Progressive Motor Neuron Disease
- SMN1 Gene: Survival motor neuron gene mutation.
- Four Types: Based on age of onset and motor milestones.
- Scoliosis: Universal in Type I/II, common in Type III.
- New Therapies: Gene therapy and antisense oligonucleotides.
- Respiratory Care: Primary cause of mortality.
- “Know the SMA types and motor milestones
- “Scoliosis is nearly universal
- “Gene therapy has changed prognosis
- “Respiratory failure is the main cause of death
New disease-modifying therapies have dramatically changed the prognosis for SMA.
- Nusinersen (Spinraza): Antisense oligonucleotide. Intrathecal. Increases SMN2 expression.
- Onasemnogene (Zolgensma): Gene therapy. Single IV dose. Replaces SMN1.
- Early treatment (before symptom onset) leads to best outcomes.
- Orthopaedic manifestations may still occur but are less severe with early treatment.
- Onset
- Less than 6 months
- Motor Milestones
- Never sits
- Prognosis
- Death by 2 years without treatment
- Onset
- 6-18 months
- Motor Milestones
- Sits, never walks
- Prognosis
- Survives to adulthood with support
- Onset
- Greater than 18 months
- Motor Milestones
- Walks (may lose ability)
- Prognosis
- Normal or near-normal lifespan
- Onset
- Adult onset
- Motor Milestones
- Walks
- Prognosis
- Mild, slowly progressive
SMASMA Types
Hook:I-II-III-IV: Infant, Intermediate, Late, Adult.
SHCOrthopaedic Issues
Hook:SHC - Scoliosis, Hips, Contractures.
Overview/Epidemiology
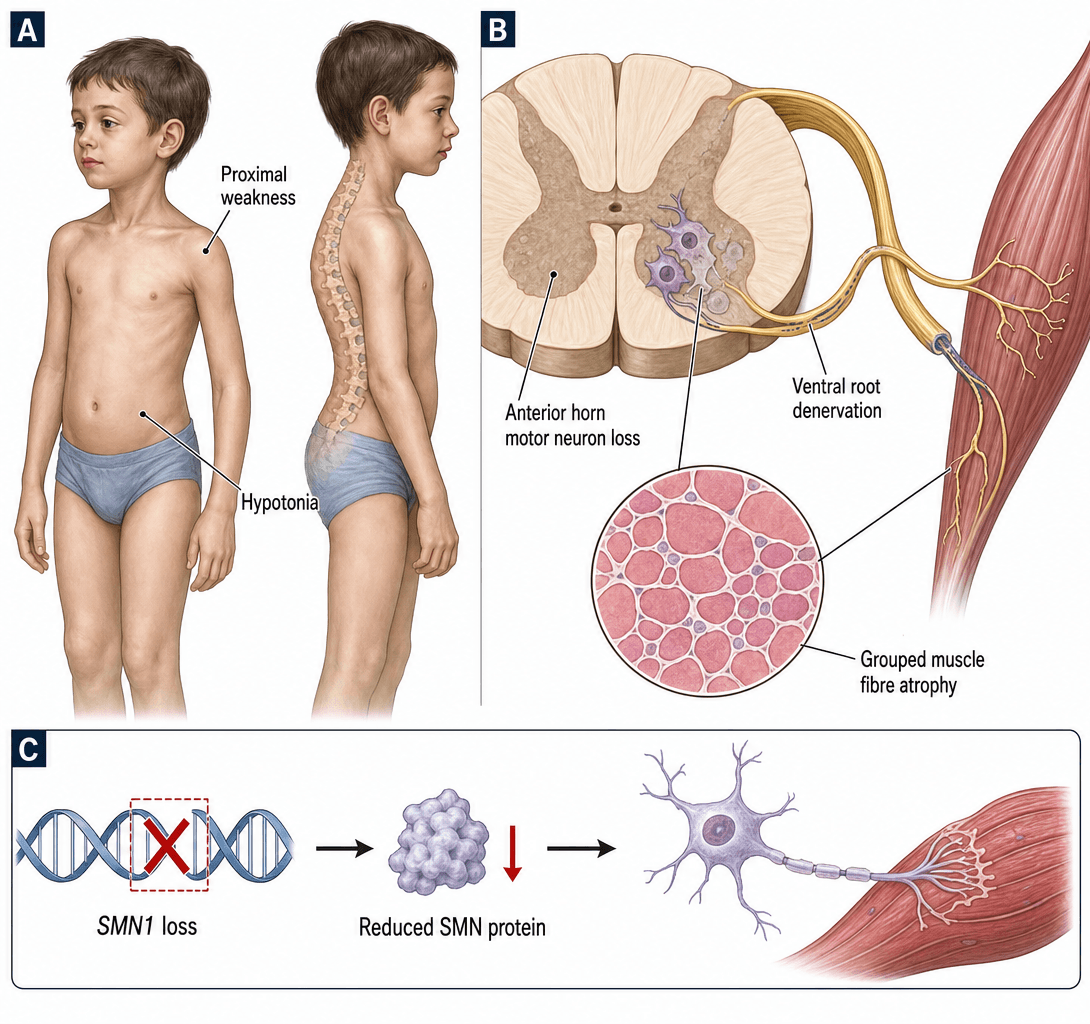
Spinal Muscular Atrophy (SMA) is a progressive neuromuscular disorder.
- Genetics: Autosomal recessive. Mutation/deletion in SMN1 (Survival Motor Neuron 1) gene on chromosome 5q.
- Incidence: Approximately 1 in 11,000 live births (international consensus figure). Carrier frequency roughly 1 in 40-60.
- Pathophysiology: Degeneration of anterior horn cells in the spinal cord leads to progressive weakness.
- Historical Significance: Leading genetic cause of infant death (prior to gene therapy).
Pathophysiology
Spinal Cord Pathology
- Anterior horn cells (lower motor neurons) degenerate.
- Results in denervation of skeletal muscles.
- Proximal muscles affected more than distal.
- Lower limbs typically weaker than upper limbs.
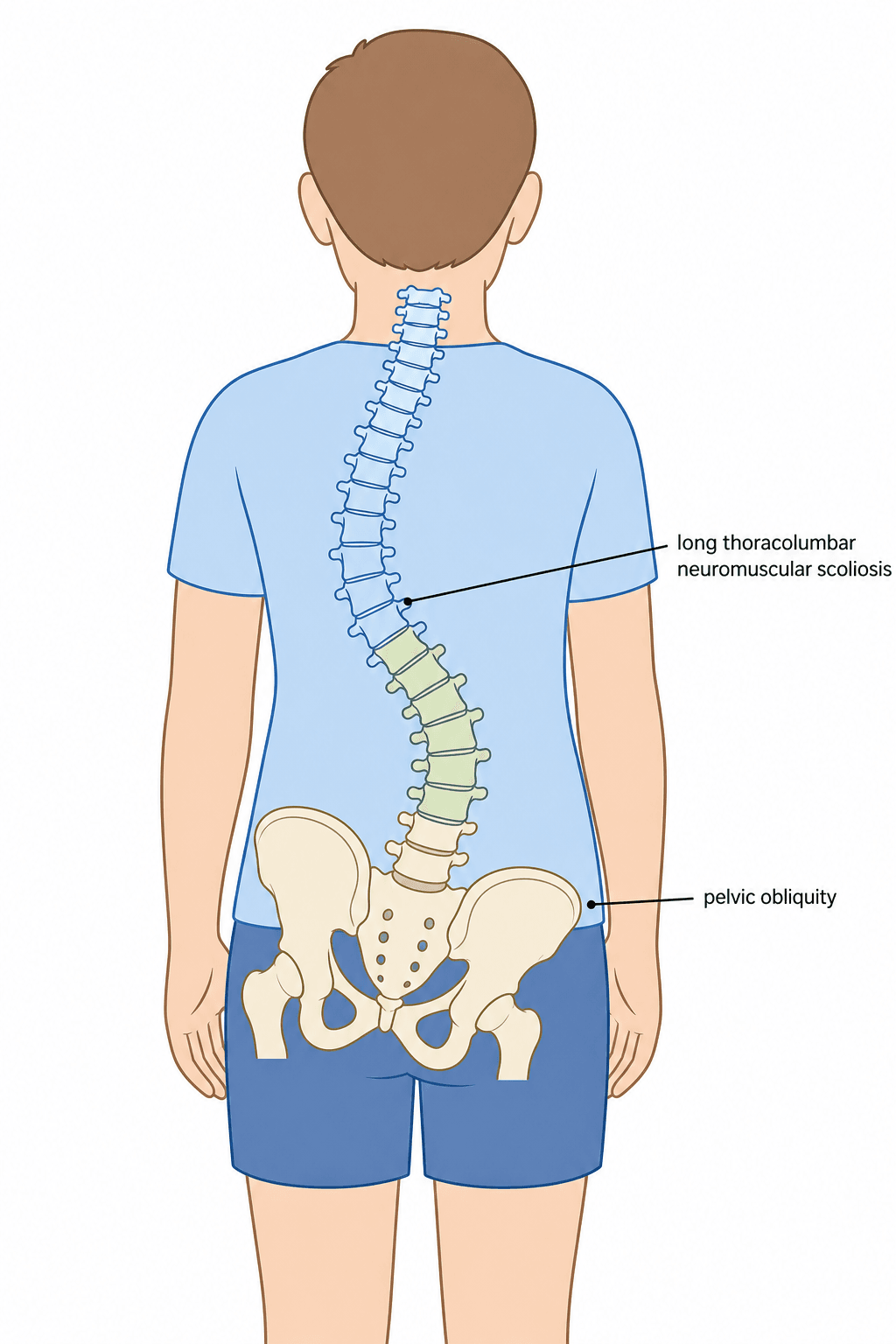
Why Scoliosis Develops
- Trunk muscle weakness leads to spinal collapse.
- Gravity + asymmetric weakness = progressive curve.
- Usually thoracolumbar, long sweeping C-curve.
- Pelvic obliquity is common.
SMN1/SMN2 Molecular Biology
The topic repeatedly invokes "SMN2 copy number predicts severity," "nusinersen increases SMN2 expression," and "risdiplam is an SMN2 splicing modifier" — but these only make sense once the underlying gene biology is explicit.
Two genes, one protein
- SMN1 is the primary gene producing full-length, functional Survival Motor Neuron (SMN) protein. Homozygous loss/mutation of SMN1 causes SMA.
- SMN2 is a near-identical paralogue on the same chromosome 5q region. It differs from SMN1 by a single translationally-silent C-to-T nucleotide change within exon 7.
- That single base change disrupts an exonic splicing enhancer, so most SMN2 transcripts skip exon 7 and produce a truncated, rapidly-degraded protein (SMNΔ7). Only roughly 10 to 15 percent of SMN2 output is full-length functional SMN.
Why copy number is prognostic
- SMN2 is present in variable copy number (1 to 4+ copies). Each extra copy adds a little more full-length SMN, partially compensating for the absent SMN1.
- More SMN2 copies therefore correlate with a milder phenotype: typically 1 to 2 copies in Type 1, 3 copies in Type 2, and 3 to 4 copies in Type 3. (Copy number predicts severity at a population level but is not an absolute individual guarantee.)
Every disease-modifying therapy targets the same bottleneck — raising functional SMN. Nusinersen (intrathecal antisense oligonucleotide) and risdiplam (oral small molecule) both promote exon-7 inclusion so SMN2 makes more full-length protein, while onasemnogene abeparvovec delivers a replacement SMN1 transgene via an AAV9 vector. The disease-specific principles of the gene-replacement platform itself are covered in the gene therapy and tissue engineering topic.
Classification Systems
SMA Type I (Werdnig-Hoffmann Disease)
- Onset: Birth to 6 months.
- Motor Milestones: Never achieves sitting.
- Features: Severe hypotonia, frog-leg posture, paradoxical breathing.
- Prognosis: Without treatment, death by age 2 (respiratory failure).
- With Gene Therapy: Dramatically improved survival.
Clinical Assessment
- Age of symptom onset.
- Motor milestones achieved and lost.
- Family history.
- Respiratory status.
- Hypotonia: Floppy infant (Type I).
- Weakness: Proximal greater than distal. Symmetric.
- Reflexes: Absent or diminished.
- Fasciculations: Tongue fasciculations are characteristic.
- Spine: Assess for scoliosis.
- Hips: Assess for dysplasia, contractures.
Investigations
- SMN1 gene deletion/mutation: Confirmatory.
- SMN2 copy number: Prognostic (more copies = milder phenotype).
- Denervation pattern (rarely needed now with genetic testing).
- FVC (forced vital capacity) monitoring.
- Spine X-ray: Scoliosis assessment.
- Hip X-ray: Dysplasia, subluxation.
Differential Diagnosis
- Inheritance / Cause
- Autosomal recessive, SMN1 deletion (5q)
- Discriminating Features
- Tongue fasciculations, absent reflexes, normal/mildly raised CK, SMN1 testing confirmatory
- Inheritance / Cause
- X-linked, dystrophin gene
- Discriminating Features
- Boys, markedly elevated CK, calf pseudohypertrophy, Gowers sign, preserved early reflexes
- Inheritance / Cause
- Various (e.g. nemaline, central core)
- Discriminating Features
- Static or slowly progressive, normal/mildly raised CK, characteristic muscle biopsy/genetics
- Inheritance / Cause
- Autosomal dominant, DMPK repeat (maternal)
- Discriminating Features
- Facial diplegia, myotonia, maternal symptoms, polyhydramnios history
- Inheritance / Cause
- Tumour, syrinx, cord compression
- Discriminating Features
- Sensory level, asymmetry, sphincter involvement; MRI differentiates
- Inheritance / Cause
- Enzyme deficiency (e.g. Pompe)
- Discriminating Features
- Exercise intolerance, cardiomyopathy (Pompe), specific enzyme/genetic assays
Key Differentiators for SMA: SMN1 genetic testing is confirmatory; tongue fasciculations are characteristic; CK is normal or only mildly elevated; reflexes are absent or diminished.
Management Algorithm
Medical Management
- Gene Therapy (Onasemnogene/Zolgensma): Single IV dose in infants.
- Nusinersen (Spinraza): Intrathecal injections every 4 months.
- Risdiplam (Evrysdi): Oral SMN2 splicing modifier.
- Respiratory Support: BiPAP, cough assist, suctioning.
- Nutritional Support: Gastrostomy if swallowing impaired.
RSGTreatment Principles
Hook:RSG - Respiratory, Scoliosis, Gene therapy.
Surgical Techniques
Posterior Spinal Fusion
Indications: Progressive scoliosis greater than 40-50 degrees with adequate pulmonary function.
Technique: Posterior approach. Long fusion from upper thoracic to pelvis (typically T2-pelvis). Pelvic fixation (iliac screws or S2-alar-iliac screws) is essential due to pelvic obliquity. Use of hybrid constructs or all-screw constructs.
Considerations: High perioperative risk due to respiratory compromise. Anesthesia team experienced in neuromuscular scoliosis is essential.
Anaesthetic & Perioperative Considerations
The surgical sections repeatedly flag "high perioperative risk," an "experienced anaesthesia team," respiratory optimisation, ICU and prolonged ventilation — but the specific principles that drive those statements deserve to be explicit, because in SMA the airway and ventilation, not the spine, are what threaten the patient.
Respiratory — the dominant concern
- Restrictive lung disease from intercostal weakness gives a low and falling forced vital capacity (FVC); a low pre-operative FVC predicts post-operative ventilatory dependence.
- Pre-operative optimisation: treat chest infection, nutritional support, and training with non-invasive ventilation (NIV/BiPAP) and mechanical cough-assist before surgery.
- Plan for elective post-operative NIV and aggressive secretion clearance rather than reactive re-intubation; protocolised extubation directly onto NIV reduces re-intubation after scoliosis fusion.
Airway, drugs and monitoring
- Bulbar weakness and impaired cough mean a real aspiration risk — careful airway protection and secretion management.
- Avoid depolarising neuromuscular blockers (suxamethonium): denervated/atrophic muscle carries up-regulated extrajunctional acetylcholine receptors and risks life-threatening hyperkalaemia.
- Expect heightened and prolonged sensitivity to non-depolarising relaxants and to opioids/sedatives — titrate carefully, use quantitative neuromuscular monitoring, and ensure full reversal.
- Long instrumented fusions carry significant blood loss; plan cross-match, cell salvage and neuromonitoring, and anticipate intensive-care recovery.
A classic examiner trap: SMA is a denervating motor-neuron disease and is not associated with malignant hyperthermia, so volatile agents are not contraindicated on MH grounds — but suxamethonium is still avoided because of the hyperkalaemia risk in chronically denervated muscle. (The MH syndrome itself, its triggers and dantrolene management, is dealt with in the malignant hyperthermia topic, and the general conduct of anaesthesia in the general anaesthesia in orthopaedics topic.)
Complications
- Context
- Primary cause of death
- Management
- BiPAP, ventilation, cough assist
- Context
- Universal in Type I/II
- Management
- Bracing, surgery
- Context
- Common in Type I/II
- Management
- Usually observation
- Context
- Hips, knees, feet
- Management
- Stretching, splinting, releases
- Context
- High risk for scoliosis surgery
- Management
- Experienced team, ICU care
Postoperative Care
- ICU Admission: For scoliosis surgery.
- Respiratory: May require prolonged ventilation.
- Mobilization: Early sitting in wheelchair.
- Pain Management: Multimodal.
- Long-Term: Bracing discontinued after fusion. Ongoing respiratory and nutritional support.
Outcomes/Prognosis
- Type I (Untreated): Death by 2 years.
- Type I (Gene Therapy): Many achieving motor milestones, survival dramatically improved.
- Type II: Survive to adulthood with respiratory support.
- Type III/IV: Normal or near-normal lifespan.
- Scoliosis Surgery: Improves sitting balance, quality of life, may improve respiratory function.
Guidelines, Registries & Global Practice
Global epidemiology
- Incidence approximately 1 in 11,000 live births; pan-ethnic, with carrier frequency roughly 1 in 40-60.
- SMN2 copy number is the principal genetic modifier worldwide: 2 copies predict the most severe phenotype, while 3 or more copies predict milder disease.
Major guidelines, side by side
- Scope
- Diagnosis, orthopaedic, rehabilitation, nutrition
- Key recommendation
- Manage by functional status (non-sitter/sitter/walker); growth-friendly instrumentation early, fusion to pelvis once growth adequate
- Scope
- Pre-symptomatic detection
- Key recommendation
- Population SMN1 screening enables treatment before motor-neuron loss; best outcomes when treated pre-symptomatically
- Scope
- Disease-modifying therapy
- Key recommendation
- Three approved DMTs (onasemnogene, nusinersen, risdiplam); choice driven by age, weight, SMN2 copies and access
- Scope
- Surgical timing
- Key recommendation
- Long fusion to pelvis for sitters; preserve intrathecal access if continuing nusinersen
Registries & access
- No single global SMA implant registry; outcome data come from national neuromuscular registries (e.g. TREAT-NMD, SMArtCARE in Europe, Cure SMA in North America) and tertiary-centre series.
- Newborn screening for SMA is now established across much of North America, Europe and parts of Asia-Pacific, but coverage remains uneven globally.
High- vs limited-resource practice variation
- High-resource settings: newborn screening, early disease-modifying therapy, MAGEC/growth-friendly constructs, intrathecal-access-preserving fusion, ICU-supported neuromuscular spine surgery.
- Limited-resource settings: diagnosis often clinical or delayed; disease-modifying drugs frequently unaffordable; management centres on respiratory support, seating, contracture care, and fusion where safe perioperative care exists.
Controversies & Areas of Uncertainty
- Spinal surgery in the gene-therapy era: Disease-modifying therapy is reducing curve severity in early-treated children, but it is unclear whether it will eliminate the need for fusion or merely delay it. Long-term natural history of the treated cohort is still being defined.
- Timing of fusion vs growth-friendly constructs: When to convert magnetically controlled growing rods to definitive fusion, and whether early definitive fusion in older children is preferable, remains debated; both strategies show durable correction in current series.
- Preserving intrathecal access: Nusinersen requires repeated intrathecal injection, so "skip" or fenestrated constructs and laminotomy windows are used to keep access; the optimal technique and whether oral risdiplam removes this constraint are unresolved.
- Pulmonary outcome of fusion: Fusion reliably improves sitting and halts deformity, but vital capacity often falls rather than improves after surgery — the respiratory benefit is mainly preservation, not gain.
- Lower FVC threshold for surgery: There is no universally agreed FVC cut-off; very low FVC raises perioperative risk but is not an absolute contraindication when seating and quality of life are at stake.
- Hip management: Whether asymptomatic hip subluxation/dislocation ever warrants reconstruction in non-ambulators is contested; most centres observe because reconstruction has high redislocation rates and limited functional gain.
MCQ Practice Points
Q: What gene is mutated in SMA? A: SMN1 (Survival Motor Neuron 1) on chromosome 5q.
Q: A child who can sit but never walks has which SMA type? A: Type II.
Q: What correlates with disease severity? A: SMN2 copy number - more copies = milder phenotype.
Q: What is the mechanism of nusinersen (Spinraza)? A: Antisense oligonucleotide that increases SMN2 expression.
Q: What is the extent of fusion in SMA scoliosis surgery? A: T2 to pelvis with pelvic fixation (S2-alar-iliac or iliac screws).
Q: How should hip dysplasia in SMA be managed? A: Observation - surgery rarely indicated due to high failure rate and minimal functional benefit.
Self-Assessment Quiz
Additional Quiz Questions
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“8-month-old with confirmed SMA Type I. Has received gene therapy. Now developing thoracolumbar scoliosis of 30 degrees.”
“14-year-old with SMA Type II. Wheelchair-dependent. Thoracolumbar scoliosis of 80 degrees with pelvic obliquity. FVC 35%.”
“Same patient also has bilateral hip subluxation on X-ray. Is this an indication for surgery?”
GENETICS
- SMN1 Mutation
- Autosomal Recessive
- SMN2 Copies = Prognosis
- Chromosome 5q
TYPES
- I: Never sits
- II: Sits, never walks
- III: Walks
- IV: Adult onset
ORTHO ISSUES
- Scoliosis (universal)
- Hip Dysplasia
- Contractures
- Pelvic Obliquity
SCOLIOSIS SURGERY
- T2 to Pelvis Fusion
- Pelvic Fixation Essential
- High Perioperative Risk
- ICU Postop Care
MEDICAL THERAPY
- Onasemnogene (Gene Therapy)
- Nusinersen (Intrathecal)
- Risdiplam (Oral)
- Early Treatment Best
EXAM PEARLS
- Tongue Fasciculations
- 100% Scoliosis in Type I/II
- Hip Surgery Rarely Indicated
- FVC Monitoring Critical
Evidence Base
- Single IV dose of AAV9-SMN gene therapy in 15 infants with SMA type 1
- All 15 alive and event-free at 20 months vs 8% survival in a historical cohort
- High-dose cohort: CHOP INTEND rose 15.4 points by 3 months; 11 of 12 sat unassisted, 2 walked
- Transient transaminitis attenuated by prednisolone
- Randomised, double-blind, sham-controlled phase 3 trial of intrathecal nusinersen in infantile-onset SMA
- Motor-milestone response 51% (37/73) vs 0% (0/37) in controls
- Hazard ratio for death or permanent ventilation 0.53 (P=0.005)
- Trial stopped early at interim analysis for efficacy
- Open-label trial of oral risdiplam in 41 infants with type 1 SMA (2 SMN2 copies)
- At 24 months, 44% (18/41) sat without support for at least 30 seconds vs a 5% natural-history threshold
- No infant achieved standing or independent walking
- Most common serious adverse events were pneumonia (39%) and respiratory distress
- Consensus update on diagnosis, rehabilitation, orthopaedic/spinal and nutritional care
- SMA incidence approximately 1 in 11,000 live births
- Spinal management framed by functional status (non-sitter / sitter / walker)
- Recommends growth-friendly instrumentation in young children and definitive fusion to pelvis once growth is adequate
- 22 SMA patients with curves over 100 degrees and pelvic obliquity over 20 degrees, one-stage PSF with pelvic fixation
- Independent sitting improved from 22.7% preoperatively to 77.3% postoperatively (P less than 0.001)
- Mean FVC remained stable; 50% improved
- Perioperative complications in 27.3% (pneumonia, epiglottic oedema, delayed wound healing); none needed reoperation
- 26 SMA type 2 patients: 17 magnetically controlled growing rods (MCGR), 9 posterior spinal fusion (PSF)
- Major curve correction 44% (MCGR) and 55% (PSF); pelvic obliquity under 5 degrees in all at follow-up
- Pelvic fixation by T-construct (2 sacral plus 2 iliac screws); lung function unchanged by either procedure
- Low complication rate; all patients improved sitting ability
- Modified PSF skipping a thoracolumbar level to preserve intrathecal access for nusinersen
- 8 patients, mean curve correction 35.2 degrees, 4-year follow-up
- No rod breakage or loss of correction; one revision for bony overgrowth at the skipped level
- Pulmonary function before and after PSF in neuromuscular disease
- All 6 SMA patients lost vital capacity (mean loss 0.63 L)
- Contrasts with merosin-deficient dystrophy, which gained VC