Myelomeningocele and Orthopaedic Care
- Neurological Level: Determines ambulatory potential.
- Hip Dysplasia: Common but treatment controversial.
- Clubfoot: Often rigid, surgical.
- Scoliosis: Congenital and neuromuscular types.
- Fractures: Insensate limbs prone to pathological fractures.
- “Level determines function
- “Hip surgery controversial
- “Clubfoot needs surgery
- “Insensate = fracture risk
Patients with Spina Bifida have INSENSATE lower limbs below the lesion level.
- Pathological fractures occur with minimal trauma.
- Pressure sores are common - careful orthotic fitting essential.
- Post-operative cast care must be meticulous.
- Teach patients/families to check skin daily.
Overview/Epidemiology
Spina Bifida is a neural tube defect where the spinal column fails to close during the first 28 days of embryonic development.
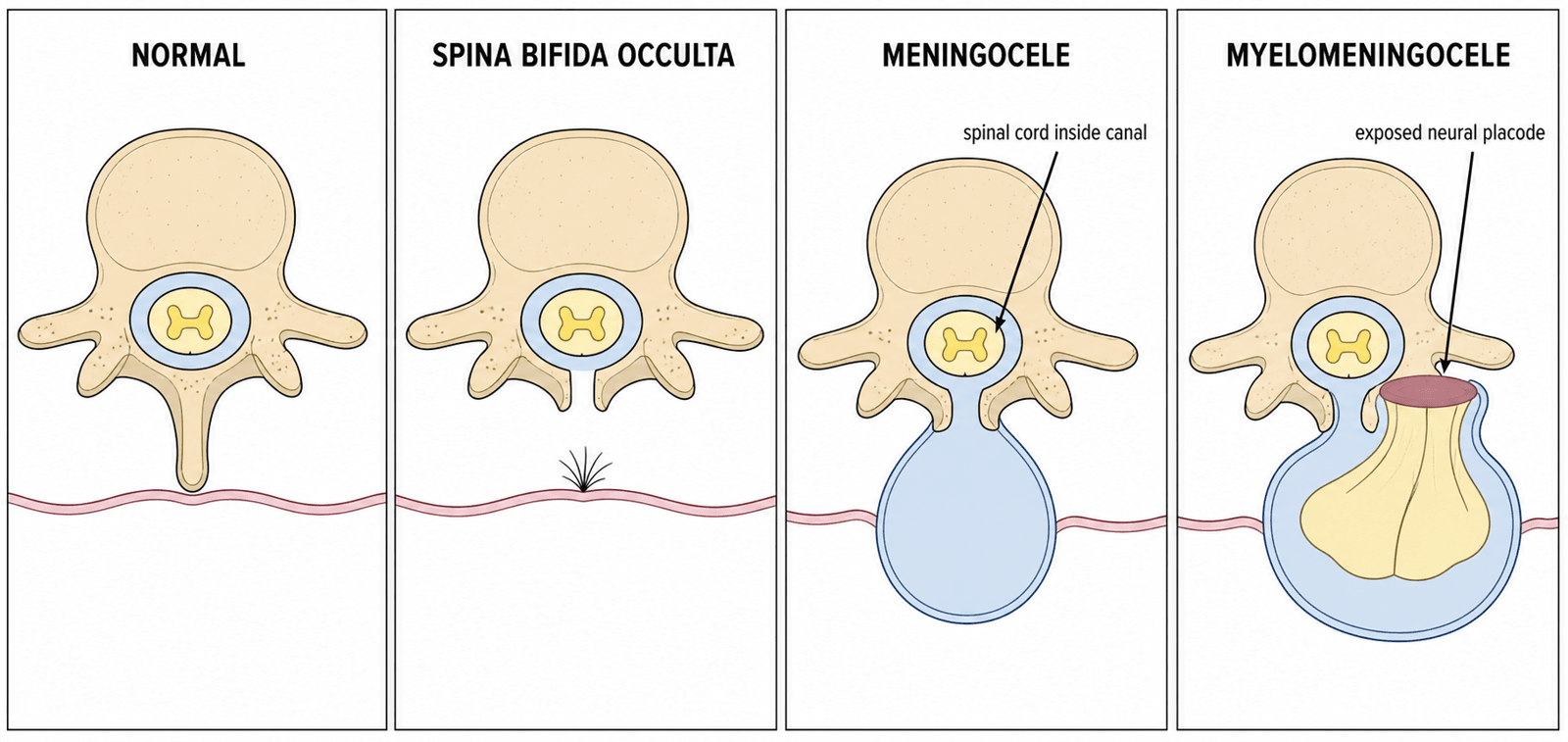
Types of Spina Bifida
-
Myelomeningocele (95% of cases):
- Most severe open form - exposed neural placode
- Spinal cord and meninges herniate through defect
- Associated with significant neurological deficit
- Requires immediate surgical closure after birth
- Nearly always associated with Chiari II malformation
-
Meningocele (4%):
- Meninges herniate through defect, spinal cord intact
- Usually better neurological function
- May present as lumbosacral mass at birth
- Surgical closure required
-
Spina Bifida Occulta (1%):
- Minor posterior arch defect without herniation
- Often asymptomatic, incidental finding
- Skin markers: Hair tuft, dimple, lipoma, hemangioma
- May be associated with tethered cord
Epidemiology
- Incidence: 0.5-1 per 1000 live births in folate-fortified populations; 2-4 per 1000 historically
- Geographic variation: Highest in Celtic/British Isles and parts of China and Latin America; lowest where flour is mandatorily fortified
- Sex ratio: Slight female predominance
- Risk factors: Maternal folate deficiency, anticonvulsants (valproate, carbamazepine), maternal diabetes, obesity, hyperthermia, prior affected pregnancy, MTHFR polymorphisms
Prevention - Folic Acid
- Periconceptional supplementation: 400-800 mcg folic acid daily for all women planning pregnancy, starting at least 1 month pre-conception through the first trimester
- High-risk women: 5 mg daily (previous NTD pregnancy, antiepileptic drugs, diabetes, obesity)
- Mandatory flour fortification: Adopted in the USA (1998), Canada, Australia/New Zealand (2009), and over 80 countries; not yet mandatory across most of Europe
- Evidence: The MRC Vitamin Study RCT showed a 72% reduction in NTD recurrence with periconceptional folic acid; fortification programs reduce population NTD prevalence by roughly 30-50%
Associated Conditions
- Chiari II Malformation: Nearly 100% with myelomeningocele
- Hydrocephalus: 80-90% require VP shunt
- Tethered Cord: May develop progressively
- Syringomyelia: Common finding on MRI
- Neurogenic Bladder: Universal below lesion level
- Neurogenic Bowel: Requires bowel management program
- Cognitive Impairment: Variable, often preserved intelligence
Pathophysiology, Anatomy & Pathomechanics
Neurological Level and Motor Function
- The level of the lesion determines muscle function below
- Motor function is predictable based on spinal level
- Sensation is typically absent below the lesion
- The motor level often differs from the sensory level
- Key Muscle
- Iliopsoas
- Function
- Hip flexion
- Clinical Test
- Observe hip flexor power
- Key Muscle
- Iliopsoas, Adductors
- Function
- Hip flexion/adduction
- Clinical Test
- Hip adduction against resistance
- Key Muscle
- Quadriceps
- Function
- Knee extension
- Clinical Test
- Knee extension against gravity
- Key Muscle
- Tibialis Anterior
- Function
- Ankle dorsiflexion
- Clinical Test
- Walk on heels
- Key Muscle
- EHL, Peroneals
- Function
- Great toe extension, eversion
- Clinical Test
- Great toe dorsiflexion
- Key Muscle
- Gastrocnemius
- Function
- Ankle plantarflexion
- Clinical Test
- Single leg heel raise
- Key Muscle
- Bladder/Bowel
- Function
- Continence
- Clinical Test
- Urodynamics
Pathogenesis of Orthopaedic Deformities
Muscle Imbalance Principle
- Active muscles without functioning antagonists cause progressive deformity
- Example: Active hip flexors (L1-L2) without extensors (L5-S1) = hip flexion contracture
- Example: Active quadriceps (L3) without hamstrings = knee hyperextension
Specific Deformity Patterns by Level
-
Thoracic Level:
- No lower limb motor function
- Paralytic hip dislocation (both hips)
- Spinal deformity common (100% have scoliosis)
- Severe kyphosis may interfere with sitting
-
High Lumbar (L1-L2):
- Hip flexors active, extensors absent → flexion contracture
- Hip adductors active without abductors → adduction contracture
- Progressive hip subluxation/dislocation (muscle imbalance)
- Knee flexion contractures common
-
Mid Lumbar (L3-L4):
- Quadriceps active → community ambulators
- Hip instability less severe
- Knee extension possible but may have hyperextension
- Foot deformities common (clubfoot, calcaneus)
-
Low Lumbar (L5-S1):
- Near-normal motor function
- Mild foot deformities (pes cavus, clawing)
- Good ambulatory potential
- Less severe spinal issues
Why Orthopaedic Issues Are Universal
- Muscle Imbalance: Drives most deformities
- Lack of Sensation:
- No protective sensation → unrecognized trauma
- Pressure sores under braces and casts
- Pathological fractures present with swelling (no pain)
- Gravity and Positioning:
- Unopposed forces create contractures
- Hip flexion contracture from prolonged sitting
- Osteoporosis:
- Insensate, non-weight-bearing limbs become osteoporotic
- High fracture risk with minimal trauma
Classification Systems
Classification by Neurological Level
- Thoracic: No lower limb motor function. Wheelchair-bound.
- High Lumbar (L1-L2): Hip flexion only. Standing frames.
- Mid Lumbar (L3-L4): Quadriceps active. Community ambulation with AFOs.
- Low Lumbar (L5): Ankle dorsiflexion. Good ambulators.
- Sacral: Ankle plantar flexion. Near-normal walking.
Clinical Assessment
History
Essential Information
- Neurological level: Documented motor and sensory level
- Ambulatory status: Current and best function achieved
- Bladder/bowel function: Clean intermittent catheterization, bowel program
- Prior surgeries: Closure, shunt, orthopaedic procedures
- Shunt status: Type, last revision, symptoms of malfunction
Red Flags to Identify
- Shunt malfunction symptoms: Headache, vomiting, irritability, decreased consciousness
- Tethered cord symptoms: Deteriorating gait, new weakness, increasing scoliosis, change in bladder function
- Skin breakdown: Location, duration, prior wounds
- Recent fractures: Often missed due to lack of pain
Physical Examination
Neurological Assessment
- Motor level: Test each myotome systematically
- Sensory level: Light touch and pinprick
- Reflexes: May be variable depending on level
- Document baseline for comparison
Spine Examination
- Scoliosis assessment: Adam's forward bend test, trunk shift
- Kyphosis: Lumbar kyphosis common, rigid vs flexible
- Skin over spine: Scars, sinus tracts
- Sitting balance: Essential for wheelchair users
Hip Examination
- Range of motion: Document flexion contracture (Thomas test)
- Hip stability: Barlow/Ortolani in infants, assess with motion
- Gait: If ambulatory, observe pattern
- Sitting posture: Pelvic obliquity from hip problems
Knee Examination
- Flexion contractures: Common, limit ability to use orthoses
- Hyperextension: May occur with quadriceps function
- Extension lag: Quadriceps strength assessment
Foot Examination
- Deformity type: Clubfoot, vertical talus, calcaneus, cavus
- Rigidity: Assess correctability
- Skin: Pressure points, calluses, ulcers
- Braceable: Can foot fit in AFO without pressure issues?
Skin Examination
- Critical assessment - insensate skin very vulnerable
- Under braces and orthoses
- Bony prominences
- Prior wound sites
- Signs of infection
Ambulatory Classification
- Motor Function
- None below
- Ambulatory Potential
- Wheelchair only
- Orthotic Needs
- Standing frame (therapeutic)
- Motor Function
- Hip flexors
- Ambulatory Potential
- Standing frames
- Orthotic Needs
- HKAFO, wheelchair primary
- Motor Function
- Quadriceps
- Ambulatory Potential
- Community ambulation
- Orthotic Needs
- KAFO or AFO
- Motor Function
- Ankle dorsiflexion
- Ambulatory Potential
- Community, minimal aids
- Orthotic Needs
- AFO, often supramalleolar
- Motor Function
- Plantarflexion
- Ambulatory Potential
- Near-normal
- Orthotic Needs
- Shoe inserts only
Investigations
- Spine X-ray: Scoliosis, kyphosis, vertebral anomalies.
- Hip X-ray: DDH, subluxation.
- Foot X-ray: Clubfoot, talus position.
- MRI Spine: Tethered cord (before scoliosis surgery).
- EMG: If level unclear.
- Urodynamics: Bladder function.
Differential Diagnosis
The differential is for the flaccid lower-limb paralysis, foot deformities and neurogenic bladder seen in a child, plus the imaging differential of a lumbosacral mass or midline skin lesion.
- Distinguishing Features
- Open defect, neural placode exposed, Chiari II, hydrocephalus
- Key Discriminator
- Visible open lesion at birth, flaccid paralysis below level
- Distinguishing Features
- Skin-covered; cutaneous markers (lipoma, hair tuft, dimple, sinus)
- Key Discriminator
- Progressive (not static) deficit; MRI shows low conus
- Distinguishing Features
- Absent sacral segments, popliteal webbing, maternal diabetes
- Key Discriminator
- Lateral radiograph shows absent sacrum/lumbar vertebrae
- Distinguishing Features
- Multiple rigid joint contractures, normal sensation, intact bladder
- Key Discriminator
- Sensation PRESERVED; symmetric rigid contractures
- Distinguishing Features
- Symmetric flaccid weakness, fasciculations, normal sensation/sphincters
- Key Discriminator
- Genetic (SMN1); sensation and continence preserved
- Distinguishing Features
- Acquired progressive deficit, back pain, level on MRI
- Key Discriminator
- History of trauma or enhancing lesion on MRI
The cardinal feature separating spina bifida (and other dysraphisms) from arthrogryposis and SMA is absent sensation below the level. Insensate skin drives the pressure-sore and pathological-fracture risk that dominates orthopaedic care.
Management Algorithm
Hip Management
- High Lumbar (L1-L2): Treatment controversial. Many do not operate.
- Mid-Low Lumbar: May benefit from reduction if ambulatory potential.
- Surgical Options: Open reduction, femoral/pelvic osteotomy.
- Salvage: McHale (proximal femoral resection-interposition).
Surgical Techniques
Scoliosis Surgery in Spina Bifida
Indications
- Progressive curve greater than 40-50 degrees
- Declining sitting balance affecting function
- Trunk imbalance causing pain or skin breakdown
- Pulmonary compromise (rare)
Pre-operative Planning
- MRI Spine: Exclude tethered cord - if present, release first
- Neurosurgery consultation: Shunt assessment
- Latex-free OR: Pre-order all equipment
- Blood typing: High blood loss procedure
- Nutritional optimization: Many are malnourished
Surgical Technique
- Posterior spinal fusion: Standard approach
- Fusion levels: T2 to pelvis for wheelchair users
- Pelvic fixation: Iliac screws or Galveston technique
- Avoid short fusions: High failure rate
- Bone graft: Consider allograft supplementation
Key Considerations
- Latex allergy: Universal precautions
- Poor bone quality: Larger, longer screws needed
- Skin closure: May be difficult over kyphosis
- Shunt: Position carefully, avoid kinking
- Post-op: Custom seating may be needed
Salvage of the Painful Dislocated Hip — The McHale Procedure
The management and surgical sections name the McHale procedure (proximal femoral resection-interposition) as the salvage option for the dislocated hip but never describe it. This matters because in spina bifida the goal of hip surgery is rarely a "stable, reduced" joint — it is comfort, sitting and hygiene in a limb where reduction does not improve walking.
When salvage (not reconstruction) is the aim
- The problem hip in an older, non-ambulatory patient is typically chronically dislocated, stiff and painful, sometimes with a windswept pelvis, pelvic obliquity, perineal-care difficulty or skin breakdown over the prominent femoral head.
- Reconstruction (open reduction, femoral and pelvic osteotomy) is inappropriate for the stiff, degenerate, insensitive-yet-painful hip; a resection/salvage procedure is chosen instead.
What the McHale procedure is
- Described by McHale and colleagues, it combines resection of the femoral head and neck with a proximal (subtrochanteric) valgus osteotomy of the femur.
- The valgus osteotomy angles the remaining proximal femur away from the acetabulum and ischium, so the femoral shaft points laterally. This resists the proximal migration and painful bony impingement that limit a simple Girdlestone-type head-and-neck excision (Castle resection) done alone.
- Soft tissue is interposed over the cut bone ends to cushion the construct — hence the "resection-interposition" descriptor.
Goals and caveats
- Goals: pain relief, improved hip range for comfortable sitting and perineal/hygiene access, and easier positioning — not restoration of a weight-bearing, ambulatory hip.
- Recognised problems: heterotopic ossification, proximal migration with recurrent impingement, and persistent or recurrent pain; postoperative traction/positioning and, in some hands, short-term immobilisation are used to limit migration — always weighed against the pressure-sore and osteoporosis risks of immobilising an insensate limb.
For the stiff, chronically dislocated, painful neuromuscular hip, do not attempt reconstruction — salvage. The McHale procedure (femoral head-and-neck resection plus a proximal valgus osteotomy) redirects the femur away from the pelvis to limit the proximal migration and impingement that plague plain excision. The aim is comfortable sitting and hygiene, not walking.
Complications
Complications of Spina Bifida - Orthopaedic Focus
- Incidence
- Very common
- Presentation
- Skin breakdown over bony prominence
- Management
- Prevention, wound care, plastic surgery
- Incidence
- 20-30%
- Presentation
- Swelling, warmth (mimics infection)
- Management
- Gentle splinting, avoid immobilization
- Incidence
- 30-70%
- Presentation
- Anaphylaxis, urticaria
- Management
- Latex-free OR environment
- Incidence
- Progressive
- Presentation
- New weakness, scoliosis progression
- Management
- MRI, neurosurgical release
- Incidence
- Variable
- Presentation
- Headache, vomiting, altered consciousness
- Management
- Urgent neurosurgery
Pressure Sores - Critical Issue
High-Risk Areas
- Under braces and orthoses
- Ischial tuberosities (wheelchair users)
- Sacrum and coccyx
- Heels and malleoli
- Over prominent hardware
Prevention Strategies
- Regular skin checks (daily for at-risk areas)
- Properly fitted orthoses - check at every visit
- Pressure-relieving cushions for wheelchairs
- Weight shifts and position changes
- Patient/family education
Management When Present
- Remove all pressure from area
- Wound care (may need plastic surgery)
- Underlying osteomyelitis may require debridement
- Can take months to heal
Pathological Fractures
- Mechanism: insensate, osteoporotic bone (femur/tibia) fractures with minimal or unrecognised trauma
- Presentation: swelling and warmth without pain; mimics infection (may have low-grade fever from fracture haematoma)
- Management: gentle splinting only; avoid prolonged immobilization which worsens osteoporosis and causes pressure sores; healing occurs but may be slow
Perioperative Complications
Latex Allergy
- Present in 30-70% of spina bifida patients
- Due to repeated procedures and latex exposure
- Mandatory latex-free OR for all procedures
- Pre-operative antihistamines in known cases
Shunt Considerations
- Inform neurosurgery of planned surgery
- Position to avoid pressure on shunt
- Monitor for signs of malfunction post-op
- May need shunt adjustment for positioning
Wound Healing
- Poor skin quality common
- Increased infection risk
- Consider plastic surgery involvement for complex closures
- Extended antibiotics often required
Latex Allergy in Spina Bifida — Why and What To Do
The topic repeatedly flags latex allergy (present in roughly 30-70% of spina bifida patients) as a mandatory perioperative consideration, but the reason it clusters in this population — and the concrete protocol — deserve development.
Mechanism and why spina bifida is high-risk
- Latex allergy is a Type I, IgE-mediated immediate hypersensitivity to soluble proteins in natural rubber latex (from Hevea brasiliensis), not to the finished rubber itself.
- Spina bifida patients are sensitised by early, repeated and mucosal/parenteral exposure: multiple operations from birth (closure, shunt, orthopaedic), and lifelong clean intermittent catheterisation with latex catheters. Cumulative number of operations is the strongest risk factor; myelomeningocele (versus lower dysraphism) and atopy add further risk.
- Sensitisation can be silent — a positive specific-IgE without prior clinical reaction still mandates avoidance, because the first clinical event may be intra-operative anaphylaxis.
Latex-fruit syndrome (cross-reactivity)
- Latex proteins (notably hevein/prohevein and class-I chitinases) cross-react with plant foods. Ask specifically about reactions to banana, avocado, kiwi and chestnut (the classic quartet), and also passionfruit, fig and papaya.
- A history of oral itch/swelling with these foods is a clinical clue to occult latex sensitisation.
Perioperative protocol
- Primary prevention is the highest-yield step: raising every child with spina bifida in a latex-free environment from birth measurably lowers sensitisation rates, so avoidance is not only a theatre issue.
- For any procedure: designate a latex-free (latex-safe) theatre — synthetic (nitrile/neoprene) gloves, latex-free catheters, tourniquets, drains, syringe plungers, medication vial bungs and anaesthetic circuit; schedule the patient first on the list to minimise airborne latex particulate from prior cases.
- Treat unexplained intra-operative cardiovascular collapse, bronchospasm or urticaria — often appearing minutes after induction/skin or mucosal contact — as latex anaphylaxis until proven otherwise; management is standard anaphylaxis care (remove the trigger, adrenaline, fluids, airway support).
- Routine antihistamine/steroid "premedication" does not reliably prevent latex anaphylaxis and does not replace strict avoidance.
Spina bifida is the archetypal cause of clinically significant natural-rubber-latex allergy because of cumulative early surgical and catheter exposure. Screen for latex-fruit cross-reactivity (banana, avocado, kiwi, chestnut), and the answer to "how do you prevent it?" is a latex-free environment from birth plus a latex-safe, first-on-the-list theatre — not premedication.
Postoperative Care
Immediate Postoperative Period
Skin Monitoring
- Critical in first 48-72 hours
- Cast windows for skin inspection
- Bivalved casts when possible
- Daily skin checks by nursing staff
- Teach family to inspect on discharge
Positioning
- Avoid pressure on shunt
- Pressure-relieving mattress
- Regular turning (every 2 hours minimum)
- Heel protection mandatory
Pain Management
- May have diminished pain perception
- But still need adequate analgesia - central processing intact
- Watch for signs of discomfort (irritability, vital signs)
- Regional blocks can be effective
Cast Care in Spina Bifida
- Insensate limbs cannot report problems - window/bivalved cast, well-padded over bony prominences, not too tight, parents check edges daily
- Keep duration short (skin tolerance), transition to a carefully moulded orthosis when safe
Rehabilitation
Goals by Level
- Thoracic: Maximize upper body strength, wheelchair skills
- L1-L2: Standing program if appropriate, transfers
- L3-L4: Gait training with appropriate orthoses
- L5-Sacral: Optimize gait efficiency, minimize energy expenditure
Orthotic Management
- Fitted by experienced orthotist
- Check fit at every clinic visit
- Anticipate growth - regular adjustments
- Replace when worn or outgrown
Outcomes/Prognosis
Ambulatory Outcomes by Level
- Community Ambulation Rate
- 0%
- Long-term Mobility
- Wheelchair-dependent
- Community Ambulation Rate
- 0-10%
- Long-term Mobility
- Standing frames, wheelchair primary
- Community Ambulation Rate
- 50-80%
- Long-term Mobility
- Community ambulation common
- Community Ambulation Rate
- 80-100%
- Long-term Mobility
- Near-normal ambulation
Factors Affecting Outcome
Positive Prognostic Factors
- Lower neurological level (L4-Sacral)
- Preserved cognition
- Strong family support
- Access to multidisciplinary care
- Early intervention for deformities
Negative Prognostic Factors
- Higher lesion level
- Significant cognitive impairment
- Multiple shunt revisions
- Severe scoliosis
- Recurrent pressure sores
Life Expectancy
- Significantly improved with modern care
- Most patients with myelomeningocele reach adulthood
- Main causes of death: Shunt-related, renal failure, respiratory
- Quality of life can be excellent with appropriate support
Transition to Adult Care
- Plan transition from age 14-16 years
- Identify adult orthopaedic surgeon experienced with spina bifida
- Ongoing surveillance for:
- Skin breakdown
- Progressive deformity
- New weakness (tethered cord)
- Spina Bifida Foundation support services
Guidelines, Registries & Global Practice
Global Epidemiology
- Prevalence: 0.5-1 per 1000 live births in folate-fortified countries; 2-4 per 1000 historically and in unfortified regions
- Highest rates: British Isles/Celtic populations, northern China, parts of Latin America
- Lowest rates: USA, Canada, Australia/New Zealand and other countries with mandatory flour fortification
- Mandatory fortification (now in over 80 countries) reduces population NTD prevalence by roughly 30-50%
Folic Acid Guidelines - Side by Side
- Recommendation
- 400 mcg/day periconceptionally; advocates mandatory staple-food fortification
- Recommendation
- 400 mcg/day for all; 5 mg/day if previous NTD, diabetes, BMI of 30 or more, or on antiepileptics
- Recommendation
- 400-800 mcg/day for all women capable of pregnancy (Grade A); mandatory grain fortification since 1998
- Recommendation
- 400-500 mcg/day; 5 mg/day high-risk; mandatory bread-making flour fortification since 2009
Orthopaedic & Surgical Practice Consensus
- AAOS / POSNA & EPOS (European Paediatric Orthopaedic Society): deformity management individualised to functional level; preserve a plantigrade, braceable foot; avoid routine hip reduction in high-level lesions
- AO/Scoliosis Research Society: pre-operative spinal MRI to exclude symptomatic tethered cord; long posterior fusion to the pelvis for neuromuscular curves affecting sitting balance
- Fetal therapy consensus (post-MOMS): in-utero repair offered in selected centres meeting MOMS eligibility criteria, balanced against preterm birth and uterine risk
Registries & Surveillance
- EUROCAT (European congenital anomaly surveillance) and the ICBDSR track NTD prevalence and the impact of fortification policy internationally
- National Spina Bifida Patient Registry (USA) captures longitudinal multidisciplinary outcomes
- No dedicated implant registry exists for spina bifida; arthroplasty/instrumentation outcomes are drawn from neuromuscular subgroups within general registries
High- vs Limited-Resource Practice Variation
- High-resource: multidisciplinary clinics (paediatric orthopaedics, neurosurgery, urology, rehabilitation, orthotics), urodynamics-guided bladder care, fetal surgery programmes, custom orthoses and seating
- Limited-resource: late presentation of unrepaired/neglected defects, higher infection and pressure-sore burden, reliance on serial casting and simpler bracing; fortification programmes are the highest-yield public-health intervention
Controversies & Areas of Uncertainty
- Current Position
- Strong evidence (Wright; Clin Orthop Relat Res 2011) that reduction does not improve walking. Reserve surgery for symptomatic unilateral dislocation causing pelvic obliquity/skin breakdown. Avoid in painless bilateral dislocation.
- Current Position
- The MOMS RCT showed in-utero repair halves shunt rates and improves motor/ambulation outcomes, but at the cost of preterm birth and uterine dehiscence. Not all fetuses are candidates; counselling must balance maternal risk.
- Current Position
- Initial correction rates approach those of idiopathic clubfoot, but recurrence is far higher (~68% vs ~26%). Casting is now first-line, reserving extensive release/talectomy for refractory feet.
- Current Position
- Curve correction is achievable but functional/seating benefit is uncertain and complication rates (infection, non-union, wound breakdown) exceed 50% in several series. Decision is individualised around sitting balance and skin.
- Current Position
- Radiological tethering is near-universal; release is indicated only for symptomatic progression (new weakness, scoliosis progression, pain, urological change), not for imaging findings alone.
- Current Position
- 400-800 mcg prevents most NTDs; mandatory fortification debated in Europe over theoretical masking of B12 deficiency and cancer concerns, though large analyses have not confirmed harm.
MCQ Practice Points
Q: A patient with L3 spina bifida has which muscle function? A: Quadriceps (knee extension). Can be a community ambulator.
Q: Does hip reduction improve walking in spina bifida? A: Controversial - traditional view is no improvement.
Q: What is the goal of foot surgery in spina bifida? A: Plantigrade foot that can be braced.
Q: What allergy is common in spina bifida? A: Latex allergy.
Q: What must be excluded before scoliosis surgery in spina bifida? A: Tethered cord - requires pre-operative MRI and neurosurgical release if present.
Q: How does a pathological fracture present in spina bifida? A: Swelling and warmth without pain - mimics infection but occurs due to insensate osteoporotic bone.
Self-Assessment Quiz
At a Glance
- Details
- Neural tube defect with failure of caudal neural tube closure (~day 28)
- Details
- 0.5-1 per 1000 live births in fortified populations; 2-4 per 1000 historically
- Details
- Periconceptional folic acid (400-800 mcg/day; 5 mg if high-risk)
- Details
- Neurological level determines ambulatory potential
- Details
- Diagnosed prenatally or at birth
- Details
- Universal - hip, spinal deformity, feet, fractures
- Key Muscle
- None below
- Ambulatory Potential
- Wheelchair
- Key Muscle
- Hip flexors
- Ambulatory Potential
- Standing frames only
- Key Muscle
- Quadriceps
- Ambulatory Potential
- Community with AFOs
- Key Muscle
- Ankle dorsiflexion/plantar flex
- Ambulatory Potential
- Community, minimal aids
L1L2L3L4L5S1Neurological Level and Function
Hook:L1-2-3-4-5, S1 = Hip Flex/Add, Knee Ext, Ankle Dorsi/Evert, Plantar Flex.
HSFKOrthopaedic Issues
Hook:HSFK - Hips, Spine, Feet, Knees.
RCFHip Treatment Controversy
Hook:RCF - Reduction controversial, consider function.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“5-year-old with L3 level spina bifida. Ambulant with AFOs. Presents with bilateral hip subluxation.”
“Same child also has rigid bilateral clubfoot. How would you manage?”
“10-year-old with thoracic level spina bifida. Wheelchair-bound. Thoracolumbar scoliosis 60 degrees with pelvic obliquity.”
“8-year-old with L2 level spina bifida presents with swelling and warmth of the left thigh. No history of trauma. Parents worried about infection.”
LEVELS
- L1-L2: Hip flexors
- L3-L4: Quads (ambulator)
- L5: Ankle dorsiflexion
- Thoracic: Wheelchair
ORTHOPAEDIC
- Hips: Controversial
- Spine: Scoliosis/Kyphosis
- Feet: Clubfoot
- Fractures: Insensate
SURGERY ISSUES
- Latex allergy
- Tethered cord
- Pressure sores
- Shunt malfunction
GOALS
- Maximize function
- Plantigrade feet
- Sitting balance
- Prevent sores
Evidence Base
- RCT of prenatal vs postnatal MMC repair, stopped early for efficacy (183 patients)
- Shunt placement by 12 months: 40% prenatal vs 82% postnatal (RR 0.48)
- Improved motor function and ambulation at 30 months; reduced hindbrain herniation
- Increased preterm delivery and uterine dehiscence
- Full 183-patient cohort, 30-month outcomes
- Independent ambulation 44.8% prenatal vs 23.9% postnatal (p=0.004)
- Functional level at least 2 better than anatomic level in 26.4% vs 11.4%
- Lesion at L3 or below and in-utero leg movement predicted independent walking