Rare Long Bone Deficiency | Jones Classification | Knee Functionality Key | Synostosis vs Amputation
- Jones classification: Type IA-IV based on tibial presence and knee functionality
- Key decision: knee functionality - non-functional knee (Type IA) = amputation, functional knee (IB/II) = synostosis + Syme
- Type IB vs IA differentiation: USS/MRI essential - IB has proximal cartilage (preserve knee), IA has no tibia (amputation)
- Proximal tibiofibular synostosis: Creates stable knee joint when proximal tibia present (IB/II)
- Treatment timing: Amputation at 6 months - 1 year, synostosis when sufficient ossification
- “Key decision is knee functionality - non-functional (Type IA) = amputation, functional (IB/II) = synostosis + Syme
- “Type IB vs IA: Must differentiate with USS/MRI - IB has cartilage (preserve), IA has nothing (amputate)
- “Proximal tibiofibular synostosis preserves knee function when proximal tibia present
- “Jones Type IA and II are most common - know these well
Key decision: knee functionality - non-functional knee (Type IA, absent tibia) = amputation. Functional knee (Type IB/II, proximal tibia present) = proximal tibiofibular synostosis + Syme amputation. This is the most critical assessment.
Type IB vs IA: Must differentiate with USS/MRI - Type IB has proximal cartilage (preserve knee with synostosis), Type IA has no tibia at all (amputation). Clinical exam and X-ray alone insufficient - imaging essential.
Synostosis procedure: When proximal tibia present (IB/II), create proximal tibiofibular synostosis to provide stable knee joint. Fibula becomes weight-bearing bone. Then perform Syme amputation distally. Preserves knee function.
Amputation timing: 6 months to 1 year of age for Type IA. Synostosis timing: When sufficient ossification present (usually 1-2 years). Early treatment allows prosthetic fitting and development.
- Tibial Status
- Absent tibia
- Knee Function
- Non-functional
- Treatment
- Amputation
- Tibial Status
- Proximal cartilage only
- Knee Function
- Functional (preserve)
- Treatment
- Synostosis + Syme
- Tibial Status
- Ossified proximal tibia
- Knee Function
- Functional (preserve)
- Treatment
- Synostosis + Syme
- Tibial Status
- Ossified distal only
- Knee Function
- Variable
- Treatment
- Syme or Chopart
- Tibial Status
- Short tibia, diastasis
- Knee Function
- Variable
- Treatment
- Syme amputation
Overview and Epidemiology
Tibial hemimelia is a rare congenital deficiency characterized by partial or complete absence of the tibia. It is much rarer than fibular hemimelia and represents one of the most challenging conditions in pediatric orthopedics, with treatment decisions based primarily on knee functionality.
- Incidence: 1 in 1,000,000 live births (very rare)
- Male to female ratio: 1.5:1
- Bilateral involvement: 30% of cases
- Right and left sides: Equal distribution
- Much rarer than fibular hemimelia (1:40,000)
Tibial hemimelia results from failure of normal tibial development during embryogenesis. The exact cause is unknown but may involve:
- Vascular insult during development
- Genetic factors (rare familial cases)
- Teratogenic exposure
- Failure of mesenchymal condensation
The condition represents a spectrum from complete absence (Type IA) to partial presence (Type IB-IV), with Jones classification describing severity based on tibial presence and knee functionality.
Pathophysiology and Mechanisms
Why the tibia matters. The tibia normally carries roughly 85-90% of axial load and stabilises both the knee (proximal articulation with the femur via the medial tibial plateau and cruciates) and the ankle (distal articulation with the talus). Its loss therefore produces a predictable triad of problems whose location depends on which part of the tibia is missing.
Consequences by deficiency pattern:
- Joint affected
- Knee
- Functional consequence
- Knee instability, fixed flexion contracture, no extensor pull if quadriceps/patella absent
- Joint affected
- Ankle
- Functional consequence
- Ankle instability, the fibula migrates proximally, severe varus foot
- Joint affected
- Knee + ankle
- Functional consequence
- Non-weight-bearing limb, marked shortening, the fibula lies lateral and proximally displaced
The decisive structures are therefore the proximal tibial anlage (bony or cartilaginous), the patella and an active quadriceps mechanism - their presence determines whether a stable knee can be salvaged. The fibula is almost always present and frequently becomes the load-bearing strut after reconstruction.
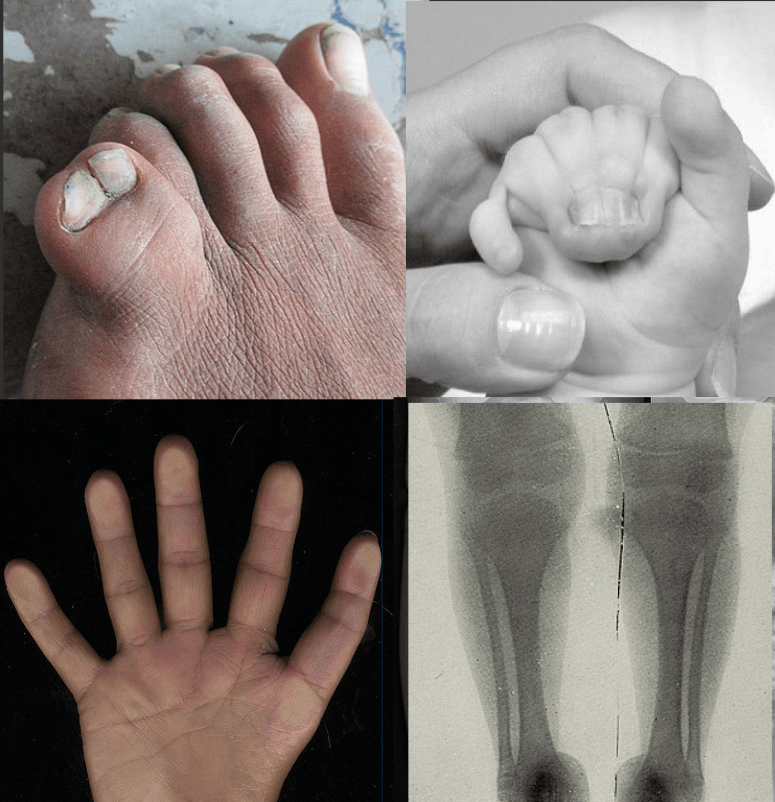
Associated findings (tibial hemimelia is rarely isolated): foot deformity (usually equinovarus), marked limb-length discrepancy, ipsilateral hand/upper-limb anomalies, bifid or duplicated femur (Gollop-Wolfgang complex), and a recognised autosomal-dominant familial form. A systematic survey for associated anomalies is mandatory.
Classification Systems
Jones Classification (1978)
Based on tibial presence and knee functionality:
- Tibial Status
- Absent tibia
- Knee Function
- Non-functional
- Treatment
- Amputation
- Tibial Status
- Proximal cartilage only
- Knee Function
- Functional (preserve)
- Treatment
- Synostosis + Syme
- Tibial Status
- Ossified proximal tibia
- Knee Function
- Functional (preserve)
- Treatment
- Synostosis + Syme
- Tibial Status
- Ossified distal only
- Knee Function
- Variable
- Treatment
- Syme or Chopart
- Tibial Status
- Short tibia, diastasis
- Knee Function
- Variable
- Treatment
- Syme amputation
Type IA: Complete absence of tibia, non-functional knee. Treatment: Amputation (knee disarticulation or above-knee). Most severe form.
Type IB: Proximal tibia present as cartilage only (not ossified on X-ray). Must differentiate from Type IA with USS/MRI. Treatment: Proximal tibiofibular synostosis + Syme amputation. Preserves knee function.
Type II: Ossified proximal tibia present. Treatment: Proximal tibiofibular synostosis + Syme amputation. Similar to Type IB but tibia is ossified.
Type III: Ossified distal tibia only (least common). Proximal tibia absent. Treatment: Syme or Chopart amputation. Assume eventual proximal ossification may occur.
Type IV: Short tibia with distal diastasis (separation). Treatment: Syme amputation.
Key point: Type IA and II are most common. Type IB vs IA differentiation is critical (requires USS/MRI).
ABCDJones Classification Types
Hook:ABCD classification: Type IA (Absent = Amputation), IB (cartilage = synostosis), II (proximal = synostosis), III/IV (distal/short = Syme)!
Clinical Assessment
- Shortened lower limb noted at birth
- May have foot deformity noted
- Family history (rare but may be present)
- Difficulty with weight-bearing or walking
- Previous treatment (if established case)
Physical Examination
- Shortened lower limb
- Assess for tibial presence (may not be palpable)
- Foot deformity (common)
- Assess for bilateral involvement
- Look for associated deformities
- Tibia may be absent or hypoplastic
- Assess fibula (usually present)
- Assess knee stability
- Assess ankle stability
- Assess foot structure
- Knee: Assess stability and function (critical)
- Ankle: May have limited motion, instability
- Assess for contractures
- True leg length: ASIS to medial malleolus
- Apparent leg length: umbilicus to medial malleolus
- Assess knee function (critical)
- Assess quadriceps function
- Assess knee stability
- Assess passive motion
- Non-functional knee (Type IA) = amputation
- Functional knee (IB/II) = synostosis possible
- Assess foot structure
- Assess for deformities
- Assess for preservation possibility
- Other limbs: Assess for other anomalies
- Other systems: Rare associations
Investigations
- Assess tibial presence/absence
- Evaluate proximal tibia (if present)
- Evaluate distal tibia (if present)
- Assess fibula (usually present)
- Measure limb length discrepancy
- Assess knee joint
- Assess ankle joint
- Accurate LLD measurement
- Assess alignment
- Evaluate knee and ankle
- Assess foot structure
- Evaluate deformities
- Essential to differentiate Type IB from IA
- Assess for proximal tibial cartilage (Type IB)
- If cartilage present = Type IB (preserve knee)
- If no cartilage = Type IA (amputation)
- Detailed assessment of proximal tibia
- Assess cartilage presence
- Differentiate Type IB from IA
Key Point: USS/MRI essential for Type IB vs IA differentiation - cannot rely on X-ray alone (cartilage not visible on X-ray).
Differential Diagnosis
The short, varus, externally deformed leg of tibial hemimelia overlaps clinically with several other congenital long-bone deficiencies. The discriminators below are high-yield.
- Key bone affected
- Tibia deficient, fibula intact
- Foot/deformity
- Equinovarus, foot supinated
- Distinguishing feature
- Varus foot, prominent fibular head laterally, extensor mechanism may be absent
- Key bone affected
- Fibula deficient, tibia present
- Foot/deformity
- Equinovalgus, lateral rays absent
- Distinguishing feature
- Valgus foot, anteromedial tibial bow, ~25x commoner than tibial
- Key bone affected
- Proximal femur
- Foot/deformity
- Foot at level of opposite knee
- Distinguishing feature
- Bulky thigh held in flexion/abduction/ER, hip instability
- Key bone affected
- Tibia present but dysplastic
- Foot/deformity
- Anterolateral tibial bow
- Distinguishing feature
- Anterolateral (not posteromedial) bow, NF1 association, fracture/nonunion
- Key bone affected
- Tibia absent + bifid femur
- Foot/deformity
- Hand ectrodactyly
- Distinguishing feature
- Distal femoral bifurcation with ipsilateral complete tibial hemimelia
Associated Syndromes: Gollop-Wolfgang Complex and Familial Forms
Tibial hemimelia is rarely isolated, and the topic repeatedly names its syndromic associations (bifid femur/Gollop-Wolfgang, hand ectrodactyly, triphalangeal thumb, familial cases) without developing them. Recognising these changes both the counselling and the reconstructive plan, because they cluster at the severe, proximally-deficient end of the spectrum.
Gollop-Wolfgang complex. The striking triad of distal femoral bifurcation (a forked/duplicated distal femur), ipsilateral complete tibial hemimelia (aplasia), and hand ectrodactyly (split-hand / "lobster-claw"); the femur-tibia overlap is sometimes labelled the tibial agenesis-ectrodactyly syndrome. The bifurcated femur carries an accessory bony spike that typically must be resected to bring the limb into line before any reconstruction or prosthetic fitting. Its presence signals that the proximal tibia is usually absent, so management gravitates toward knee disarticulation or complex staged reconstruction rather than a simple synostosis.
Familial (autosomal-dominant) tibial hemimelia. Pedigrees with affected siblings and vertical transmission are documented (Fernandez-Palazzi recorded familial cases in this topic's evidence base); an autosomal-dominant pattern with variable expressivity and incomplete penetrance is recognised, and these familial cases are more often bilateral and syndromic. A careful family history - and clinical-genetics referral where available - is therefore part of the workup.
Other named associations to survey for. Preaxial polydactyly and triphalangeal thumb (the composite radiograph in this topic is drawn from tibial hemimelia-polysyndactyly-triphalangeal-thumb syndrome), other limb-reduction defects, and occasional visceral anomalies. A deliberate head-to-toe anomaly survey is mandatory before committing to any irreversible surgical decision.
Gollop-Wolfgang = bifid (bifurcated) femur + ipsilateral complete tibial hemimelia + hand ectrodactyly. It marks the severe end of the spectrum: the proximal tibia is typically absent, the accessory femoral spike must be resected, and the knee is usually non-salvageable - so treatment tends toward disarticulation or complex staged reconstruction rather than synostosis. Always take a family history: an autosomal-dominant familial form (often bilateral/syndromic) exists.
Management Algorithm

Treatment Philosophy
Key principle: Treatment based on knee functionality, not just tibial presence.
- Knee function: Non-functional (Type IA) = amputation, functional (IB/II) = synostosis + Syme
- Tibial presence: Assess with X-ray, USS, MRI
- Type IB vs IA: Critical differentiation - USS/MRI essential
- Family preference: After counseling about both options
- Amputation: For Type IA (non-functional knee)
- Synostosis + Syme: For Type IB/II (functional knee, proximal tibia present)
- Syme or Chopart: For Type III/IV
- Amputation: 6 months to 1 year
- Synostosis: When sufficient ossification (1-2 years)
Early treatment allows prosthetic fitting and better developmental outcomes.
KNEETibial Hemimelia Treatment Decision
Hook:KNEE determines treatment: Knee functionality, No tibia (IA) = amputation, Evaluate with imaging, Early treatment timing!
Surgical Techniques
Proximal Tibiofibular Synostosis
Type IB/II (proximal tibia present, functional knee).
- Approach: Lateral approach to proximal tibia and fibula
- Preparation:
- Expose proximal tibia and fibula
- Decorticate contact surfaces
- Create bony contact
- Synostosis:
- Create bony bridge between tibia and fibula
- May use bone graft
- Internal fixation (screws, plate)
- Position: Ensure proper alignment
Cast 6-8 weeks, then protected weight-bearing. Monitor for union.
Creates stable knee joint, allows fibula to become weight-bearing bone.
Fibular Centralization (The Brown Procedure)
The Paley classification, the Paley evidence card and the Controversies section all name Brown fibular centralization as the historic reconstructive alternative to amputation for complete tibial absence, yet the Surgical Techniques section above never describes it. Because examiners ask why reconstruction of a truly absent tibia so often disappoints, this deserves its own treatment.
Concept. Brown (1965) transposed the fibula medially and centralised it beneath the femoral condyles so that it articulates with the distal femur as a "fibula pro tibia" (fibula-in-place-of-tibia) weight-bearing strut. The proximal fibula is aligned under the intercondylar notch and stabilised, soft tissues (including hamstring/knee flexors) are balanced, and the foot is managed separately - usually by Syme amputation or ankle reconstruction.
Why it disappoints in complete absence. True Jones Type IA generally means an absent or deficient quadriceps/extensor mechanism and patella. A knee with no active extension develops persistent or recurrent flexion contracture and posterior instability/subluxation of the centralised fibula, and a large proportion of these limbs ultimately require knee disarticulation anyway. This is exactly why the historic Brown procedure for complete absence gave poor knee stability.
Patient selection. The rare good candidate has active knee extension (a functioning quadriceps), a stable proximal fibula and minimal fixed flexion - but such a limb, by definition, tends to have a proximal tibial anlage (Jones IB/II) and is usually better served by tibiofibular synostosis. For genuine complete absence with no extensor mechanism, most surgeons now favour early knee disarticulation.
Modern place. Narrow. It has largely been superseded by anlage-preserving synostosis (IB/II) and by Paley-type staged reconstruction (patelloplasty, distraction of contractures, lengthening) where a proximal tibia, patella and quadriceps exist. In a viva, state this nuance explicitly rather than offering centralization as a routine option for the absent tibia.
Brown fibular centralization fails in Jones Type IA because there is no extensor mechanism (absent quadriceps/patella): the reconstructed knee cannot actively extend, so it develops recurrent flexion contracture and instability and often ends in knee disarticulation. Reserve any centralization thinking for the rare limb with active knee extension; for true complete absence with no quadriceps, early knee disarticulation remains the reliable choice.
SYNOSTOSISSynostosis Procedure
Hook:SYNOSTOSIS procedure: Stable knee, Young age, Non-weight bearing, Ossification required, Syme amputation, Tibiofibular fusion, Outcomes good, Stable joint, Imaging essential, Surgical technique!
Complications
Synostosis Complications
- Infection (rare)
- Wound healing problems
- Neurovascular injury (rare)
- Nonunion (may need revision)
- Malalignment
- Knee instability (if synostosis fails)
- Hardware problems
- Wound healing problems (5-10%)
- Infection (rare)
- Heel pad migration (Syme, if not properly fixed)
- Heel pad migration (may need revision)
- Bony overgrowth (may need revision)
- Prosthetic fitting problems (rare)
- Careful patient selection
- Meticulous surgical technique
- Proper imaging (USS/MRI for IB vs IA)
- Realistic expectations
Postoperative Care
Synostosis
- Pain management
- Wound care
- Cast 6-8 weeks
- Protected weight-bearing
- Physical therapy
- Prepare for Syme amputation
- Prosthetic fitting
- Gait training
- Return to activities
Amputation (Type IA)
- Pain management
- Wound care
- Cast 2-3 weeks
- Prosthetic fitting (6-8 weeks)
- Gait training
- Return to activities
- Prosthetic adjustments as child grows
- Monitor for complications
- Regular follow-up
Outcomes and Prognosis
- Good function with prosthesis
- Single surgery
- Early treatment allows development
- Minimal restrictions
- Preserves knee function
- Good prosthetic function
- Two-stage procedure
- Better than amputation if knee functional
- Variable outcomes
- Depends on specific anatomy
- Both groups function well overall
- Prosthetic function good
- Psychosocial support important
- Appropriate patient selection
- Proper imaging (IB vs IA differentiation)
- Meticulous surgical technique
- Early treatment
- Prosthetic adjustments as child grows
- Most function independently
- Regular follow-up needed
Guidelines, Registries & Global Practice
Global epidemiology
- Incidence approximately 1 per 1,000,000 live births - one of the rarest long-bone deficiencies, roughly 25-30x less common than fibular hemimelia.
- Slight male predominance; bilateral in around 30%; right and left affected equally.
- Rarely isolated - associated limb (hand ectrodactyly, bifid femur/Gollop-Wolfgang), and occasional syndromic or autosomal-dominant familial forms; a deliberate anomaly survey is mandatory.
Practice positions across regions (no single society publishes a dedicated tibial hemimelia guideline given rarity; positions are derived from major paediatric limb-deficiency literature):
- Position on first-line treatment
- Early amputation - knee disarticulation for type 1a, Syme for distal types
- Emphasis
- Reliable single-stage prosthetic rehabilitation
- Position on first-line treatment
- Stage with US/MRI first; preserve the cartilaginous anlage where present
- Emphasis
- Pathoanatomy-driven, anlage-preserving
- Position on first-line treatment
- Joint-preserving reconstruction when proximal tibia, patella and quadriceps present
- Emphasis
- Brown centralization, patelloplasty, Ilizarov lengthening
- Position on first-line treatment
- Early amputation and locally fabricated prosthesis
- Emphasis
- Cost, durability, single definitive procedure
Registry note: congenital limb-deficiency surveillance networks (e.g. EUROCAT in Europe, ICBDSR internationally) capture birth-prevalence data, but no arthroplasty-style implant registry exists for this reconstructive paediatric condition - outcome evidence rests on single-centre case series (level IV), not registry or randomised data.
High- vs limited-resource practice variation
- High-resource: MRI/ultrasound staging, multidisciplinary teams (paediatric orthopaedics, radiology, prosthetics, physiotherapy, psychology, genetics), and the option of multi-stage reconstruction with growth-friendly lengthening.
- Limited-resource: imaging access may be confined to plain radiographs, biasing toward early amputation; prosthetic durability, follow-up logistics and cost favour a single definitive procedure.
Counselling and governance (universal): informed consent for an irreversible decision (amputation vs reconstruction), documented knee/quadriceps assessment, US/MRI confirmation of the anlage before committing, balanced discussion of both pathways with realistic outcome expectations, and structured follow-up to skeletal maturity for limb-length management and prosthetic adjustment.
Controversies and Areas of Uncertainty
The historic default of early amputation (knee disarticulation for type 1a, Syme for distal types) is reliable, single-stage and gives excellent prosthetic function. Modern reconstruction (fibular centralization, patelloplasty, lengthening) can preserve a biological knee and foot, and Shahcheraghi reported better quality-of-life scores in reconstructed limbs - but at the cost of multiple operations and higher complication rates. There is no level 1 evidence; the decision is individualised.
Whether a radiographically absent proximal tibia is truly absent (Jones 1a) or merely cartilaginous (Jones 1b / Weber) cannot be settled by plain film. Ultrasound and MRI are decisive, yet access varies worldwide. Mislabelling a salvageable knee as 1a and amputating is the central pitfall.
Fibular centralization (the Brown procedure) for complete tibial absence has historically given disappointing knee stability, with high rates of persistent flexion contracture. Its modern indication is narrow - many surgeons still prefer knee disarticulation when no proximal tibia or quadriceps exists.
Jones remains the exam standard but is purely radiographic; Kalamchi is treatment-oriented; Weber adds the anlage and a whole-limb score; Paley is reconstruction-focused. None is universally adopted, so always state which system you are quoting.
MCQ Practice Points
Q: What is the key difference between Jones Type IA and Type IB tibial hemimelia? A: Type IA has complete absence of tibia (no cartilage or bone) with non-functional knee, requiring amputation. Type IB has proximal tibial cartilage present (not visible on X-ray, requires USS/MRI) with functional knee, allowing synostosis + Syme amputation. The differentiation is critical and requires imaging beyond X-ray.
Q: What is the most important factor in determining treatment for tibial hemimelia? A: Knee functionality - non-functional knee (Type IA) = amputation, functional knee (Type IB/II) = proximal tibiofibular synostosis + Syme amputation. The presence of proximal tibia (even as cartilage) allows knee preservation, while complete absence requires amputation.
Q: Why is USS or MRI essential for Type IB tibial hemimelia? A: Proximal tibial cartilage is not visible on X-ray - Type IB has cartilage present that allows knee preservation, but this cannot be seen on radiographs. USS/MRI is essential to differentiate Type IB (cartilage present, preserve knee) from Type IA (no tibia, amputation). Clinical exam and X-ray alone are insufficient.
Q: What is the purpose of proximal tibiofibular synostosis in tibial hemimelia? A: Creates stable knee joint when proximal tibia present (Type IB/II) - the synostosis fuses the proximal tibia to the fibula, allowing the fibula to become the weight-bearing bone and preserving knee function. This is followed by Syme amputation distally to create an end weight-bearing stump.
Q: What is the recommended timing for amputation in Type IA tibial hemimelia? A: 6 months to 1 year of age - early amputation allows prosthetic fitting and normal development. For Type IB/II synostosis, the procedure is performed at 1-2 years when sufficient ossification is present. Early treatment improves outcomes.
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 3-month-old infant presents with tibial hemimelia. On examination, the tibia appears absent on X-ray, but there is some knee function. How would you assess and manage this child?”
“A 2-year-old child with confirmed Type IB tibial hemimelia (proximal tibial cartilage present, functional knee) is ready for synostosis. Describe the procedure and postoperative management.”
“A 6-month-old infant with Type IA tibial hemimelia (confirmed absent tibia, non-functional knee) is ready for treatment. The parents are asking about treatment options. How would you counsel them and what procedure would you recommend?”
Key Facts
- Incidence: 1 in 1,000,000 (very rare, much rarer than fibular hemimelia)
- Jones classification: Type IA-IV based on tibial presence and knee function
- Key decision: Knee functionality - non-functional (IA) = amputation, functional (IB/II) = synostosis
- Type IA and II are most common
Jones Classification
- Type IA: Absent tibia, non-functional knee = Amputation
- Type IB: Proximal cartilage only (differentiate with USS/MRI) = Synostosis + Syme
- Type II: Ossified proximal tibia = Synostosis + Syme (like IB)
- Type III: Ossified distal only (rare) = Syme or Chopart
- Type IV: Short tibia, distal diastasis = Syme amputation
Treatment Decision
- Type IA: Knee disarticulation or above-knee amputation (6m-1y)
- Type IB/II: Proximal tibiofibular synostosis (1-2y) + Syme amputation
- Key: Knee functionality determines treatment
- USS/MRI essential for IB vs IA differentiation (cartilage not visible on X-ray)
Surgical Pearls
- Synostosis: Decorticate surfaces, create bony bridge, internal fixation
- Preserves knee function when proximal tibia present
- Fibula becomes weight-bearing bone after synostosis
- Syme amputation performed distally after synostosis heals
Complications
- Synostosis: Nonunion (may need revision), malalignment, knee instability
- Amputation: Wound healing (5-10%), heel pad migration (Syme)
- Prevention: Careful patient selection, proper imaging, meticulous technique
- Realistic expectations essential
Evidence Base
Jones Classification of Tibial Aplasia/Dysplasia
- Original radiographic classification of congenital tibial deficiency with intact fibula
- Type 1a: tibia not visualised, hypoplastic distal femoral epiphysis; Type 1b: tibia not seen but proximal anlage present
- Type 2: proximal tibia ossified, distal tibia absent; Type 3: distal tibia present, proximal absent (rare); Type 4: distal tibiofibular diastasis
- Quadriceps/knee function and proximal tibial presence drive whether the knee can be salvaged
Kalamchi Classification of Congenital Tibial Deficiency
- Late results of 24 legs in 21 children with a proposed treatment-oriented classification
- Type I: total tibial absence; Type II: distal absence; Type III: distal deficiency with tibiofibular diastasis
- Early radiographic appearance, quadriceps function and severity of knee flexion contracture guided operation selection
- Classification correlated with both treatment recommendation and final functional result
Weber Classification and Score: Role of the Cartilaginous Anlage
- Seven-type classification with a five-class score evaluated on 95 affected limbs
- Explicitly incorporates the cartilaginous tibial anlage, under-recognised in earlier systems
- Requires sonography and MRI for precise pre-operative pathoanatomy beyond plain radiographs
- Type VII (61%) and type III (15%) were the most frequent patterns in the series
Paley Classification and Reconstructive Options
- New classification linking pathoanatomy to reconstruction rather than defaulting to amputation
- Describes Brown fibular centralization, Weber patelloplasty and staged distraction techniques
- Improved understanding of genetics, aetiology and pathoanatomy underpins joint-preserving surgery
- Presence of a knee joint, patella and quadriceps mechanism favours reconstruction
Functional Outcomes of Reconstruction with Foot Preservation
- 36 patients (48 tibial-deficient limbs), mean follow-up 9 years - largest single-surgeon series
- Primary amputation in 8 patients (10 limbs); limb preservation in 38 legs (28 patients)
- Tibiofibular synostosis, ankle centralization and Ilizarov lengthening were the commonest procedures
- Reconstructed group PedsQL (68) exceeded the amputation group; nonunion of synostosis (2) and knee stiffness (6) were the main complications
Epidemiology and Type Distribution
- 22 limbs in 18 patients confirm incidence of approximately 1 per 1 million live births
- Frequently associated with other anomalies of the same limb or elsewhere; familial cases recorded
- Jones type distribution: 9 type Ia, 4 type Ib, 3 type II, 2 type III, 4 type IV
- Earlier amputation gave faster rehabilitation; the child accepts it as a congenital amputation
Deformity Reconstruction Surgery for Tibial Hemimelia
- Comprehensive contemporary review of pathology, classification and surgical options
- Type-specific reconstruction: staged distraction of knee/ankle contractures, Weber patelloplasty, fibular centralization, arthrodesis
- Amputation remains simpler and reliable, but reconstruction increasingly delivers good function
- Factors favouring reconstruction: present knee joint/proximal tibia and an intact patella with quadriceps mechanism