Diagnosis of Exclusion
- Diagnosis of Exclusion: You MUST rule out CP, Duchenne's, and Autism/Sensory processing issues.
- Key Exam Finding: Normal neurological exam (no clonus, normal reflexes, normal tone).
- Gowers Sign: Check for proximal myopathy (Duchenne).
- Spasticity: Check for catch (tardieu scale) to rule out CP.
- Management: Stretching to Casting to Surgery (TAL/Gastrocs).
- “Ask about birth history (prematurity = CP risk)
- “Ask about 'late walker' (Duchenne)
- “Can they stand flat on command? (Differentiates habit from fixed contracture)
- “Check localized back skin changes (hair tuft = tethered cord)
Do not diagnose 'Idiopathic' without checking:
- CK Level: Rule out Duchenne Muscular Dystrophy in all males.
- Spine MRI: Rule out Tethered Cord/Diastematomyelia if any neuro signs.
- Clonus: Greater than 3 beats is abnormal. Suggests Upper Motor Neuron lesion (CP).
- Mild Cerebral Palsy
- Often Premature / NICU
- Idiopathic Toe Walking
- Usually Normal Term
- Mild Cerebral Palsy
- Spastic (Clasp-Knife)
- Idiopathic Toe Walking
- Normal (or only tightness)
- Mild Cerebral Palsy
- Hyperreflexic / Clonus
- Idiopathic Toe Walking
- Normal
- Mild Cerebral Palsy
- Crouch / Scissoring / Intoeing
- Idiopathic Toe Walking
- Pure Equinus (Bouncing)
- Mild Cerebral Palsy
- Difficult
- Idiopathic Toe Walking
- Often can do on command (early)
PPPHistory Red Flags
Hook:The 3 P's.
Overview/Epidemiology
Idiopathic Toe Walking (ITW) is a condition where children walk on their toes (forefoot contact) without any identifiable neurological or orthopedic cause.
- Early Walkers: New walkers often toe-walk intermittently for the first 3-6 months. This is normal.
- Resolution: Most ITW resolves spontaneously.
- Persistence: If it persists beyond age 3, it is considered pathological/habitual.
- Sequelae: Long-term toe walking leads to adaptive shortening of the Achilles tendon (equinus contracture), widening of the forefoot (splay foot), and rarely traumatic symptoms in adolescence.
- Speech Delay/Autism: High prevalence of toe walking in children with ASD (Sensory processing).
- ADHD: Also associated.
Etiology Theories
Several theories attempt to explain idiopathic toe walking:
Neurological Hypothesis:
- Incomplete maturation of central pattern generators
- Abnormal supraspinal control of gait
- Vestibular dysfunction affecting postural control
- Sensory processing abnormalities
Musculoskeletal Hypothesis:
- Primary shortening of gastrocnemius-soleus complex
- Altered muscle fiber composition (increased Type I fibers)
- Developmental variation in tendon length
- Habitual pattern leading to adaptive shortening
Genetic Factors:
- Strong familial clustering (30-70% have positive family history)
- Autosomal dominant inheritance pattern suggested
- May represent a phenotypic spectrum with variable penetrance
True Idiopathic Toe Walking vs 'Short Tendo Achilles'
The natural-history evidence and the controversies section both rely on a modern distinction the body never develops: the child with an early fixed ankle contracture is not a true idiopathic toe-walker but has a separate entity - "short tendo Achilles". This reconceptualisation (Engström & Tedroff, JBJS Am 2018) overturns the old habit of labelling every toe-walker "idiopathic" and changes what you do.
The key observation: in the population cohort, true idiopathic toe walking did NOT cause a triceps surae contracture - around 79% resolved spontaneously by age 10 with preserved passive dorsiflexion. The small group who carried a fixed equinus from the start behaved differently and should be diagnosed separately as a (often congenital) short tendo Achilles, because they do not self-resolve and benefit from earlier active treatment.
- True idiopathic toe walking
- Intermittent, can often stand/walk flat on command
- Short tendo Achilles
- Persistent; cannot reach the floor flat
- True idiopathic toe walking
- Preserved (no fixed contracture)
- Short tendo Achilles
- Fixed equinus from early on (cannot reach neutral)
- True idiopathic toe walking
- ~79% resolve spontaneously by age 10, no contracture
- Short tendo Achilles
- Does NOT self-resolve; contracture persists/worsens
- True idiopathic toe walking
- Reassurance and observation appropriate
- Short tendo Achilles
- Treat early (casting/surgery); do not just reassure
Why it matters for the exam and the clinic: the presence of a fixed contracture (passive dorsiflexion that cannot reach neutral) in a persistent toe-walker should make you doubt the "idiopathic" label - both because it may be a non-idiopathic cause (CP, neuromuscular disease, tethered cord) and because, even if neurology is normal, it is better classified as short tendo Achilles and treated rather than watched. The corollary is reassuring: a flexible toe-walker who can get flat has true ITW and a high chance of spontaneous resolution. (This is the modern nuance behind the older teaching that ITW is "a diagnosis of exclusion"; the distinction is still debated - see Controversies.)
True idiopathic toe walking does not cause a fixed contracture and mostly resolves by age 10 - so a persistent toe-walker who already has a fixed equinus (cannot reach neutral) is either non-idiopathic or a separate "short tendo Achilles", and is treated early rather than simply observed. Reserve "idiopathic" for the flexible, intermittently toe-walking child who can get flat.
TOESDifferential Diagnosis of Toe Walking
Hook:Check the TOES.
Pathophysiology, Anatomy & Pathomechanics
- Gastrocnemius: Crosses the knee and ankle. Tightness is tested with the knee extended.
- Soleus: Crosses only the ankle. Tightness is tested with the knee flexed.
- Silfverskiold Test: Essential to differentiate gastroc vs soleus tightness.
- Gastroc Tightness: Ankle dorsiflexion improves when knee is flexed. (Most common in ITW).
- Soleus/Combined: Ankle dorsiflexion remains limited even when knee is flexed.
- Initial Contact: Forefoot strike instead of heel strike.
- Mid-stance: "Vaulting" over the stiff ankle.
- Push-off: Often powerful, "bouncing" gait.
- Compensations: Anterior pelvic tilt, lumbar lordosis (sway back) to shift center of gravity forward.
- Histological studies of calf muscle in ITW show a specific pattern: Increased Type I (slow twitch) fibers, suggesting a chronic adaptation to sustained activity rather than a primary myopathy.
Classification Systems
Alvarez Classification
Designed to guide treatment based on severity of contracture.
- Mild: No fixed contracture. Can stand flat on command. Dynamic deformity only.
- Moderate: Transient contracture. Can be passively corrected but walks on toes.
- Severe: Fixed equinus contracture. Cannot reach neutral dorsiflexion even passively.
Clinical Assessment
- Birth: Prematurity? NICU stay? (CP).
- Milestones: Did they walk late? (Duchenne/Myopathy).
- Family Hx: Do dad/mum walk on toes?
- Pattern: Intermittent or Constant? Worse when tired?
- Pain: Is there pain? (Pain usually points to a tarsal coalition or infection/tumor, not ITW).
- Gait: Observe walking and running. Ask them to "walk like a penguin" (heels only) and "walk like a giant" (toes).
- Neurological:
- Reflexes (Patella/Achilles).
- Clonus (Rapid rhythmic beating).
- Tone (Catch?).
- Gowers Sign (Ask child to stand up from floor - do they walk hands up thighs?).
- Orthopedic:
- Silfverskiold Test: Check DF with knee straight vs bent.
- Popliteal Angle: Check hamstring tightness (often associated).
- Spine: Check for hairy patch/dimple (Spina bifida occulta).
Investigations
- CK (Creatine Kinase): Mandatory in all males with idiopathic toe walking to rule out Duchenne Muscular Dystrophy.
- Genetic Testing: If suspicious features.
- X-rays (Lateral Stand):
- Look for "talar beaking" (chronic impingement).
- Look for Tarsal Coalition (C-sign).
- Spine MRI:
- Indication: If any neurological signs (asymmetry, atrophy, reflex change, bladder issues).
- Rule out: Tethered cord, syrinx, diastematomyelia.
Gait Analysis:
- Shows "double bump" absent pattern.
- Premature calf activation.
- Used in research, rarely essential for straightforward clinical cases.
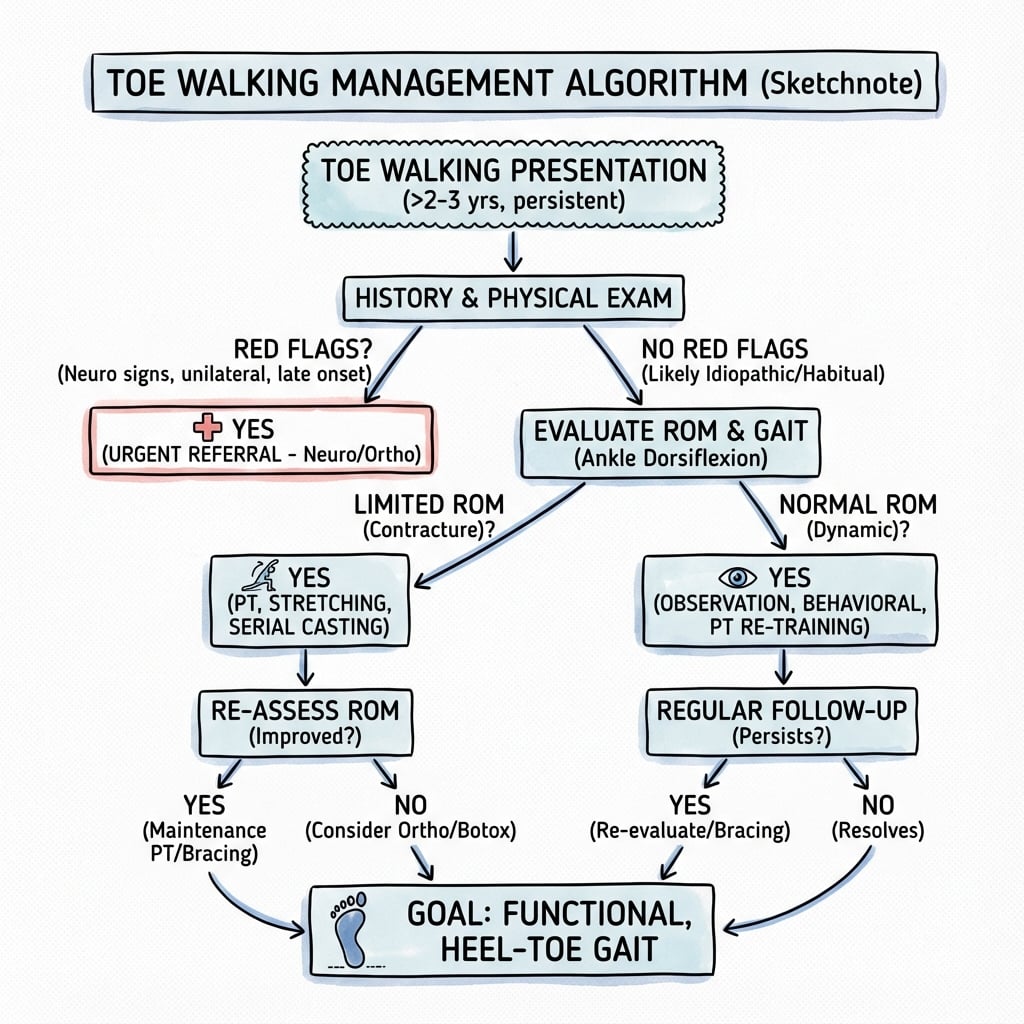
Management Algorithm
1. Observation
- Age less than 3 years.
- No contracture.
- Reassurance (Most resolve).
2. Physical Therapy
- Stretching (Calf stretches).
- Tibialis Anterior strengthening.
- Motor planning games (walking on heels).
3. Serial Casting (The Gold Standard)
- Indication: Fixed contracture (less than 0 deg dorsiflexion).
- Protocol: Below knee walking casts changed weekly for 6 weeks.
- Goal: Plastic deformation of the sarcomeres (add sarcomeres in series).
- Success: High short term success, but recurrence is common.
4. Botox
- Role: Paralyzes the gastrocnemius temporarily to allow easier stretching/casting.
- Evidence: controversial. Some studies show adding Botox to Casting is better than Casting alone.
SSSManagement Hierarchy
Hook:Start with S.
How Serial Casting Lengthens Muscle and Why It Recurs
The management section states that casting works by "plastic deformation of the sarcomeres (add sarcomeres in series)", the FAQ says it is a "low load, long duration stretch that remodels the tissue", and the post-operative section notes recurrence happens because "bone elongates faster than muscle-tendon" - but the biology that ties these together is never assembled. It explains why casting beats manual stretching and why ITW is so prone to recur during growth.
Why a cast lengthens muscle when manual stretching does not:
- Manual/quick stretch
- High load, short duration
- Serial cast (sustained)
- Low load, long duration
- Manual/quick stretch
- Elastic - springs back to length
- Serial cast (sustained)
- Viscoelastic creep + biological remodelling
- Manual/quick stretch
- None lasting
- Serial cast (sustained)
- Adds sarcomeres in series (true lengthening of the muscle belly)
- Manual/quick stretch
- Transient
- Serial cast (sustained)
- Genuine, retained gain in dorsiflexion
A muscle held at a sustained stretch responds by serial sarcomerogenesis - laying down new sarcomeres in series along each myofibril, genuinely lengthening the muscle belly - while the tendon undergoes viscoelastic stress-relaxation/creep. A brief manual stretch only deforms the tissue elastically, so it recoils; the cast's "low-load, long-duration" hold is what triggers the remodelling. This is why casting, not stretching, is the conservative workhorse for a true contracture.
Why recurrence is the rule, not the exception: longitudinal muscle growth normally keeps pace with bone by adding sarcomeres at the myotendinous junction, driven by the stretch the growing bone applies. In a toe-walker the muscle-tendon unit fails to keep pace with the bone lengthening at the physis, so every growth spurt re-shortens the construct and the equinus returns. Recurrence therefore reflects the biology of a growing child rather than a failed technique - which is exactly why night splinting must continue through growth, why correction in a skeletally immature child is inherently fragile, and why rapid or repeated recurrence should prompt a re-screen for a missed driver (tethered cord, evolving CP).
A cast lengthens muscle by a low-load, long-duration stretch that adds sarcomeres in series (true muscle-belly lengthening) plus tendon creep - a quick manual stretch is only elastic and recoils, which is why casting works and stretching alone does not. Recurrence is common because the muscle-tendon unit cannot keep pace with bone growth at the physis, so each growth spurt re-shortens it - hence night splinting through growth and re-casting early recurrence.
Surgical Technique: Zone 1 vs Zone 3

Gastrocnemius Recession (Strayer)
Indication: Isolated Gastroc Tightness. Technique:
- Incision: Posterior medial calf, just distal to muscle belly.
- Identify: Sural nerve (lateral).
- Dissect: Separate Gastrocnemius tendon form underlying Soleus muscle fascia.
- Cut: Transverse division of the Gastrocnemius tendon.
- Test: Push foot into dorsiflexion. You will see the cut ends separate (usually 2cm gap).
- Repair: Suture skin only. Pros: Maintains soleus power (push off strength). Low risk of over-lengthening.
Complications
- Rate
- High (20-30%)
- Prevention/Management
- Continuing night splints and stretching post-op.
- Rate
- Rare (TAL)
- Prevention/Management
- Avoid TAL if possible. Do Strayer. Aim for neutral, not 10 deg DF.
- Rate
- Severe
- Prevention/Management
- Result of over-lengthening. Use AFOs. Hard to fix.
- Rate
- Rare
- Prevention/Management
- Sural nerve at risk in lateral release.
- Rate
- greater than 1%
- Prevention/Management
- Standard protocol.
Key principles: recurrence is managed by escalating back up the ladder (re-stretch to re-cast to revision surgery) and prompts a search for a missed driver (tethered cord, evolving CP) if it is rapid or repeated. Calcaneal gait from over-lengthening is largely preventable by never lengthening past neutral; once established it is very difficult to reverse and is supported with an AFO and gastrocnemius strengthening. Post-TAL weakness affects push-off and usually compensates over 6-12 months but may limit elite sprint/jump performance — a further reason to prefer Strayer.
Postoperative Care
- Timing
- Weeks 0-4
- Focus
- Below-knee walking cast/CAM boot in neutral dorsiflexion (slight plantarflexion if repair tension is high); weight-bear as tolerated.
- Timing
- Weeks 4-8
- Focus
- Transition to AFO/night splint; begin active dorsiflexion and proprioceptive work; pool therapy if available.
- Timing
- Weeks 8-12
- Focus
- Progressive tibialis anterior and eccentric calf strengthening; single-leg balance; cycling.
- Timing
- Weeks 12+
- Focus
- Walk-jog progression then jump/hop drills; full sport once power normalises.
Night splints are critical. Evidence supports night splinting through the first 12 months to prevent recurrence, because during growth bone elongates faster than muscle-tendon and re-shortens the construct.
Outcomes/Prognosis
- Natural history: most ITW resolves spontaneously — around 79% by age 10 in population data (Engström & Tedroff, JBJS Am 2018), without contracture.
- Recurrence: ITW is notorious for recurrence, especially during growth spurts; night splinting mitigates this.
- Surgical durability: functional gait gains after lengthening are maintained at 5 years (McMulkin, Gait Posture 2016).
- Adult sequelae: limited data; most function well, occasionally with calf tightness or forefoot symptoms.
- Worse prognosis
- Older at presentation (over 7 years)
- Worse prognosis
- Severe fixed equinus (over 15 degrees)
- Worse prognosis
- Associated ASD or sensory-processing disorder
- Worse prognosis
- Multiple failed casting attempts; poor splint compliance
- Worse prognosis
- Rapid or repeated recurrence (re-screen for tethered cord/CP)
Follow-up: after casting, review at 6 weeks, 3, 6 and 12 months measuring dorsiflexion, continuing night splints for 6-12 months and re-casting early recurrence. After surgery: 2-week wound check, 6-week immobilisation removal and physio, 3-month gait/strength review, 6-month sport clearance, then annual review to skeletal maturity.
Guidelines, Registries & Global Practice
Global epidemiology:
- Prevalence approximately 2-5% in the general paediatric population; the best population data (Swedish cohort, n=1,401) give approximately 5% at age 5.5 years (Engström & Tedroff, JBJS Am 2018).
- Around 79% resolve spontaneously by age 10 without treatment or contracture.
- Family history positive in roughly 30-70% of series; slight male predominance.
- Toe walking is far more common in autism spectrum disorder (approximately 20% in one large series) and in language/developmental disorders.
Side-by-side guidance (no single national society "owns" ITW — practice is consensus-driven):
- Position on Toe Walking
- Observe children under 3-5 years with no contracture; most resolve.
- Position on Toe Walking
- Confirm diagnosis of exclusion first (rule out CP, neuromuscular disease, tethered cord); stretching and serial casting before surgery.
- Position on Toe Walking
- Serial casting and surgery improve dorsiflexion and gait; botulinum toxin A adds no benefit to casting.
- Position on Toe Walking
- Any boy with toe walking plus calf hypertrophy, late walking or proximal weakness needs a CK before an "idiopathic" label.
there is no dedicated ITW registry. ITW is a benign, self-limiting condition not tracked in arthroplasty/implant registries; outcome evidence comes from single-centre series and gait-analysis cohorts rather than national registries.
- Well-resourced centres: access to 3D instrumented gait analysis, formal serial-casting clinics, occupational therapy for sensory-driven toe walking, and selective surgery (Strayer/gastrocnemius recession preferred).
- Limited-resource settings: diagnosis is clinical; CK and spine MRI may be hard to obtain, so a careful neurological exam carries more weight. Home stretching and below-knee casting are low-cost and effective; surgery is reserved for fixed contractures that fail conservative care.
- A common global pitfall is late referral — toe walking dismissed as "they will grow out of it" until a fixed equinus contracture has developed.
Controversies & Areas of Uncertainty
- Is ITW a distinct entity or a spectrum? The 2018 natural-history cohort argues that children with early fixed contracture are a separate "short tendo Achilles" group, not true ITW — challenging the older habit of labelling all toe-walkers as idiopathic.
- Role of botulinum toxin. Despite widespread use, the best RCT (Engström 2013) and systematic review (van Kuijk 2014) show botulinum toxin A adds nothing to casting. Some centres still use it to ease casting; the evidence does not support routine use.
- When (and whether) to intervene at all. Because approximately 79% resolve spontaneously, the threshold for casting versus observation in a flexible foot is genuinely uncertain; over-treatment of a self-limiting condition is a real risk.
- Surgery: Strayer vs TAL vs intramuscular lengthening. Strayer/gastrocnemius recession is favoured for isolated gastrocnemius tightness to preserve push-off power, but high-level comparative data are lacking; choice is guided by the Silfverskiöld test and surgeon preference.
- Sensory drive in ASD. In autism/sensory-processing toe walking, mechanical correction may fail if the sensory drive persists; the place of occupational/sensory therapy versus orthopaedic treatment is not standardised.
- Cause unknown. No single neurological or musculoskeletal mechanism has been proven; the strong familial clustering suggests a heritable component without a defined gene.
Deep Dive: Sensory Processing
Why do they do it? In children with ASD or Sensory Processing Disorder, toe walking is theorized to be:
- Seekers: Seeking intense proprioceptive input through the calf muscles.
- Avoiders: Avoiding tactile sensation of the floor on their heels/soles.
- Vestibular: Altering head position in space. Implication: Mechanical treatment alone (casting/surgery) may fail if the sensory drive remains. Occupational Therapy is key.
Parent's Guide: Frequently Asked Questions
Q: Will he grow out of it? A: If he is under 3, possibly. If he is 7 and has tight heels, no. He needs help (stretches or casting).
Q: Is surgery dangerous? A: It is low risk, but "over-lengthening" is a disaster where the child walks flat but has no power to run or jump. We are very conservative to avoid this.
Q: Why do we have to cast? Can't we just stretch? A: Once the tendon is physically short (contracture), manual stretching is like trying to stretch a leather belt. It doesn't work well. Casting provides a "low load, long duration" stretch that actually remodels the tissue.
Q: Does Botox cure it? A: No. Botox just relaxes the muscle temporarily. We use it to make the casting easier and more effective, but the casting does the work.
Q: What about AFOs (ankle braces)? A: AFOs can help maintain correction after casting or surgery, and are useful as night splints to prevent recurrence. They don't actively stretch the tendon but prevent it from shortening again. Solid AFOs are best for contracture prevention.
Q: Can toe walking cause back pain? A: Chronic toe walking can cause compensatory lumbar lordosis (swayback) to shift the centre of gravity forward. This may contribute to back pain in some cases, though studies haven't shown a strong long-term association.
Q: My child was diagnosed with autism. Will the toe walking treatment still work? A: Treatment outcomes are somewhat less predictable in children with autism spectrum disorder. The mechanical treatment (casting/surgery) can still work for the contracture, but the sensory-seeking behaviour may persist. Occupational therapy addressing sensory processing is an important part of management.
Case Study: The Late Presenter
9-year-old male. History: Tioe walker since age 2. "Physio didn't work". Exam:
- Fixed equinus: -20 degrees dorsiflexion with knee straight. -10 degrees with knee bent.
- Neuro: Normal. CK: Normal.
- Gait: Bouncing, early heel rise.
- Attempted Serial Casting x 6 weeks. Improved to neutral, but recurred within 3 months.
- Surgery: Zone 1 Gastrocnemius Recession (Strayer).
- Intra-op: 2.5cm gap obtained in muscle belly. Dorsiflexion improved to +15 degrees.
- Post-op: Walking boot 4 weeks. Night splints 6 months.
- Outcome: Walks flat. Plays soccer. No recurrence at 2 years.
Key Learning Points from Case
- Serial casting should be attempted first even in older children with fixed contractures
- Zone 1 (Strayer) is preferred when gastrocnemius is the primary problem (positive Silfverskiold)
- Post-operative splinting is crucial - minimum 6 months to prevent recurrence
- Complete neurological workup (CK, neuro exam) must precede any surgical intervention
- Realistic expectations - improvement takes time and compliance is essential
Additional Case Scenarios
Case 2: The Toddler
- 2.5-year-old female, intermittent toe walking noticed by parents
- Can stand flat on command, no contracture
- Normal neurological examination
- Management: Reassurance, observation, reassess at age 3-4 if persists
Case 3: The Duchenne Suspect
- 4-year-old male with toe walking, difficulty climbing stairs
- Positive Gowers sign, enlarged calves
- CK level: 15,000 U/L (normal less than 200)
- Management: Urgent referral to paediatric neurologist, genetic testing, NOT orthopaedic surgery
MCQ Practice Points
Q: Which feature is consistent with Idiopathic Toe Walking? A: Normal Reflexes. Hyperreflexia suggests CP. Absent reflexes suggests neuropathy/myopathy.
Q: What is the primary advantage of a Strayer procedure over a TAL? A: Preservation of Push-off Power. The soleus is left intact to generate force.
Q: What neuro-developmental disorder is most strongly associated with toe walking? A: Autism Spectrum Disorder (ASD).
Q: A positive Silfverskiold test implies tightness of which muscle? A: Gastrocnemius. (Improved DF with knee flexion).
Self-Assessment Quiz
2. Describe a positive Gowers sign.
The child uses their hands to 'climb up' their legs when standing from a floor sitting position. Indicates proximal muscle weakness.
Viva Scenarios
Practise clinical reasoning and management decisions out loud
“4-year-old boy. Parents concerned he walks on toes. Constant. No pain.”
“7-year-old girl. Casted twice. Recurved. Now has -15 deg dorsiflexion.”
“Child toes walk, but when standing flat, they have a severe flat foot.”
RULE OUT
- Cerebral Palsy (Spasticity)
- Duchenne (CK)
- Tethered Cord (Spine MRI)
- Autism (Sensory)
- Habitual Toe Walking
CLINICAL
- Normal Neuro Exam
- Bouncing Gait
- Positive Silfverskiold
- Family Hx
CLASSIFICATION
- Alvarez Type 1 (Mild/Dynamic)
- Alvarez Type 2 (Moderate)
- Alvarez Type 3 (Fixed greater than 20 deg)
- Pompeo Type 1 (Gastroc)
- Pompeo Type 2 (Combined)
MANAGEMENT
- Stretch/Physio
- Serial Cast (Gold Stal)
- Strayer (Zone 1)
- TAL (Zone 3)
Evidence Base
- Population-based cohort of 1,401 Swedish children; ITW prevalence approximately 5% (63 of 1,401) at age 5.5 years
- By age 10, 79% (50 of 63) had spontaneously developed a typical gait without intervention
- Idiopathic toe walking did NOT cause triceps surae contracture; a separate subgroup with early ankle contracture is 'short tendo Achilles', not ITW
- Neurodevelopmental comorbidity was common among persistent toe-walkers
- Review of 954 ambulatory children seen by a developmental paediatrician
- Persistent toe walking occurred in 20.1% of 324 children with autism spectrum disorder
- Tight heel cords occurred in 12.0% of ASD children
- Confirms a high incidence of toe walking and secondary contracture risk in autism and language disorders