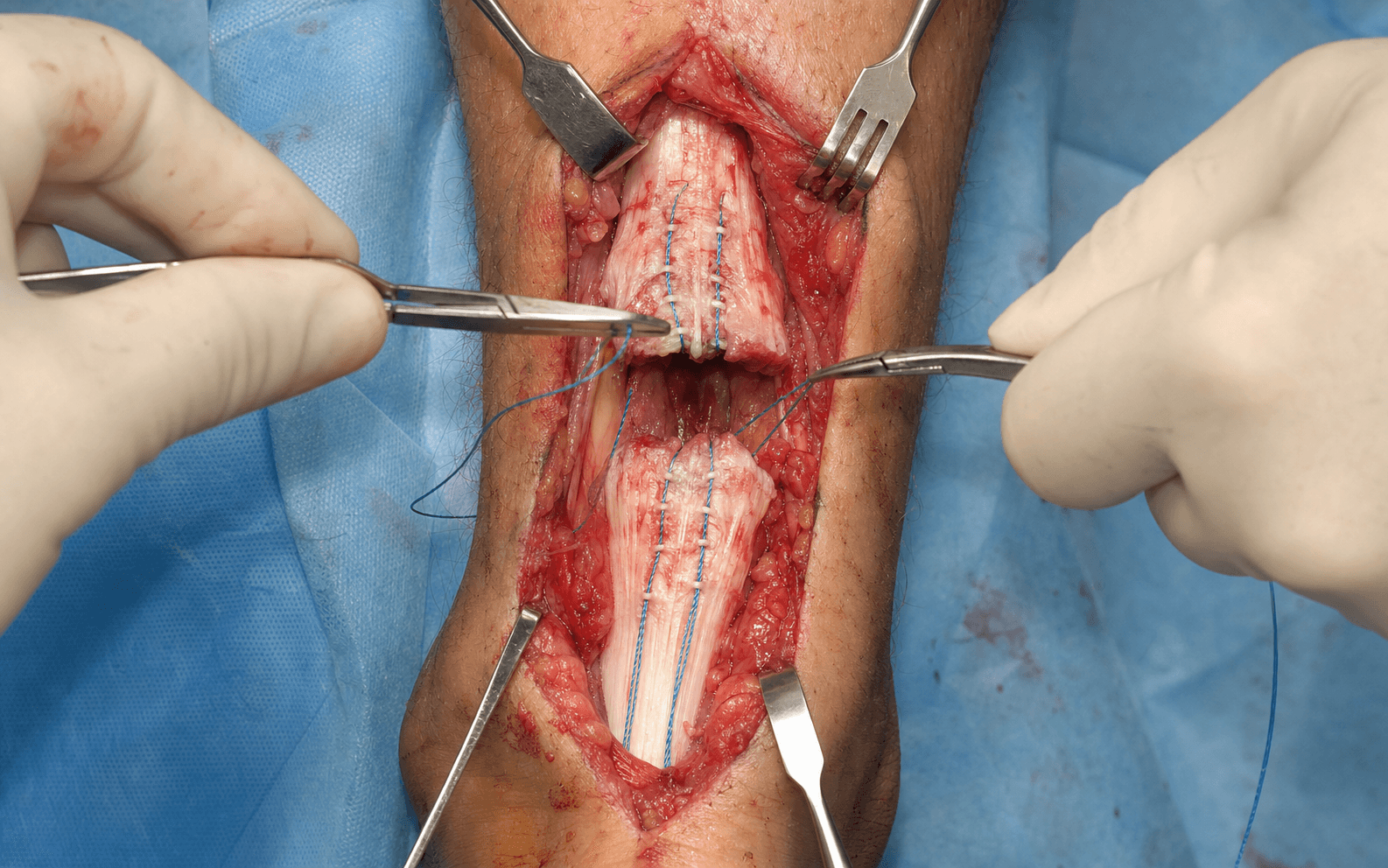
Acute rupture · posteromedial open repair · Krackow core suture with epitendinous reinforcement and paratenon closure
- The Simmonds–Thompson test is pathognomonic: with the patient prone, squeeze the calf — a normal ankle plantarflexes, a ruptured tendon shows no motion. It is roughly 96 percent sensitive and specific for complete rupture.
- Rupture typically occurs 4–6cm proximal to the calcaneal insertion, in the watershed zone (2–6cm proximal to insertion) of poorest blood supply. Peak incidence is 30–50 years, males more than females, the classic weekend-warrior athlete.
- The Krackow running locked suture is the strongest core repair — 6 or more locks in each tendon stump using non-absorbable number 2 or number 5 braided suture (Ethibond or FiberWire), ultimate load to failure 400–500N.
- A posteromedial incision placed 1cm medial to the Achilles midline protects the sural nerve, which runs posterolaterally. Full-thickness skin flaps down to paratenon preserve vascularity and reduce wound necrosis.
- Paratenon closure over the repair is critical — it reduces re-rupture by about half, adds a strength layer, brings vascularity to the repair site, and reduces adhesions to the overlying skin.
- Modern accelerated rehabilitation (immediate weight-bearing in a CAM boot with heel wedges, early range of motion from 2 weeks) does NOT increase re-rupture compared with traditional casting and gives less tendon elongation and faster return to function.
- FHL (flexor hallucis longus) transfer is the modern gold standard for chronic ruptures or gaps greater than 6cm — it is in-phase, in the same deep posterior compartment, and a strong biological augment.
When & Why
Indication. An acute Achilles tendon rupture in an active patient who, after shared decision-making and counselling, elects surgical repair to minimise re-rupture risk and maximise strength and speed of return. The diagnosis is clinical — a positive Thompson test with a palpable gap 4–6cm proximal to the calcaneal insertion — and imaging is reserved for equivocal cases or chronic rupture (ultrasound is dynamic and cheap; MRI is the gold standard for gap size, tendon-end quality, and chronic change). Operative vs non-operative — the one decision. With modern accelerated functional rehabilitation, the re-rupture difference between surgery and non-operative care is small and the trade-off is the complication profile. The high-level evidence consistently shows:
Young, active patients (typically less than 50–60 years), competitive athletes, manual labourers wanting maximal plantarflexion strength and the lowest re-rupture risk, chronic rupture in a motivated patient, or failed non-operative management.
Older sedentary patients (typically greater than 65 years), low activity level, significant medical comorbidity (diabetes, peripheral vascular disease, immunosuppression), partial rupture, or patient preference after counselling.
Surgery lowers re-rupture (modern figures about 5–10 percent operative vs 10–15 percent non-operative) but carries wound complications 5–10 percent, infection 2–5 percent, and sural nerve injury 10–15 percent. Both pathways use the same accelerated functional rehabilitation.
Consent specifically for re-rupture (5–10 percent), wound breakdown or infection (5–10 percent), sural nerve injury with lateral foot numbness or a painful neuroma (10–15 percent), DVT/PE (1–5 percent), possible over-lengthening with a weak push-off, and the small residual strength deficit that often persists. Setup. Prone with the feet hanging free over the end of the table (allows intraoperative ankle motion and tension testing); chest rolls and padding of all pressure points. Thigh tourniquet at 350mmHg. Exsanguinate by elevation rather than Esmarch, which displaces the tendon ends and haematoma and makes identification harder. General or regional anaesthesia.
The Operation
The goal: expose the rupture through a posteromedial longitudinal incision that protects the sural nerve, raise full-thickness flaps down to paratenon, freshen the tendon ends minimally, reapproximate them with a strong Krackow core suture reinforced by an epitendinous running suture, and close paratenon over the repair — then protect it with an accelerated functional rehabilitation protocol. The exposure is laid out in full as the first steps below.
Operative sequence
- Prone, feet hanging free over the end of the table so the ankle can be moved to test repair tension; pad eyes, chest, genitals, breasts and knees.
- Thigh tourniquet at 350mmHg; exsanguinate by elevation only (not Esmarch — it displaces tendon ends and haematoma).
- Palpate the rupture gap (typically 4–6cm proximal to the calcaneal insertion) and mark the course of the sural nerve, which runs posterolaterally about 1–2cm lateral to the midline with the lesser saphenous vein.
- A longitudinal posteromedial incision 10–12cm, centred over the palpable gap and placed 1cm medial to the Achilles midline — this keeps the wound away from the posterolateral sural nerve (the structure most often injured).
- Plan it to run from about 2cm distal to the gap to the proximal end of the retracted stump; extend proximally if the proximal stump has retracted out of view.
- Raise full-thickness skin and subcutaneous flaps sharply down to paratenon — carry the fat with the skin to preserve blood supply from both sides and avoid necrosis.
- Do not undermine in the subcutaneous plane (wound-complication risk). Identify and protect the lesser saphenous vein if it is encountered.
- Incise the paratenon longitudinally in line with the incision and preserve as much of it as possible for closure.
- Identify the proximal and distal stumps. The proximal end usually retracts 5–10cm proximally from gastrocnemius pull — milk it distally or extend the incision to retrieve it.
- Evacuate the haematoma from the gap and freshen the ends minimally with a scalpel, removing only obviously necrotic tissue (excessive debridement creates a gap and may force augmentation).
- Assess the gap with the ankle at 90 degrees and the knee extended: 0–3cm allows primary repair in neutral; 3–6cm needs slight plantarflexion; greater than 6cm or a chronic rupture needs augmentation.
- Use a non-absorbable braided suture (number 2 for standard repairs, number 5 for heavy patients or athletes; Ethibond, FiberWire or Ti-Cron). Never absorbable — it loses strength before the tendon heals.
- In the proximal stump, start 5–6cm from the cut end and create a running locked zigzag pattern with a minimum of 6 locks (8–10 for larger tendons), exiting at the cut end and leaving long tails.
- Mirror the technique on the distal stump. The Krackow is the strongest core configuration (400–500N ultimate load), superior to a modified Kessler (300–400N) or Bunnell (250–350N).
- Set the ankle in neutral to slight plantarflexion (10–15 degrees) — NOT excessive plantarflexion, which raises DVT risk and later contracture while giving no re-rupture benefit.
- Bring the tendon ends together and tie the core sutures with 4–6 square knots; tension should be snug but not over-tight, and knots buried within the repair.
- Add a circumferential epitendinous running (baseball) suture with absorbable 2-0 or 3-0 (Vicryl, PDS, Monocryl), taking perpendicular bites around the repair edge for 2–3 passes.
- This reinforces the core (adds 10–25 percent strength), smooths the contour, and reduces adhesions to the paratenon. The core is essential; the epitendinous layer is the adjunct.
- Indicated for a gap greater than 6cm, a chronic rupture older than 6 months, poor tissue quality, or revision.
- FHL transfer (modern gold standard): via a medial approach, harvest FHL proximal to the knot of Henry (protecting FDL and the posterior tibial neurovascular bundle), drill two 5–7mm tunnels in the posterior calcaneus, route FHL through the tunnels, and suture it under tension to both stumps. It is in-phase, in the same deep posterior compartment, and a strong vascularised augment.
- Alternatives: gastrocnemius turndown flap (inverted V-flap from the proximal aponeurosis, turned down over the repair), V-Y lengthening (gains 2–4cm for a contracted chronic rupture), or Achilles/semittendinosus allograft for salvage.
- Deflate the tourniquet and gently passively dorsiflex the ankle to neutral — the repair should hold without gapping (if it gaps, reinforce or re-tension).
- Compare resting tension and the Thompson response with the contralateral side: excessive plantarflexion means over-tight (redo); excessive dorsiflexion means loose (redo). Mark the resting ankle position for splinting.
- Close the paratenon over the repair with a running absorbable suture (3-0 Vicryl/Monocryl) without tension — this reduces re-rupture by about half, adds strength, brings vascularity, and reduces adhesions.
- Achieve meticulous haemostasis (haematoma drives wound complications and infection); consider a surgical drain for 12–24 hours if there is oozing.
- Deep dermal absorbable layer, then skin with interrupted nylon or a subcuticular absorbable. Apply a below-knee backslab in the marked position (neutral to slight plantarflexion).
The sural nerve runs posterolateral to the Achilles in the subcutaneous tissue, about 1–2cm lateral to the midline at the rupture level, travelling with the lesser saphenous vein. Injury (numbness of the lateral foot and heel, or a painful neuroma) occurs in 10–15 percent of open repairs. Prevent it with a posteromedial incision 1cm medial to midline, full-thickness flaps, gentle retraction, and direct visualisation if the nerve is encountered.
When augmenting with an FHL transfer, the posterior tibial neurovascular bundle (3–4cm deep and medial, in the tarsal tunnel with FDL and FHL) is at risk during the medial harvest. Stay orientated, protect FDL and the bundle, and visualise the deep structures directly rather than working blind.
Set the ankle in neutral to slight plantarflexion (10–15 degrees) when tying the core. Multiple studies show neutral is safe and does not increase re-rupture, while excessive plantarflexion (greater than 20 degrees) raises DVT risk and causes later contracture and limited dorsiflexion with no re-rupture benefit.
Closing paratenon over the repair is the step candidates omit — and the one examiners probe. It reduces re-rupture by about 50 percent in some studies, adds a strength layer, brings vascular tissue to the healing tendon, and prevents adhesions between tendon and the overlying skin and subcutaneous tissue. Perform it in every open repair.
Aftercare & Complications
Accelerated functional rehabilitation | Phase | Timing | Protection | Activity | |-------|--------|------------|----------| | 1 | 0–2 weeks | CAM boot with 3 heel wedges (about 20 degrees plantarflexion); sutures out at 2–3 weeks | Weight-bearing as tolerated; ankle pumps | | 2 | 2–4 weeks | Remove 1 wedge (about 10 degrees plantarflexion) | Gentle ROM, no resistance; continue weight-bearing | | 3 | 4–6 weeks | Remove final wedge to neutral | Progressive ROM; begin isometric strengthening | | 4 | 6–12 weeks | Wean boot to a shoe with a heel lift | Progressive strengthening and proprioception | | 5 | 3–6 months | — | Running progression and sport-specific training | | 6 | 6–9 months | — | Return to sport, gated by functional testing | Return to sport is decided by function, not the calendar: a single-leg calf raise of 20 or more repetitions equal to the contralateral side, hop testing at 80 percent or more of the contralateral distance, and isokinetic strength at 90 percent or more. Add thromboprophylaxis (LMWH or aspirin) for 6 weeks. Expect a 6–12 month plateau and a residual calf-strength deficit of 5–15 percent at a year, improving to less than 5 percent by two years; about 80–90 percent return to their pre-injury sport. Lifetime re-rupture risk is about 2–5 percent, with most re-ruptures occurring at 6–12 weeks from premature loading. Complications
- Recognition
- Sudden pop during rehab, palpable gap, positive Thompson; 5–10 percent open, 10–15 percent non-operative
- Prevention
- Strong Krackow core, epitendinous reinforcement, paratenon closure, protected accelerated rehab, functional testing before sport
- Management
- Acute (less than 6 weeks): revision open repair with augmentation; chronic: augmentation mandatory; non-operative for the low-demand patient
- Recognition
- Wound breakdown, drainage, erythema; deep dehiscence exposes tendon; 5–10 percent
- Prevention
- Posteromedial incision, full-thickness flaps, meticulous haemostasis, paratenon closure, tension-free layered closure, smoking cessation, diabetic optimisation
- Management
- Superficial: wound care and oral antibiotics; deep: IV antibiotics, debridement, negative-pressure therapy, rarely flap cover
- Recognition
- Numbness or dysaesthesia of the lateral foot and heel; possible painful neuroma; 10–15 percent open
- Prevention
- Posteromedial incision 1cm medial to midline, full-thickness flaps, careful subcutaneous dissection, gentle retraction
- Management
- Most are neuropraxia — observe, improve over 3–6 months; permanent numbness usually tolerated; painful neuroma may need excision or relocation
- Recognition
- Calf pain, swelling, warmth; PE with dyspnoea and chest pain; 1–5 percent
- Prevention
- Thromboprophylaxis (LMWH or aspirin 6 weeks), ankle neutral not excessive plantarflexion, early mobilisation, ankle pumps
- Management
- Urgent venous duplex; anticoagulation for 3–6 months; PE — CT pulmonary angiography, anticoagulation, ICU if massive
- Recognition
- Weak plantarflexion, unable to single-leg calf raise, diminished push-off; 5–15 percent
- Prevention
- Minimal debridement, neutral ankle position, intraoperative tension testing, augmentation for gap greater than 6cm
- Management
- Physiotherapy, heel lift, activity modification; severe cases — tendon-shortening or salvage; often a permanent deficit
- Recognition
- Limited dorsiflexion versus contralateral, equinus posture; 5–10 percent
- Prevention
- Repair in neutral to slight plantarflexion (not greater than 20 degrees), early ROM from 2 weeks
- Management
- Aggressive stretching and physiotherapy; serial casting if severe; surgical lengthening (V-Y) as salvage
- Recognition
- Stiffness, reduced excursion, pain with ankle motion
- Prevention
- Paratenon closure, smooth epitendinous repair, early ROM
- Management
- Manual therapy and progressive ROM; persistent restricting adhesions — adhesiolysis (rare)
- Recognition
- Persistent insertional or mid-substance pain beyond 6 months; 10–20 percent with some residual symptoms
- Prevention
- Anatomic repair, paratenon closure, gradual return to activity, avoid overuse
- Management
- Activity modification, eccentric strengthening (Alfredson), shockwave; persistent — surgical debridement as salvage
Viva & Exam Focus
ACHILLESACHILLES — repair technique essentials
THOMPSONTHOMPSON — clinical diagnosis
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old recreational basketball player felt a sudden snap in his right calf during a game three days ago — 'kicked from behind' — and has a palpable gap 5cm proximal to his heel. How do you decide between operative and non-operative management?”
“You have decided to proceed with open repair of an acute Achilles rupture. Walk me through your technique step by step, explaining the evidence behind each critical decision.”
“A patient is eight months out from an Achilles repair and now has a palpable gap and a positive Thompson test — a re-rupture. How do you manage this, and how does it differ from a primary repair?”
Indication
- Acute rupture in active patients (typically less than 50–60 years), athletes, manual labourers
- Shared decision-making: young active favours surgery, elderly sedentary favours non-operative
- Chronic rupture or failed non-operative management in a motivated patient
Exposure & danger structures
- Posteromedial incision 10–12cm, 1cm medial to the midline (protects the posterolateral sural nerve)
- Full-thickness flaps to paratenon preserve vascularity
- At risk: sural nerve and lesser saphenous vein (superficial); FHL and posterior tibial neurovascular bundle (deep, during FHL harvest)
Core repair
- Krackow running locked — 6 or more locks each stump, non-absorbable number 2 or 5, 400–500N
- Ankle in neutral to slight plantarflexion (10–15 degrees), NOT excessive
- Epitendinous baseball suture adds 10–25 percent strength and a smooth surface
Closure & splinting
- Paratenon closure is critical — halves re-rupture, adds strength and vascularity
- Meticulous haemostasis; consider a drain; layered tension-free closure
- Below-knee backslab in the marked resting position
Rehabilitation
- Accelerated: immediate weight-bearing in a CAM boot with 3 heel wedges; remove 1 wedge every 2 weeks to neutral at 6 weeks
- ROM from 2 weeks; wean boot 6–8 weeks; return to sport 6–9 months by functional testing
- Thromboprophylaxis (LMWH or aspirin) for 6 weeks
Evidence
- With accelerated functional rehab, re-rupture differences are small (Ochen 2019: 2.3 percent vs 3.9 percent)
- Surgery's trade-off is higher wound/infection and sural nerve risk
- Augmentation (FHL) for gap greater than 6cm or chronic rupture
Background & Evidence
Epidemiology. The incidence of Achilles tendon rupture is rising worldwide, commonly reported at about 18–40 per 100,000 population annually in high-income settings, driven by greater recreational sport participation and an ageing active population. Peak age is 30–50 years (the classic weekend warrior), with a male predominance of about 4–5:1. Typical mechanisms are sudden eccentric loading — push-off, jumping, sprinting — in basketball, racquet sports, football, and recreational running. Recognised risk factors are fluoroquinolone antibiotics (boxed warnings from both US FDA and European EMA), corticosteroid use (systemic or local peritendinous), inflammatory arthropathy and metabolic disease (diabetes, obesity), pre-existing Achilles tendinopathy, and poor training progression. Anatomy and blood supply. The Achilles is the largest and strongest tendon in the body — about 15cm long from the gastrocnemius–soleus junction to the calcaneus, 5–6cm wide proximally narrowing to 2–3cm, and 5–7mm thick. Gastrocnemius fibres spiral 90 degrees to insert posterolaterally on the calcaneus. Blood supply comes from the musculotendinous junction proximally, periosteal vessels from the calcaneus distally, and the paratenon throughout (which provides about 25–30 percent of the supply — preserve it). The watershed zone, 2–6cm proximal to the insertion, has the poorest blood supply and is where about 90 percent of ruptures occur. Classification. Ruptures are classified by timing, by the anatomic gap (measured with the ankle at 90 degrees and the knee extended), and by tissue quality — each guiding whether primary repair alone suffices or augmentation is required.
- Timing
- Less than 6 weeks from injury
- Tissue and gap
- Fresh ends with good-quality tissue, minimal retraction
- Typical management
- Primary end-to-end repair without augmentation; best outcomes
- Timing
- 6 weeks to 6 months
- Tissue and gap
- Possibly degenerative ends, moderate retraction and gap formation
- Typical management
- Primary repair; consider augmentation if gap greater than 3–4cm
- Timing
- Greater than 6 months
- Tissue and gap
- Significant degeneration and scarring, gap typically greater than 6cm
- Typical management
- Augmentation mandatory (FHL, gastrocnemius turndown, allograft); guarded outcomes
- Management
- Primary end-to-end repair in neutral; standard core suture; no augmentation
- Prognosis
- Excellent
- Management
- Primary repair with ankle in slight plantarflexion (10–15 degrees); strong core suture; consider epitendinous augmentation
- Prognosis
- Good with proper technique
- Management
- Augmentation required — FHL transfer preferred; gastrocnemius turndown or allograft as alternatives
- Prognosis
- Guarded
- Open
- 5–10 percent
- Percutaneous
- 8–12 percent
- Non-operative
- 10–15 percent
- Open
- 5–10 percent
- Percutaneous
- 2–3 percent
- Non-operative
- 0 percent
- Open
- 5–10 percent
- Percutaneous
- 10–15 percent (blind technique)
- Non-operative
- Less than 1 percent
- Open
- 80–90 percent good-excellent
- Percutaneous
- Similar
- Non-operative
- Similar with accelerated functional rehab
Guidelines and global practice. Modern guidance has converged on accelerated functional rehabilitation for both pathways, with re-rupture differences that are statistically small and a complication burden weighted toward surgery.
- Position on acute rupture
- Both operative and non-operative treatment are acceptable; the evidence does not strongly favour one; emphasises functional rehabilitation and shared decision-making
- Position on acute rupture
- Supports functional (non-operative) management with early rehabilitation as a mainstream pathway; surgery reserved for selected patients and re-ruptures
- Position on acute rupture
- Technique-focused: anatomic repair, strong core suture, paratenon closure, early protected functional rehabilitation
- Position on acute rupture
- Re-rupture differences are small with modern functional rehabilitation; the complication profile (infection, sural nerve) is the main trade-off favouring non-operative care
References
Operative versus nonoperative treatment of acute Achilles tendon ruptures with accelerated functional rehabilitation
- Multicentre RCT of 144 patients; BOTH arms used accelerated functional rehabilitation (early weight-bearing and early ROM)
- Re-rupture in 2 of 72 operative and 3 of 72 non-operative patients — no clinically important difference
- No clinically important difference in isokinetic strength, ROM, calf circumference or Leppilahti score
- Thirteen complications in the operative group versus six non-operative, mainly soft-tissue complications with surgery
Operative treatment versus nonoperative treatment of Achilles tendon ruptures: systematic review and meta-analysis
- Largest pooled dataset: 29 studies, 15,862 patients (10 RCTs and 19 observational studies)
- Re-rupture operative 2.3 percent versus non-operative 3.9 percent (RR 0.43); absolute risk difference only 1.6 percent
- Complications higher with surgery (4.9 percent versus 1.6 percent, RR 2.76), driven mainly by infection (2.8 percent operative)
- With accelerated functional rehabilitation and early ROM, no significant re-rupture difference (RR 0.60, p=0.23)
Surgical versus nonsurgical treatment of acute Achilles tendon rupture: a meta-analysis of randomized trials
- Meta-analysis of 10 RCTs comparing surgical and conservative treatment
- With early-ROM functional rehabilitation, re-rupture rates were equal (risk difference 1.7 percent, p=0.45)
- Without early ROM, surgery reduced re-rupture by an absolute 8.8 percent (p=0.001)
- Surgery increased non-re-rupture complications by 15.8 percent but allowed return to work 19 days sooner
Treatment of acute Achilles tendon ruptures: a meta-analysis of randomized, controlled trials
- Twelve RCTs, 800 patients; pre-dates routine accelerated rehabilitation
- Open repair reduced re-rupture versus non-operative treatment (relative risk 0.27)
- Open repair increased other complications (RR 10.6: infection, adhesions, disturbed skin sensibility)
- Percutaneous repair lowered complications versus open; postoperative functional bracing reduced overall complications versus rigid cast
Randomized controlled trial of accelerated rehabilitation versus standard protocol following surgical repair of ruptured Achilles tendon
- RCT of 51 patients comparing accelerated versus standard post-operative rehabilitation after repair
- Accelerated group had less tendon lengthening (0.39cm versus 1.00cm)
- Accelerated group returned to running faster (17.2 versus 21.1 weeks)
- Achilles Total Rupture Score at 12 months was similar between groups
Comparison of FHL tendon transfer and turndown flaps for chronic Achilles re-ruptures
Establishes FHL transfer as superior to gastrocnemius turndown for chronic Achilles rupture reconstruction — in-phase muscle, strong biological augmentation, better outcomes.
Major functional deficits persist 2 years after acute Achilles tendon rupture
Long-term outcome study showing a persistent 5–15 percent strength deficit versus the contralateral side at 2 years — emphasising intensive rehabilitation and realistic patient counselling.
The non-operative functional management of patients with a rupture of the tendo Achillis leads to low rates of re-rupture and high patient satisfaction
Modern functional bracing with accelerated rehabilitation achieves good outcomes non-operatively, with re-rupture rates approaching surgical series.
Clinical outcomes and complications of percutaneous Achilles repair system versus open technique for acute Achilles tendon ruptures
Percutaneous techniques have lower wound complications (2–3 percent versus 5–10 percent) but similar or higher sural nerve injury (10–15 percent) due to the blind technique, with similar re-rupture rates.
Achilles tendon ruptures in elite athletes
Review of elite-athlete outcomes showing 80–90 percent return to pre-injury level with modern surgical techniques and accelerated rehabilitation.
A new treatment of ruptured Achilles tendons. A prospective randomized study
Classic study establishing the importance of early functional rehabilitation and the benefits of immediate mobilisation over prolonged casting for both operative and non-operative treatment.