Article summary
A comprehensive review of Dual Mobility (DM) in Total Hip Arthroplasty. Understanding the 'Jump Distance', indications for use, and the unique complication of Intra-Prosthetic Dislocation.
Educational content is reviewed for source visibility, editorial coherence, and correction readiness.
No individual clinician credential is claimed unless a named person is shown.
Verify before clinical use; this is not medical advice or a substitute for local guidance.
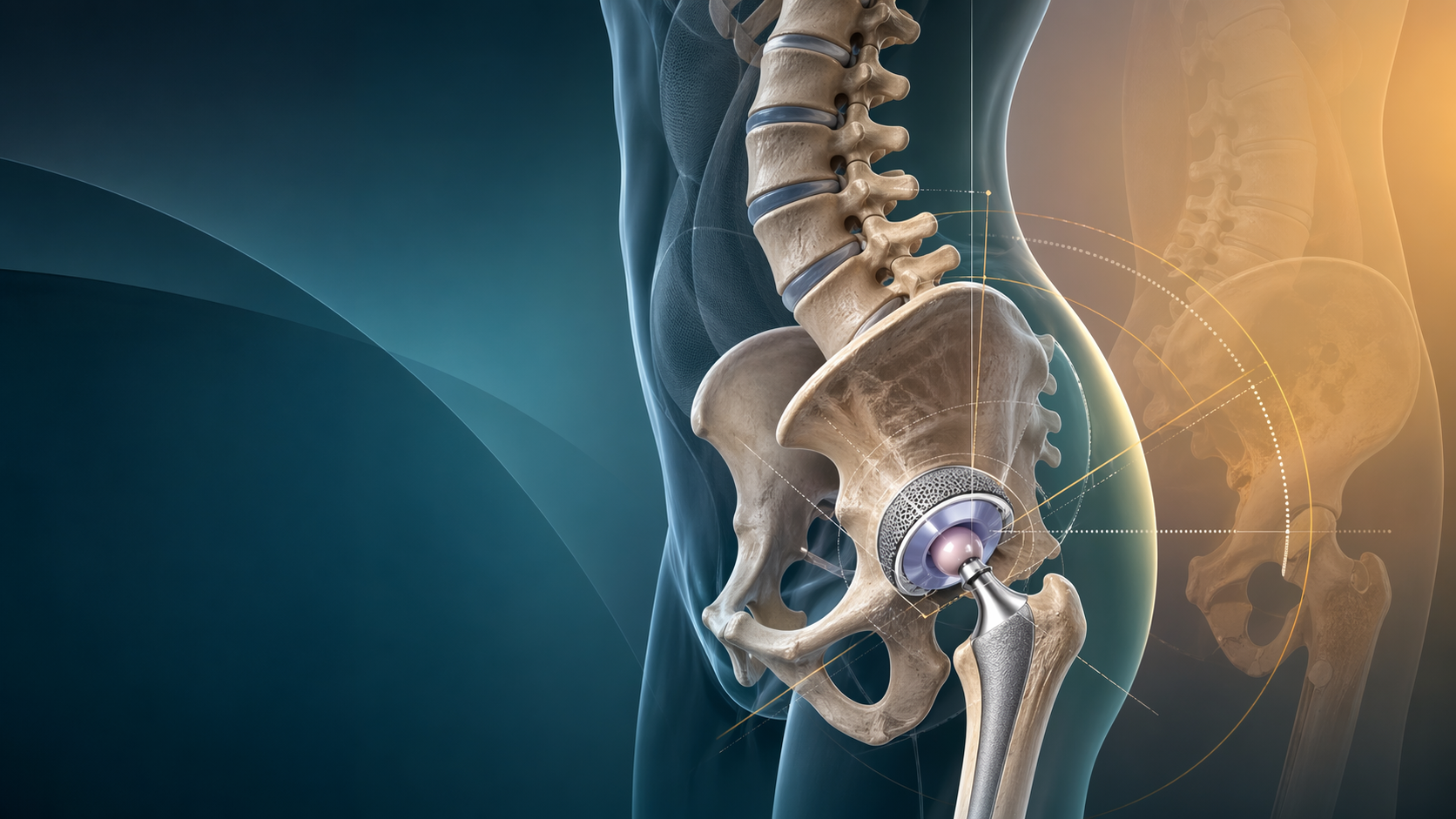
Dual Mobility Hips: Biomechanics, Indications, and Risks
Instability and dislocation remain the Achilles' heel of Total Hip Arthroplasty (THA). Despite advancements in surgical approaches, including the widespread adoption of the direct anterior approach, dislocation is consistently cited as the leading cause of revision THA within the first year post-operatively, and a major driver of late revisions.
Historically, surgeons attempted to combat instability by increasing the femoral head size (from 22mm to 32mm, 36mm, and even 40mm). While larger heads definitely improve the head-to-neck ratio and jump distance, they are limited by the patient's native acetabular anatomy. You cannot safely fit a 40mm head into a 48mm acetabulum without compromising the thickness and structural integrity of the polyethylene liner.
Enter the Dual Mobility (DM) cup. Once considered a niche European implant, it has emerged as the ultimate biomechanical solution for the unstable hip, rapidly becoming a staple in both complex primary and revision arthroplasty across the globe.
Originally conceptualised and designed by the French surgeon Gilles Bousquet and engineer André Rambert in 1974 at the University of St. Etienne, the concept was initially met with intense skepticism in North America and the UK. The early designs suffered from high rates of polyethylene wear, osteolysis, and mechanical failures. However, the advent of modern highly cross-linked polyethylene (HXLPE) has essentially solved the wear issue, sparking a massive resurgence and widespread acceptance of DM constructs.
For orthopaedic trainees and fellowship candidates, understanding the intricate biomechanics, strict indications, and unique failure modes of Dual Mobility is non-negotiable. It is highly testable in viva scenarios and critical for safe clinical practice.
The Biomechanics: How It Actually Works
The Dual Mobility construct is structurally unique because, as the name implies, it possesses two distinct articulations (sometimes referred to as a tripolar system when the shell-bone interface is considered).
- The Small Articulation (Inner): A small, captive femoral head (traditionally 22.2mm or 28mm) is forcibly press-fit (snapped) into a retentive mechanism within a large mobile polyethylene liner. This inner articulation handles the majority of motion during routine, low-demand daily activities such as steady-state walking or sitting. Because of its small radius, it generates very low frictional torque against the acetabular fixation.
- The Large Articulation (Outer): The large polyethylene liner itself acts as a massive, unconstrained prosthetic femoral head, articulating directly inside a highly polished metal acetabular shell. This secondary articulation only engages at the extremes of motion (e.g., deep flexion, rising from a low chair, cross-legged sitting) when the neck of the femoral stem impinges against the rim of the polyethylene liner, causing the entire liner to move within the metal shell.
Early critics of Bousquet's design argued that a massive polyethylene bearing surface articulating against metal would generate catastrophic wear debris.
The "French Paradox" explains why this didn't happen as rapidly as expected, even with conventional poly: While the volumetric wear (total volume of particles generated) increases with a larger bearing surface, the linear wear (the depth of penetration into the poly) actually decreases due to the load being distributed over a vastly larger surface area.
Today, with Highly Cross-Linked Polyethylene (HXLPE) essentially eliminating clinically significant wear in most patients, the paradox is less of a concern, making DM a viable long-term option even in younger, active demographics.
The "Jump Distance" Revolution
To understand why DM hips are so inherently stable, you must understand Jump Distance.
The jump distance is defined as the vertical translation the center of the femoral head must undergo to completely clear the rim of the acetabular component and dislocate. It is the primary mechanical determinant of hip stability.
- Jump Distance Formula:
- = Radius of the articulating head.
- = Angle of the cup coverage (typically an arc of 180 degrees or a hemisphere).
Let's look at the math in a clinical context:
- Standard 32mm Head: A small radius () equates to a relatively small jump distance. If the hip impinges, the head easily levers out over the rim.
- Dual Mobility Construct: The effective head size preventing dislocation is the outer diameter of the polyethylene liner (e.g., 48mm, 52mm, or even 56mm). A 52mm outer diameter () yields a massive jump distance.
Furthermore, the Dual Mobility design maximizes the Head-to-Neck Ratio. A standard 12/14 trunnion neck paired with a 50mm outer liner creates a head-to-neck ratio that permits a functional range of motion (ROM) often exceeding 120-130 degrees before any bony or component impingement occurs. It is mechanically incredibly difficult to dislocate a DM cup without catastrophic soft tissue failure or extreme trauma.
Clinical Indications: Who Needs a Dual Mobility Hip?
Despite its advantages, we do not use Dual Mobility for every primary THA. The constructs are more expensive, they introduce additional modular interfaces (which can generate fretting and corrosion), and they carry unique complications.
DM should be reserved for the "High Risk" patient. In an exam setting, you must be able to stratify these risks clearly.
1. The "Stiff Spine" and Spinopelvic Imbalance
This is currently one of the most heavily tested topics in arthroplasty. Patients with multi-level lumbar fusions (especially long constructs extending to the pelvis), severe degenerative disc disease, or ankylosing spondylitis have a "stiff spine."
Normally, when a patient transitions from standing to sitting, their lumbar spine flexes, allowing the pelvis to roll backward (posterior pelvic tilt). This dynamic retroversion functionally opens the acetabular cup anteriorly, accommodating the flexing femur and preventing anterior impingement.
In a stiff spine, the pelvis cannot roll back. It remains locked in a relatively upright or anteriorly tilted position. When the patient sits, the femur hits the anterior rim of the cup almost immediately, levering the head out posteriorly. DM provides the massive ROM forgiveness and jump distance required to compensate for this lack of spinopelvic harmony.
2. Neuromuscular and Cognitive Disorders
Patients who lack normal muscle tone or the cognitive capacity to adhere to post-operative "hip precautions" are at severe risk of early dislocation.
- Parkinson’s Disease: Tremors, rigidity, and unpredictable muscle firing patterns make standard THA perilous.
- Cerebral Palsy & Polio: Severe spasticity or profound flaccidity around the hip joint compromises the dynamic soft-tissue envelope.
- Dementia/Alzheimer's: Inability to remember not to cross legs or flex past 90 degrees.
3. Revision Surgery for Instability
Any revision operation undertaken specifically to treat recurrent instability is a mandatory indication for a constrained liner or a Dual Mobility cup. Today, DM is vastly preferred over constrained liners because constrained liners have poor ROM, impinge early, and transmit massive torsional forces to the acetabular fixation, leading to high rates of aseptic loosening and screw breakage.
DM is also the implant of choice for Abductor Deficiency. If the gluteus medius and minimus are irreparably torn or avulsed (e.g., massive greater trochanteric escape), the dynamic stabilizer of the hip is gone. The inherent mechanical stability of the DM jump distance acts as a fail-safe.
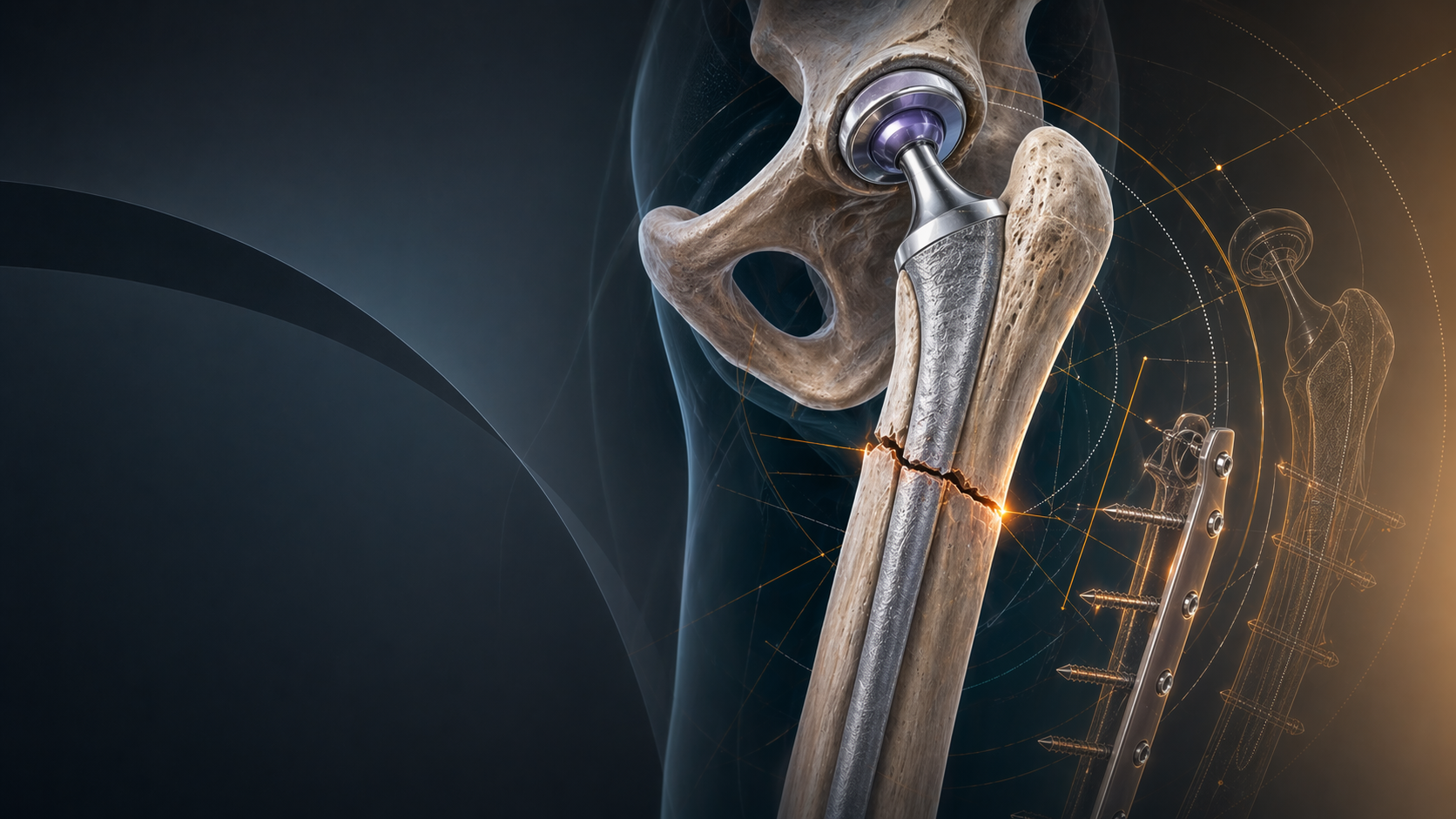
4. Femoral Neck Fractures (NOF) in the Elderly
For active, independent elderly patients suffering a displaced intracapsular neck of femur fracture, Total Hip Arthroplasty provides superior functional outcomes and longevity compared to a hemiarthroplasty. However, the dislocation rate for primary THA in the fracture setting is historically high (often quoted between 5-10%, compared to ~1% for elective osteoarthritis).
Using a Dual Mobility construct in the fracture setting drops the dislocation risk back down to baseline elective levels (<1%), combining the functional benefits of a total hip with the stability of a hemiarthroplasty.
5. High-Risk Primary Demographics
- Morbid Obesity (BMI > 40): Massive soft tissue impingement (thigh-on-abdomen) forces the hip to lever out.
- Connective Tissue Disorders: Ehlers-Danlos syndrome, Marfan syndrome, and general hyperlaxity where the capsular repair cannot be trusted to provide stability.
The Unique Complication: Intra-Prosthetic Dislocation (IPD)
While Dual Mobility dramatically reduces the risk of standard large-head dislocation, it introduces a highly specific complication that does not exist in standard THA: Intra-Prosthetic Dislocation (IPD).
This is a favourite topic for examiners because it requires specific radiographic interpretation and urgent surgical management.
The Mechanism of IPD
IPD is fundamentally a failure of the retentive mechanism holding the inner metal head inside the outer polyethylene liner. It usually occurs late (years after surgery) and follows a specific sequence, often termed the "Bottle-Opener Effect":
- Impingement: The neck of the femoral stem repeatedly impinges against the retentive rim of the polyethylene liner during extreme ROM.
- Wear: Over thousands of cycles, the hard titanium or cobalt-chrome neck wears away the polyethylene retentive chamfer.
- Jamming: Eventually, the outer liner may become jammed or completely worn against the rim of the metal acetabular shell, preventing it from moving.
- Leverage: The patient forces the leg into a position of impingement. Because the outer poly liner is stuck, the neck acts as a lever (like a bottle opener) and pries the small inner metal head entirely out of the polyethylene liner.
- The Result: The small metal head (22mm or 28mm) is now articulating directly against the large polished metal acetabular shell ("Metal on Metal" effect), while the large polyethylene liner floats completely free in the surrounding soft tissues.
Diagnosing IPD: The "Bubble Sign"
Patients with IPD will present with new-onset hip pain, a grinding sensation, and occasionally a palpable clunk, but they may still be able to weight-bear, which can trick junior doctors into thinking the hip is completely reduced.
On a standard AP Pelvis X-ray, you must look for two critical signs:
- Eccentricity: The femoral head will appear asymmetrically placed (eccentric) within the metal acetabular shell. Because the poly liner is missing, the head sits directly against the metal backing.
- The "Bubble Sign": If you adjust the contrast on the digital radiograph and look closely at the peri-articular soft tissues, you will see a faint, perfectly spherical radiolucent shadow floating outside the joint. This is the dislocated polyethylene liner.
Managing IPD
Management involves returning to the operating theatre.
- You must retrieve the floating polyethylene liner.
- You must inspect the metal acetabular shell. If the inside polish is severely scratched or damaged by the metal head, replacing the liner alone is insufficient; the new poly will rapidly wear out against the rough metal. The entire shell may need to be revised.
- You must evaluate the femoral stem neck for damage (trunnionosis or scratching) and replace the modular head.
Modular Dual Mobility (mDM): A Word of Caution
Modern reconstructive surgery often utilizes Modular Dual Mobility (mDM). Standard DM cups are "monoblock"—a single piece of metal without screw holes, coated in porous titanium for ingrowth.
However, in revision surgery, we often need to use screws to secure the cup into compromised bone. mDM systems use a standard multi-hole titanium acetabular shell. Once the shell is fixed with screws, a highly polished Cobalt-Chrome (CoCr) or Titanium alloy smooth liner is impacted into the shell via a Morse taper. The dual mobility poly liner then articulates inside this smooth modular insert.
The Risk: mDM introduces a new modular junction (Titanium shell against a CoCr/Ti insert). This interface is susceptible to micromotion, fluid ingress, fretting, and galvanic corrosion. There are increasing case reports of mDM dissociation (the metal insert falling out of the metal shell) and adverse local tissue reactions (ALTR) from corrosion. Therefore, mDM should only be used when screw fixation is absolutely mandatory; otherwise, monoblock DM is preferred.
Surgical Technique Pearls for Trainees
If you are putting in a DM cup, attention to detail is paramount to prevent premature wear and IPD:
- Clear the Perimeter: You must aggressively resect all overhanging marginal osteophytes around the acetabulum. If an osteophyte is left behind, the large poly liner will impinge on it, restricting its motion and accelerating the "bottle-opener" wear on the inner retentive mechanism.
- Stem Selection matters: Avoid using femoral stems with excessively thick or "skirted" necks. A thick neck impinges on the poly liner much earlier in the arc of motion, reducing the functional benefits of the construct. Opt for modern, smooth, highly polished, thin-necked trunnions (like a standard 12/14 taper).
- Cup Version: While DM is forgiving, you should still aim for the standard Lewinnek safe zone (15±10° anteversion, 40±10° inclination). Placing a DM cup in excessive vertical inclination (>50°) concentrates edge-loading forces on the poly liner, risking rapid wear.
Conclusion
The Dual Mobility bearing has revolutionized how orthopaedic surgeons manage the unstable hip. By brilliantly combining the low-friction advantages of a small primary articulation with the massive jump distance and stability of a large secondary articulation, it has largely solved the problem of dislocation for high-risk patients.
However, it is not a "get out of jail free" card for poor surgical technique. Understanding spinopelvic mechanics to identify the right patient, combined with meticulous intra-operative clearance of impingement, is essential. With modern HXLPE materials, the historic fears of accelerated wear have been laid to rest, establishing Dual Mobility as a safe, powerful, and essential long-term choice in the modern arthroplasty arsenal.
#Arthroplasty #HipReplacement #DualMobility #Biomechanics #OrthoImplants #RevisionHip #OrthoVellum #PatientSafety #SurgicalEducation
Related topics
Share this article
Useful for a journal club, study list, or teaching session.