Key Discriminator
- Volar-ulnar distal radial tilt; rotation often preserved
- Distinguishing Feature
- Dynamic pronation, partly correctable under anaesthesia
- Key Discriminator
- Increased tone; rotation passively improves when relaxed
- Distinguishing Feature
- Multiple rigid joint contractures
- Key Discriminator
- Generalised joint involvement, absent skin creases
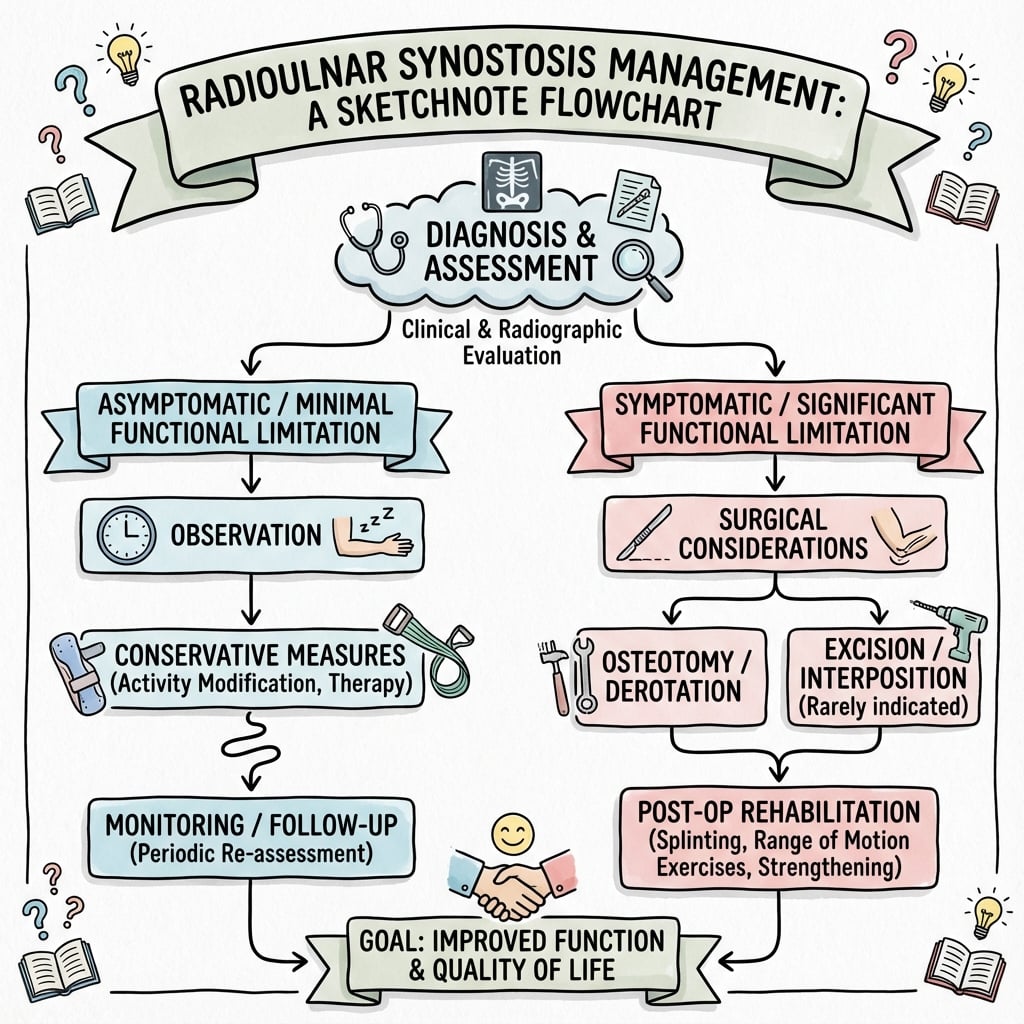
Management
Treatment Approach
- Mild (under 30-60° pronation): Observation. OT for adaptive strategies.
- Severe (over 60° pronation): Surgical correction.
- Functional deficit: Indication for surgery regardless of angle.
Surgical Technique
Derotation Osteotomy
The Gold Standard for congenital synostosis.
Surgical Steps
Distal or mid-shaft approach. Proximal approach (at synostosis) is dangerous due to neurovascular structures. Osteotomy is performed distal to the synostosis.
Transverse or Z-osteotomy through radius and ulna (if fused distally) or just radius/ulna individually if synostosis is proximal. Subperiosteal dissection is critical to protect soft tissues.
Rotate forearm to desired position (e.g., 10° supination). Watch pulse/perfusion. The soft tissues (IM membrane) will be tight. Ensure no tension on the skin closure.
Types:
- K-wires: Percutaneous, easier removal. Crossed K-wires are standard.
- Plate/Screw: More stable, requires removal in kids. 2.7mm or 3.5mm LC-DCP.
- Cast: Long arm cast required. Meticulous molding is essential to hold rotation.
Check compartment pressure. If tight, consider leaving deep fascia open or performing fasciotomy. Skin should be closed without tension.
Correction of severe deformity (over 80°) tightens the interosseous membrane and vessels. High risk of compartment syndrome/Volkmann's ischemia. Consider staged correction or prophylactic fasciotomy for severe angles.
Gradual Derotation with an External Fixator
The safety alerts, the controversies and the quiz all recommend "staged/gradual correction with an external fixator" for severe deformity, but the technique is never described - even though it is the principal way to correct a large deformity safely.
The problem it solves. The interosseous membrane, vessels and nerves are chronically shortened in a forearm fixed in hyperpronation. Twisting that forearm acutely through a large arc (the topic's quoted danger zone of roughly 60-80 degrees and beyond) wrings out the vessels and raises compartment pressure - the mechanism of the compartment syndrome / Volkmann's ischaemia warned about throughout.
How gradual correction works.
- A single-bone osteotomy (usually the ulna) is made distal to the synostosis and an external fixator (monolateral or a ring/circular frame) is applied across it.
- After a short latency period, the forearm is derotated a few degrees per day (typically over one to three weeks) until the target position is reached, then held in the frame until union.
- The slow rotation lets the shortened soft tissues, nerves and vessels accommodate gradually, so perfusion is maintained and a larger total correction can be achieved than would be safe acutely.
Trade-offs. It avoids acute neurovascular catastrophe and the need for a prophylactic fasciotomy, but at the cost of a frame on a child's arm for weeks, pin-site infection, a longer treatment course and family burden. It is therefore reserved for the severe/high-risk corrections; moderate deformities are still corrected acutely with internal fixation under vigilant compartment monitoring.
For a severe fixed pronation (beyond the ~60-80 degree acute-safe limit), correct gradually with an external fixator across a single-bone osteotomy, derotating a few degrees per day. Slow correction lets the chronically shortened interosseous membrane and vessels accommodate, preventing the acute "wringing-out" that causes compartment syndrome - the alternative to acute correction plus prophylactic fasciotomy.
Complications
-
Recurrence (Loss of Correction):
- Excision: Recurrence rates are greater than 90% and osteotomy is preferred.
- Derotation Osteotomy: Re-ankylosis in the new position is the goal, but loss of rotational correction can occur if fixation is inadequate or removed early.
- Non-union: Rare at osteotomy site due to robust periosteum in children.
-
Compartment Syndrome (Volkmann's Ischemia):
- Mechanism: Severe derotation (over 60-80°) wrings out the interosseous membrane and vessels.
- Prevention: Prophylactic fasciotomy or staged correction.
- Monitoring: Vigilant post-operative checks. Low threshold for splitting casts.
-
Neurovascular Injury:
- Posterior Interosseous Nerve (PIN): Anatomy is distorted. The nerve may run adjacent to or through the synostosis mass. Distal osteotomy avoids this zone.
- Radial Artery: Kinking can occur. Radial pulse must be documented pre- and post-correction.
- Median Nerve: Can be compressed under the pronator teres during pronation-to-supination correction.
-
Cosmetic:
- "Back of Hand": Fixed pronation leads to unsightly eating mechanics.
- Scars: Forearm scars can hypertrophy.
Postoperative Care
- Immobilization: Long arm cast for 6-8 weeks until bony union.
- Monitoring: Overnight admission for compartment checks mandatory.
- Follow-up: Check union. Hardware removal often required.
Outcomes
- Functional: Excellent improvement in ADLs (eating, hygiene). Most parents report high satisfaction with the functional gains.
- Cosmetic: Improved. The "awkward" arm position while running or at rest is resolved.
- ROM: Rotation is NOT restored (it is a fusion in a better position). Patients adapt well using shoulder motion.
- Satisfaction: Generally high if target angles are met. Bilateral severe cases derive the most benefit.
- Long-term: No long-term data suggests increased risk of elbow or wrist arthritis, as the articular surfaces are generally spared (unless Type IV/anterior dislocation).
Post-Traumatic Synostosis: Prevention and Resection
The topic lists the risk factors for post-traumatic synostosis, carries the Jupiter resection card, and notes resection "once cold" - but the prevention and the timing/technique of resection are never pulled together. This matters because, unlike the congenital form, post-traumatic synostosis is largely preventable and genuinely resectable.
Prevention is the first principle. Most post-traumatic radioulnar synostosis is iatrogenic or technique-related and avoidable:
- Rationale
- A single approach to both bones risks bridging the interosseous space - especially with same-level fractures
- Rationale
- Periosteal reaction and haematoma in the interosseous space are the substrate for the bone bridge
- Rationale
- Graft material can seed an interosseous bridge
- Rationale
- Restores the interosseous gap and limits stiffness/heterotopic bone
- Rationale
- Indomethacin/NSAID or single-dose radiation are options - the pharmacology and evidence are developed in
heterotopic-ossification; note Jupiter's series achieved good results WITHOUT prophylaxis
The highest-risk settings - Monteggia injuries, same-level both-bone fractures, high-energy trauma and the head-injured patient - warrant the most meticulous technique.
Resection - and when. A discrete, mature post-traumatic bridge can be excised to restore rotation (the opposite of the rule in congenital disease):
- Wait for maturity before resecting - a well-defined cortical margin on CT and a metabolically quiescent ("cold") bone scan with a plateaued/normalising alkaline phosphatase, classically around 6-12 months. (Jupiter & Ring resected at a mean of 19 months; in their series, resecting before versus after 12 months did not significantly change the rotation regained.)
- Excise the bridge and restore the interosseous space; free-fat interposition did not significantly change outcome in the Jupiter series.
- Outcome: non-recurring limbs regained an average of 139 degrees of rotation; the single recurrence was the only patient with a closed head injury - the key recurrence risk factor.
Post-traumatic synostosis is the exception to the "never excise" rule. Prevent it (separate incisions, gentle technique, no graft in the interosseous space); if it forms, wait until it is mature/'cold' (well-corticated on CT, normalised ALP, ~6-12 months) then resect to restore rotation. Jupiter & Ring regained ~139 degrees, with the only recurrence in a closed-head-injury patient - the dominant recurrence risk.
Guidelines, Registries & Global Practice
Global Epidemiology
- Proximal radioulnar synostosis is the most common congenital anomaly of the proximal forearm, but is rare overall (a few hundred cases reported worldwide).
- Bilateral in roughly 60% of cases; both sexes affected, with most non-syndromic isolated cases linked to SMAD6/NOG variants or sex-chromosome aneuploidy.
- Largest contemporary series (97 patients, 122 forearms; European multicentre) confirms Type III as the most frequent radiographic pattern.
Side-by-Side Guidance
There is no dedicated society guideline for this rare condition; evidence is case-series level. Principles converge across bodies:
- Position
- Avoid resection in congenital disease; derotational osteotomy for functional deficit; non-operative for mild
- Position
- Function (not angle alone) drives surgery; position dominant limb in slight pronation, non-dominant near neutral
- Position
- Centralised paediatric hand units; OT-led adaptation first; operate for fixed hyperpronation impairing ADLs
- Position
- Excision of mature, discrete post-traumatic synostosis once 'cold'; prophylaxis (NSAID/radiation) debated
Registries
- No arthroplasty/implant registry captures this condition. Outcome data derive from single-centre and pooled case series (e.g. the 2022 meta-analysis of 383 forearms and the 2025 European multicentre cohort).
High- vs Limited-Resource Practice
- Well-resourced settings: early occupational therapy, genetic testing (SMAD6/NOG, karyotype for Klinefelter), CT planning, and plate-fixed proximal osteotomy with overnight compartment monitoring.
- Limited-resource settings: diagnosis often delayed until school age; plain radiographs suffice; single-bone derotation held with K-wires and a long-arm cast is a pragmatic, low-cost alternative to plating. Genetic services may be unavailable, so clinical syndrome screening (whole-patient examination) is essential.
Controversies & Areas of Uncertainty
Osteotomy through the synostosis allows single-cut correction but concentrates the neurovascular/compartment risk; a distal (single-bone) osteotomy is safer but technically may under-correct. No high-level evidence settles this.
The safe single-stage limit is debated (often quoted as 60-85°). Some advocate gradual correction with an external fixator for severe deformity; others perform prophylactic fasciotomy and correct acutely. No randomised data exist.
Function, not a fixed angle, drives intervention. The largest cohort found no significant difference in patient-reported outcome between operated severe cases and non-operated mild cases, so unilateral, well-compensated children are often best observed.
Resection (mobilisation) of a congenital bridge has near-universal recurrence and is contraindicated; it remains valid only for discrete post-traumatic synostosis. Interposition material has not been shown to change outcome even there.
MCQ Practice Points
Q: What are the most common syndromic associations with radioulnar synostosis?
A: Apert Syndrome (Acrocephalosyndactyly) and Klinefelter Syndrome (XXY). Also Carpenter, Fetal Alcohol, and Arthrogryposis. However, most cases are isolated with no syndromic features.
Q: In bilateral radioulnar synostosis, what is the ideal position for the dominant arm?
A: 10-20° pronation for the dominant arm (facilitates writing and eating). The non-dominant arm should be fixed in neutral to slight supination for perineal hygiene.
Q: Why is excision contraindicated in congenital radioulnar synostosis?
A: Recurrence rate approaches 100% even with interposition materials. Soft tissues are foreshortened, muscles absent/fibrotic, and active rotation cannot be restored. Derotation osteotomy is the only option.
Q: At what gestational stage does radioulnar synostosis occur?
A: Weeks 5-8 when longitudinal segmentation of the forearm anlage occurs. Segmentation proceeds distal to proximal, so failure at the proximal end causes proximal radioulnar synostosis.
Q: A child undergoes 80° derotation osteotomy and develops increasing pain with passive finger stretch. What is the diagnosis?
A: Compartment syndrome. Acute correction over 60-80° tightens the interosseous membrane and vessels. Prophylactic fasciotomy is recommended for large corrections.
Additional Quiz Questions
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 4-year-old presents with bilateral fixed pronation of 90 degrees. Parents are concerned about his eating.”
“Why do you not simply excise the bridge to restore motion?”
“What are the risks of performing a one-stage correction of 90 degrees?”
Key Classification (Cleary Omer)
- Type I: Fibrous
- Type II: Bony
- Type III: Posterior Head
- Type IV: Anterior Head
Treatment Angles
- Unilateral: 10-20 Sup
- Bi-Dom: 10-20 Pro
- Bi-NonDom: Neutral
- Max correction: 60-80 degrees
Buzzwords
- Failure of Segmentation
- Fixed Pronation
- Shoulder Abduction Compensation
- Compartment Syndrome
Evidence
Cleary and Omer: Natural History and Classification (Landmark)
- Natural-history study of 23 non-operated patients with 36 congenital proximal radioulnar synostoses; forearms fixed at a mean of 30 degrees pronation.
- Described four radiographic patterns based on the osseous synostosis and radial head position - the descriptive classification still used today.
- Forearm position was NOT related to subjective limitation, employment, or objective (Jebsen) hand-function testing; most patients had few or no functional limitations.
- Concluded that operative treatment is RARELY indicated and that objective function, not the fixed angle alone, should drive assessment.
Bilateral Synostosis: Position of Fixation
- 33 patients (17 bilateral) treated with derotational osteotomy.
- 82% good or excellent results; 8 complications, 4 neurovascular.
- Best end position: 10-15° pronation in the dominant limb, neutral in the other.