Peroneal Spastic Flatfoot
- Definition: Abnormal connection between two tarsal bones (Fibrous, Cartilaginous, or Osseous).
- Presentation: Rigid flatfoot, frequent ankle sprains, 'Peroneal Spastic Flatfoot'.
- Onset: Symptoms start when the coalition ossifies (stiffens). 8-12y for CN, 12-16y for TC.
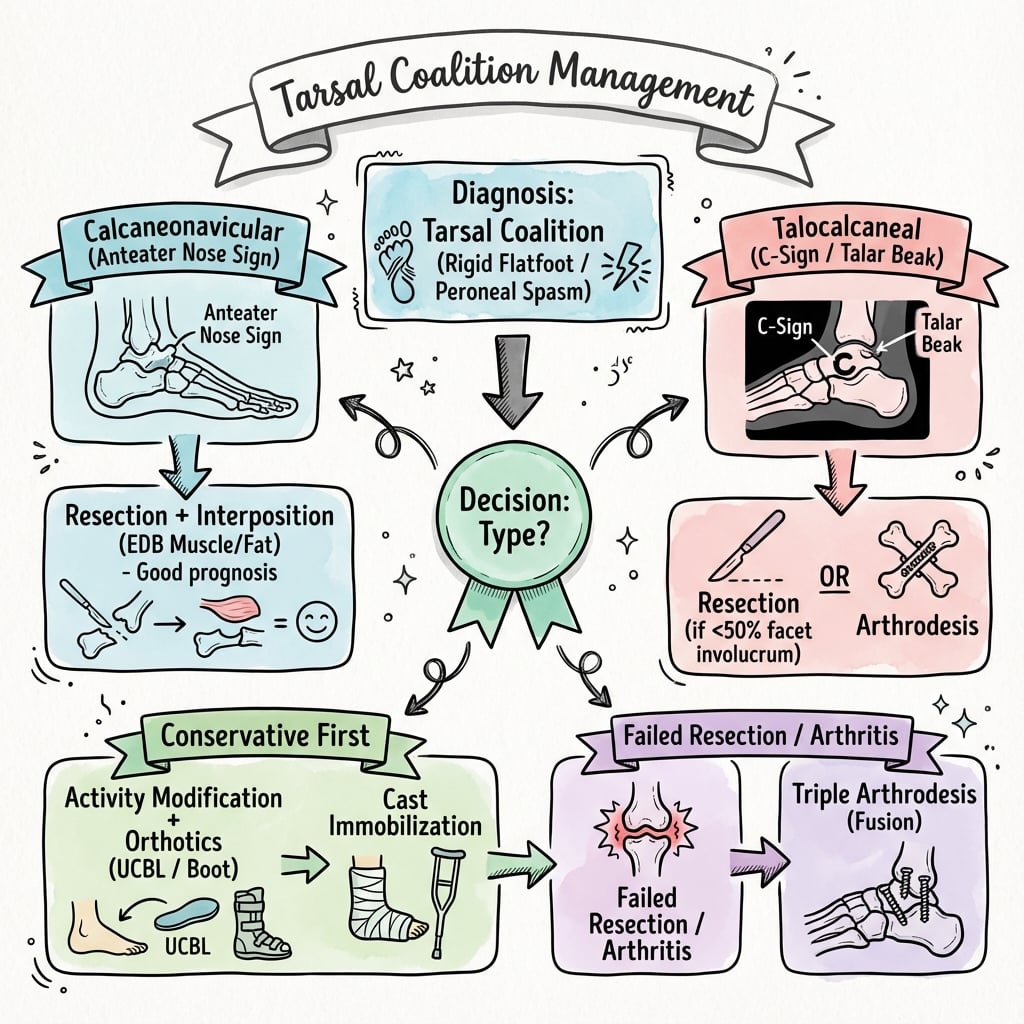
- X-ray Signs: Anteater Nose (CN), C-Sign (TC), Talar Beaking (Dorsal).
- Treatment: Conservative (Rest/Cast) → Resection (if under 50% of joint) → Fusion (Triple/Subtalar).
- “CN coalition ossifies FIRST (8-12y), TC coalition LATER (12-16y).
- “Anteater Nose Sign = CN Coalition (elongated anterior calcaneus).
- “C-Sign = TC Coalition (continuity of talus/calcaneus on lateral).
- “Resection of TC coalition is only viable if under 50% of the joint is involved and no arthrosis.
- “Bilateral in 50% of cases.
'Ankle Sprains'. Recurrent ankle sprains in an adolescent with a flat foot → Think Coalition.
Not the Coalition. Talar beak is a traction spur from abnormal motion/stress. It is NOT the coalition itself.
The 50% Rule. Do not resect TC coalitions if over 50% of the middle facet is involved. Outcome is poor. Fuse instead.
Not True Spasm. It is adaptive shortening of the peroneals due to the valgus deformity.
- Calcaneonavicular (CN)
- Common (45%)
- Talocalcaneal (TC)
- Common (45%)
- Calcaneonavicular (CN)
- 8 - 12 years
- Talocalcaneal (TC)
- 12 - 16 years
- Calcaneonavicular (CN)
- Anterior Calcaneus - Navicular
- Talocalcaneal (TC)
- Middle Facet (Sustentaculum)
- Calcaneonavicular (CN)
- Anteater Nose
- Talocalcaneal (TC)
- C-Sign
- Calcaneonavicular (CN)
- Oblique Foot
- Talocalcaneal (TC)
- Lateral Foot / Harris Axial
- Calcaneonavicular (CN)
- Excellent (Resection)
- Talocalcaneal (TC)
- Variable (Resection vs Fusion)
RICEResection Steps
Hook:RICE for Resection success.
Overview and Epidemiology
A failure of segmentation between two or more tarsal bones, producing a fibrous (syndesmosis), cartilaginous (synchondrosis), or osseous (synostosis) bridge.
- Incidence: Less than 1% of population.
- Genetics: Autosomal Dominant with variable penetrance.
- Laterality: Bilateral in 50% of cases.
- Types: CN and TC make up greater than 90% of all coalitions.
- Congenital problem, but asymptomatic in young children because the coalition is cartilaginous/fibrous and allows motion.
- Symptoms start when the coalition ossifies (turns to bone) and becomes rigid, restricting subtalar motion.
- Peroneal Spastic Flatfoot: Rigid valgus foot causes shortening/tightness of peroneal tendons (not true spasm).
Aetiology and Anatomy
- Failure of differentiation and segmentation of primitive mesenchyme is the leading theory.
- Most cases are isolated and autosomal dominant. Coalitions also occur as part of syndromes (fibular hemimelia, Apert, Nievergelt-Pearlman, and other limb-deficiency / proximal focal femoral deficiency phenotypes) where multiple coalitions are common.
- The bar starts as fibrous or cartilaginous tissue that permits some motion; the foot is therefore asymptomatic in early childhood.
- As the bridge ossifies (CN typically 8-12 yr, TC 12-16 yr) it stiffens, abolishing subtalar motion and transferring stress to neighbouring joints and ligaments.
- The rigid valgus hindfoot causes adaptive shortening of the peroneal tendons ("peroneal spastic flatfoot" — a misnomer, as it is contracture, not true spasticity).
- CN coalition bridges the anterior process of the calcaneus to the lateral/dorsal navicular; the extensor digitorum brevis (EDB) origin overlies it and is the workhorse interposition tissue.
- TC coalition almost always involves the middle facet (sustentaculum tali). The flexor hallucis longus runs beneath the sustentaculum, and the posterior tibial neurovascular bundle and FDL/tibialis posterior tendons lie just medial — all at risk during medial resection.
Classification Systems
- Calcaneonavicular (CN) — ~45-50%. Ossifies 8-12 yr. Anteater-nose sign on lateral, best profiled on the oblique view.
- Talocalcaneal (TC) — ~45-50%. Ossifies 12-16 yr. Almost always the middle facet. C-sign on lateral; CT defines extent.
- Other (rare) — talonavicular, calcaneocuboid, cubonavicular. Multiple coalitions occur in syndromic feet.
Clinical Assessment
- Pain: Vague hindfoot/midfoot pain, worse with activity.
- Stiffness: "My foot doesn't move right."
- Sprains: Recurrent ankle sprains (rigid hindfoot can't accommodate uneven ground).
- Deformity: Progressive flatfoot.
- Inspection: Rigid Flatfoot (Pes Planus). Valgus heel.
- Motion:
- Restricted Subtalar Motion (Inversion/Eversion).
- Locking: Foot may be locked in valgus.
- Tender:
- Sinus Tarsi (CN).
- Medial Malleolus/Sustentaculum (TC).
- Toe Raise Test: Heel remains in valgus (does not invert) → Indicates RIGID flatfoot.
Investigations
- Lateral:
- C-Sign: Continuous C-shaped line from talar dome to sustentaculum tali (TC coalition).
- Talar Beak: Dorsal spur on talar head (sign of increased stress, not the coalition).
- Anteater Nose: Elongated anterior process of calcaneus (CN coalition).
- Oblique (Slanted): Best for CN coalition.
- Harris Axial: Can show TC coalition (middle facet angulation).
- Confirms diagnosis.
- Defines location and extent.
- Assesses % of joint involvement (Critical for TC).
- Look for degenerative changes.
- Useful for fibrous/cartilaginous coalitions (non-ossified) if CT negative but high suspicion.


Indirect Radiographic Signs of TC Coalition
The topic names the C-sign, the talar beak and "middle-facet angulation on the Harris view" piecemeal, but the reason these matter deserves to be assembled. Unlike the calcaneonavicular bar — where the anteater nose is a direct bony sign — the talocalcaneal coalition sits at the middle facet and is frequently fibrous or cartilaginous (non-osseous), so there is often no directly visible bony bridge on plain film. Diagnosis therefore rests on indirect signs that betray the abnormal subtalar mechanics, and any one of them should trigger the confirmatory CT.
- What it is
- Continuous C-shaped line: medial talar dome curving into the inferior sustentaculum tali
- Why it occurs
- The enlarged sustentaculum is bridged to the talus, fusing the two outlines into one ring
- What it is
- The normal clear lucent line of the middle subtalar facet cannot be seen
- Why it occurs
- The facet is bridged/obliterated by the coalition, so its joint line disappears
- What it is
- Broad, rounded, dysplastic sustentaculum tali
- Why it occurs
- Altered load and failed segmentation remodel the sustentaculum
- What it is
- Dorsal beak on the talar head/neck
- Why it occurs
- Traction/periosteal response to abnormal motion — NOT the coalition and NOT a bar to resection
- What it is
- Joint-space loss, sclerosis, talus abutting calcaneus
- Why it occurs
- Late degenerative change in long-standing or large coalitions
- What it is
- Rounded (domed) talar dome and tibial plafond
- Why it occurs
- Compensatory ankle motion develops to replace the stiff subtalar joint
Putting it together: in a rigid adolescent flatfoot, the absent middle-facet sign and the C-sign are the two that most reliably point to a TC coalition; the talar beak and posterior-facet changes are supportive but less specific. None of these replaces cross-sectional imaging — they are the prompt for it. CT remains the reference standard for confirming the bar, quantifying the percentage of facet involvement and heel valgus (the resectability question), and excluding a second (double) coalition; MRI is reserved for the purely fibrous/cartilaginous bar that CT cannot show as bone.
A middle-facet TC coalition is commonly non-osseous, so do not expect to "see the bar" on plain film. Hunt for the indirect signs — absent middle-facet sign and C-sign first — then confirm and size it on CT. A talar beak is reactive, not the coalition, and (per Wilde) does not by itself contraindicate resection.
CN-TCCoalition Onset Age
Hook:CN = 9-12. TC = Teens.
Ant-CX-ray Signs
Hook:Anteater for CN, C for TC.
Differential Diagnosis
The cardinal task is separating a rigid painful flatfoot (coalition) from the far more common flexible flatfoot and from other causes of a stiff adolescent hindfoot.
- Key Discriminator
- Onset 8-16 yr, recurrent sprains, heel stays valgus on toe-raise
- Subtalar Motion
- Reduced / absent
- Confirmatory Test
- CT (TC) or oblique X-ray (CN)
- Key Discriminator
- Arch reconstitutes on tiptoe / Jack test; usually painless
- Subtalar Motion
- Normal / supple
- Confirmatory Test
- Clinical (mobile, correctable)
- Key Discriminator
- Medial midfoot pain over navicular, painful single-heel-rise
- Subtalar Motion
- Often preserved
- Confirmatory Test
- X-ray accessory ossicle, MRI tendon
- Key Discriminator
- Morning stiffness, effusion, other joints, raised inflammatory markers
- Subtalar Motion
- Reduced (effusion/synovitis)
- Confirmatory Test
- MRI synovitis, serology
- Key Discriminator
- Focal bony tenderness, age-specific apophysis/ossific changes
- Subtalar Motion
- Usually preserved
- Confirmatory Test
- MRI / focal X-ray
- Key Discriminator
- Night pain, NSAID-responsive (osteoid osteoma), systemic signs
- Subtalar Motion
- Variable
- Confirmatory Test
- MRI / thin-slice CT / bloods
Management Algorithm
Conservative Management
- Indication: Initial presentation, Mild symptoms.
- Modalities:
- Activity Modification: Avoid uneven ground.
- Immobilization: Short leg walking cast (3-6 weeks) to settle inflammation.
- Orthotics: UCBL or medial arch support (rigid support).
- Success: ~30% may resolve or become manageable without surgery.
Hindfoot Valgus: Resect, Realign, or Fuse
The resection criteria ("no severe valgus, more than 16 to 20 degrees") and the controversies section both invoke the hindfoot valgus deformity, but the management body never develops the key point: bar resection restores motion and relieves pain, but it does not by itself correct a fixed hindfoot valgus. The flatter and more valgus the heel, the worse resection alone performs — Wilde's poor-outcome group all had heel valgus more than 16 degrees. So the decision is not simply "resect vs fuse" but a three-way choice driven by the deformity as much as by the coalition size.
- Operation
- Resection + interposition alone
- Rationale
- Motion restored; alignment acceptable, no correction needed
- Operation
- Resection + a deformity-correcting hindfoot osteotomy
- Rationale
- Realigns the heel so the resection is not loaded into valgus; preserves the joints
- Operation
- Arthrodesis (subtalar or triple)
- Rationale
- Fusion both removes the painful joint and corrects the alignment
Assess the deformity before choosing: standing heel valgus, forefoot abduction ("too many toes" sign), and how much of it is flexible (correctable on tiptoe / Coleman block) versus fixed, supported by weight-bearing imaging. A correctable valgus accompanying a resectable bar is the classic indication for adding a realigning osteotomy (for example a lateral column lengthening or a medialising calcaneal osteotomy) at the time of resection. The general technique and indications for these flatfoot-reconstruction osteotomies are developed in the flatfoot topics; here the coalition-specific point is simply that significant valgus must be addressed, not ignored. Whether to perform the osteotomy at the index resection or stage it remains debated.
Excising the coalition restores subtalar motion but will not correct a fixed valgus heel. If there is significant hindfoot valgus, either add a realigning osteotomy to a resectable bar or, for an unresectable/arthritic coalition or a rigid deformity, fuse and correct — do not expect resection alone to do it.
Surgical Technique
CN Coalition Resection
- Incision: Ollier's (Lateral oblique over sinus tarsi).
- Identify: EDB muscle belly. Reflect it.
- Excise: Identify the coalition bar (calcaneus to navicular). Excise a generous rectangular block (1cm minimum) to prevent regrowth.
- Check: Verify navicular and calcaneus surfaces are clear. Check motion.
- Interpose: Sew EDB muscle origin into the defect (anchored to deep tissue/plantar aspect).
- Post-op: Cast 2 weeks then early ROM.
Complications
Complications of Surgery
- Cause
- Inadequate resection (greater than 50% remaining)
- Prevention
- Resect greater than 1cm block, Interposition (EDB/Fat)
- Cause
- Degenerative changes, Missed double coalition
- Prevention
- Pre-op CT calc, Triple Fusion if arthrosis
- Cause
- Lateral approach incision
- Prevention
- Identify nerve, careful retraction
- Cause
- Medial approach tension
- Prevention
- Gentle retraction
Complications of Non-Treatment
- Progressive Valgus deformity.
- Peroneal tendon contracture/shortening.
- Subtalar and TN joint arthritis.
Postoperative Care
Protocol:
- Immobilization: Initial splinting/casting to protect the repair/fracture.
- Rehabilitation: Gradual Range of Motion (ROM) and strengthening as healing progresses.
- Weight Bearing: Progression depends on stability of fixation and healing.
Outcomes
- CN Resection: Usually very successful. Pain relief and improved motion.
- TC Resection: success depends on size (less than 50%). If greater than 50%, consider primary fusion.
- Recurrence: Bone can regrow. Interposition material helps prevent this.
Guidelines, Registries & Global Practice
Global epidemiology
- Population prevalence is classically quoted as under 1%, but cadaveric and CT studies suggest the true figure may approach 1-13%, with many coalitions remaining asymptomatic. CN and TC together account for over 90% of cases; bilateral in roughly 50%.
- Slight male predominance; autosomal-dominant inheritance with variable penetrance.
Society guidance — practical points (no dedicated coalition guideline exists)
- Imaging emphasis
- Weight-bearing X-rays first; CT to map TC extent, MRI for fibrous/cartilaginous bars
- Treatment stance
- Non-op trial, then joint-preserving resection; fusion as salvage
- Imaging emphasis
- Oblique view for CN, CT for TC sizing
- Treatment stance
- Same staged approach; emphasis on realistic counselling re: stiffness
- Imaging emphasis
- CT and increasingly MRI to characterise tissue type and arthritis
- Treatment stance
- Growing interest in arthroscopic/endoscopic resection
- Imaging emphasis
- CT remains the reference standard for resectability decisions
- Treatment stance
- Resect when criteria met; preserve motion where possible
Registry note: There is no national registry specific to tarsal coalition; outcome data come from single-centre series and the Garg 2023 systematic review rather than arthroplasty-style registries.
High- vs limited-resource practice
- Where CT/MRI is freely available, the resect-vs-fuse decision is CT-driven. In limited-resource settings the diagnosis often rests on plain radiographs (oblique for CN, Harris axial and lateral C-sign for TC) plus clinical examination, and management leans on prolonged casting/orthoses with surgery reserved for refractory cases.
- Terminology: Historically "peroneal spastic flatfoot"; "rigid (painful) flatfoot" is preferred, as the peroneal tightness is contracture, not spasticity.
Controversies & Areas of Uncertainty
- Resection thresholds for TC: The classic 50% facet / 16-degree valgus cut-offs (Wilde) are widely taught, but Luhmann & Schoenecker reported good outcomes in some feet exceeding these limits and argued the CT criteria should guide counselling, not absolute operative choice. There is no level-I evidence defining a hard cut-off.
- Best interposition material: EDB, fat graft, bone wax and vascularised adipofascial flaps have all been used. Fat-graft and EDB give comparable results; any interposition appears better than none for reducing reossification, but no randomised comparison exists.
- Arthroscopic / endoscopic resection: Posterior arthroscopic TC resection (Knörr) and endoscopic CN resection are emerging, with good early series and complete resection without recurrence — but follow-up is short and the technique demanding.
- Concomitant deformity correction: Whether to add a calcaneal lengthening / medialising osteotomy for marked hindfoot valgus at the time of resection (rather than relying on resection alone) is debated.
- Fusion vs joint-preservation in large/arthritic TC: When resection is unsuitable, subtalar versus triple arthrodesis (and timing in the growing foot) remains individualised.
MCQ Practice Points
Q: Which coalition presents earlier? A: Calcaneonavicular (8-12 years). Talocalcaneal presents later (12-16 years).
Q: What is the 'Anteater Nose' sign? A: Elongation of the anterior process of the calcaneus, seen on lateral X-ray, indicated Calcaneonavicular coalition.
Q: What does the C-Sign indicate? A: Talocalcaneal coalition. A continuous C-shaped line formed by the medial outline of the talar dome and inferior outline of the sustentaculum tali on lateral X-ray.
Q: What is the size cutoff for resecting a TC coalition? A: 50%. If over 50% of the facet is involved, resection has poor outcomes. Fusion is preferred.
Q: What happens to the heel during a toe raise test in tarsal coalition? A: The heel stays in Valgus (does NOT invert). This indicates a RIGID flatfoot. (In flexible flatfoot, the heel inverts).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“What is the diagnosis and workup?”
“Can you resect this?”
“What do you advise, and what is the evidence for non-operative care?”
Key Features
- Rigid Flatfoot
- Age 8-16 (Ossification)
- Bilateral 50%
- Recurrent Sprains
CN Coalition
- 8-12 years
- Anteater Nose
- Oblique View
- Resection Excellent
TC Coalition
- 12-16 years
- C-Sign
- CT Essential
- Less than 50% to Resect
Management
- Cast 4-6wks first
- Resect CN + EDB
- Resect TC (Small)
- Fuse TC (Large)
Evidence Base
The 50% Rule for TC Resection
- 20 feet (17 patients under 16 yr) with symptomatic TC coalition treated by bar resection.
- Excellent/good results in the 10 feet where coronal CT showed coalition area 50% or less of the posterior facet, with heel valgus under 16 degrees and no arthritis.
- Fair/poor results in the 10 feet where coalition exceeded 50% of the posterior facet (heel valgus over 16 degrees, joint narrowing, lateral talar impingement).
- Talar beaking present in 70% but did not impair outcome.
Anteater-Nose Sign (CN)
- Anterior tubular prolongation of the superior calcaneus ('anteater nose') approaching/overlapping the navicular on the lateral film.
- Present in all 30 feet with calcaneonavicular bar but in none of 125 control feet (second-decade children).