Midline laparotomy · superior hypogastric plexus preservation · L5–S1 ALIF
- Midline transperitoneal laparotomy provides direct access to L5–S1 but crosses the peritoneal cavity.
- Superior hypogastric plexus lies in the presacral fascia over the sacral promontory — blunt midline dissection only, no monopolar diathermy.
- Left common iliac vein is the dominant vascular danger during mobilisation between the iliac vessels.
- Access surgeon (general or vascular) is strongly recommended for safe peritoneal and vascular mobilisation.
- Retrograde ejaculation risk in males from plexus injury (1–5 percent) — discuss explicitly in consent.
When & Why
What it exposes. The anterior transperitoneal approach delivers direct midline access to the L5–S1 disc, the sacral promontory and the adjacent vertebral bodies through a midline laparotomy. It gives the most direct trajectory to the lumbosacral junction and allows straightforward placement of a large lordotic interbody cage. Why transperitoneal (and why it is now a niche route). The transperitoneal route is the most direct midline path to L5–S1, especially useful when the iliac crest is high or when previous left retroperitoneal surgery has created dense scarring. It crosses the peritoneal cavity, requires bowel mobilisation, and carries a small but real risk of retrograde ejaculation from superior hypogastric plexus injury. Modern practice has shifted heavily toward the left retroperitoneal approach for most primary ALIF procedures; transperitoneal is reserved for selected L5–S1 cases but remains a core examinable topic. Indications:
- Isolated L5–S1 degenerative disc disease requiring ALIF
- L5–S1 spondylolisthesis (low-grade) with disc degeneration
- Revision ALIF at L5–S1 when the retroperitoneal plane is scarred
- High-riding iliac crest anatomy precluding safe retroperitoneal access
- Selected cases of L5–S1 pseudarthrosis after posterior fusion Contraindications:
- Prior major abdominal surgery with extensive adhesions (relative)
- Active intra-abdominal infection or inflammatory bowel disease
- Morbid obesity with difficult peritoneal access
- Patient refusal of access surgeon involvement
- Need for multilevel fusion (L4–S1 or more) — retroperitoneal or combined is better Alternative approaches:
- Left retroperitoneal approach — preferred for most primary ALIF procedures
- Right retroperitoneal approach — rarely used due to liver and IVC position
- Lateral transpsoas (XLIF/DLIF) — for L2–L5, not L5–S1
- Posterior approaches (PLIF/TLIF) — avoid anterior vascular and plexus risks entirely Position & landmarks. Supine on a radiolucent table with 10–15 degrees of Trendelenburg so the bowel falls cephalad, lumbar lordosis maintained with a small bolster. A general or vascular access surgeon performs the approach. A Foley catheter decompresses the bladder, bilateral sequential compression devices are applied, arms are abducted less than 90 degrees or tucked, and a cell saver with blood products is immediately available. Surface landmarks are the umbilicus (level of L3–L4), the pubic symphysis (inferior limit), the linea alba (midline avascular plane) and the palpable rectus edges. The incision is a vertical midline laparotomy from just below the umbilicus to just above the pubic symphysis (10–15 cm), extended proximally or distally if multilevel exposure or difficult mobilisation is anticipated.
Prolonged steep Trendelenburg can cause facial and laryngeal oedema, increased intraocular pressure and reduced venous return. Limit the angle and duration, and communicate regularly with the anaesthetic team.
The Exposure
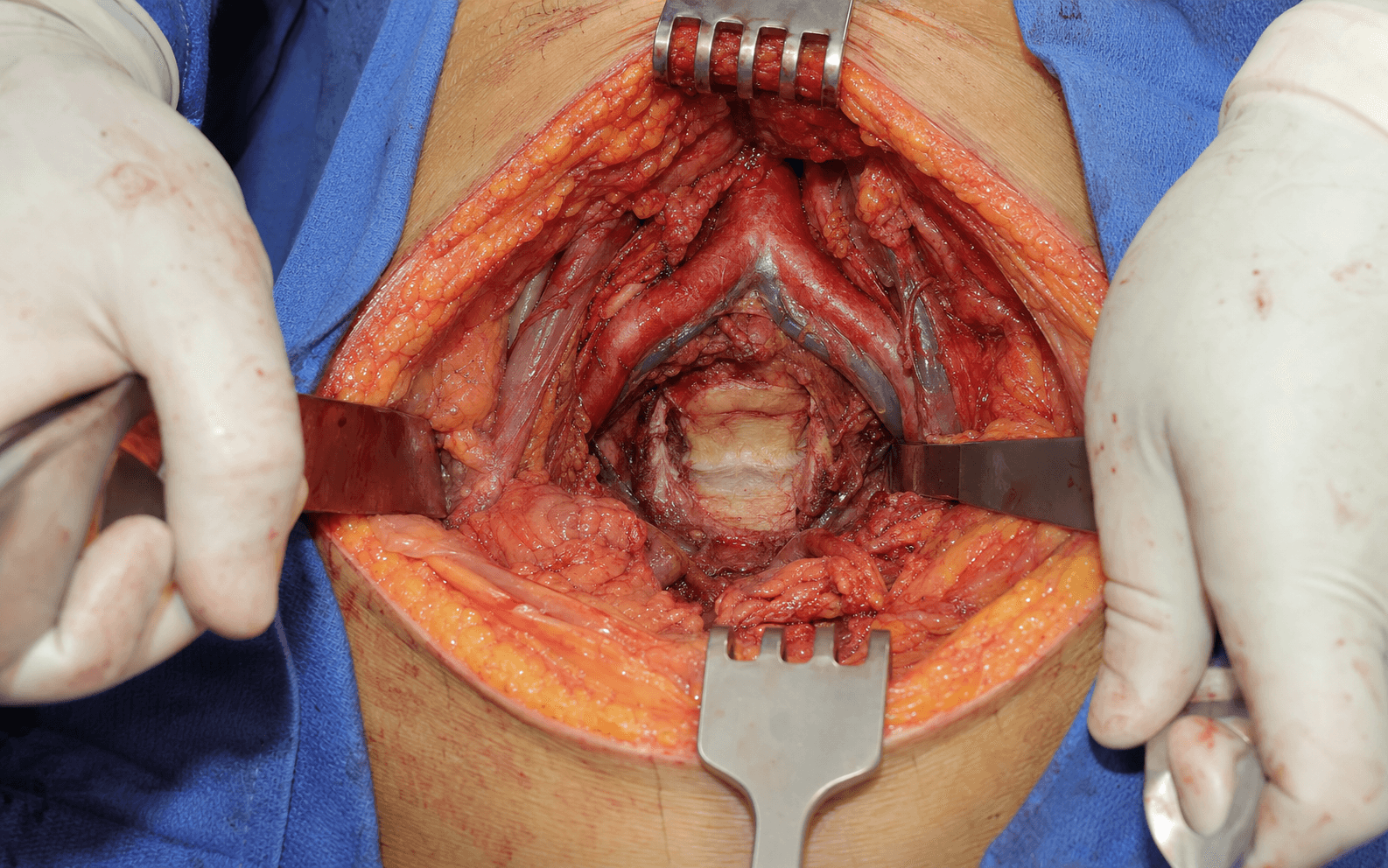
Work down through the abdominal wall in the midline, mobilise the bowel, then open the posterior peritoneum strictly over the sacral promontory, bluntly preserve the superior hypogastric plexus, control the middle sacral vessels, and mobilise the left common iliac vein to reveal the L5–S1 disc.
Exposure sequence
- Incise skin and subcutaneous fat in the midline and identify the linea alba.
- Split the linea alba sharply in the avascular midline plane; retract the rectus abdominis laterally — no muscle is divided.
- Open the peritoneum carefully, protecting the underlying bowel with a finger or instrument.
- Pack the small bowel superiorly and to the right using moist laparotomy pads.
- Mobilise the sigmoid colon laterally if it overlies the sacral promontory.
- The goal is to expose the posterior peritoneum over the lumbosacral junction.
- Identify the sacral promontory by palpation.
- Incise the posterior peritoneum strictly in the midline over the promontory and extend proximally and distally as needed (usually 4–6 cm).
- Stay exactly midline to avoid the plexus and the ureters (which lie more laterally).
- Visualise the superior hypogastric plexus as a fine network of sympathetic fibres within the presacral fascia.
- Using a Kittner or peanut dissector, gently sweep the plexus fibres laterally to both sides.
- Never use monopolar diathermy in this plane; if bleeding occurs, apply direct pressure rather than diathermy.
- Identify the middle sacral artery and vein running in the midline over the promontory.
- Ligate or clip them with bipolar diathermy or vascular clips — never monopolar near the plexus.
- This clears the midline before vascular mobilisation.
- The left common iliac vein crosses the L5–S1 disc obliquely from right to left — identify it early.
- Place vessel loops or silastic slings for gentle retraction and mobilise the vein leftward using blunt dissection and Kittner swabs.
- Mobilise the right common iliac artery rightward; protect the vein with a vein retractor during disc preparation — this creates the safe window to the disc.
- With the vessels protected, incise the anterior longitudinal ligament and annulus in the midline.
- Perform a thorough discectomy with endplate preparation for cage insertion.
- The access surgeon remains scrubbed to maintain retraction and manage any vascular issue.
- Copious warm saline irrigation and meticulous haemostasis of all peritoneal and mesenteric vessels.
- Close the posterior peritoneum with absorbable suture (restores the peritoneal barrier, reduces adhesions).
- Close the linea alba with a mass-closure technique using heavy absorbable or non-absorbable suture; close subcutaneous tissue in layers and skin.
- Obtain AP and lateral radiographs in theatre to confirm cage position and alignment.
The superior hypogastric plexus is the most important neurological structure at risk and the source of the approach's signature complication — retrograde ejaculation in males (reported at 1–5 percent), caused by sympathetic denervation of the bladder neck. It lies within the presacral fascia over the sacral promontory. Protect it with three rules only: blunt dissection (Kittner or peanut), strict midline trajectory, and absolute avoidance of monopolar diathermy. Identify the plexus visually as a fine network of fibres and sweep it laterally before exposing the disc. If bleeding occurs, use direct pressure — never blind diathermy in panic.
The left common iliac vein crosses the L5–S1 disc obliquely and is the most common source of major bleeding. Identify it early, isolate it with vessel loops, retract it gently leftward, and protect it with a vein retractor during discectomy. A tear here causes rapid, life-threatening haemorrhage — have vascular instruments, Fogarty catheters and blood products immediately available. Published injury rates are less than 2 percent with experienced access surgeons.
Dangers & Extensions
Structures at risk, by layer
- Structure at risk
- Rectus abdominis and linea alba
- Protection strategy
- Midline split of the linea alba, lateral retraction only — no muscle divided
- Structure at risk
- Small bowel and sigmoid colon
- Protection strategy
- Careful packing superiorly and laterally with moist pads
- Structure at risk
- Superior hypogastric plexus
- Protection strategy
- Blunt midline dissection, visual identification, lateral Kittner sweep, no monopolar
- Structure at risk
- Middle sacral artery and vein
- Protection strategy
- Bipolar ligation or vascular clips before disc exposure
- Structure at risk
- Left common iliac vein
- Protection strategy
- Early identification, vessel loop isolation, gentle leftward retraction, vein retractor protection
- Structure at risk
- Ureters (on the psoas fascia)
- Protection strategy
- Stay strictly midline; avoid excessive lateral peritoneal opening
- Structure at risk
- L5–S1 disc and vertebral bodies
- Protection strategy
- Subperiosteal exposure only after vascular mobilisation
Intra-operative complications
- Prevention
- Blunt midline dissection, no monopolar, visual identification
- Management
- Document, refer to sexual medicine, consider sperm banking
- Prevention
- Early identification, vessel loops, gentle retraction
- Management
- Immediate pressure, proximal and distal control, vascular repair, blood products
- Prevention
- Bipolar ligation before disc work
- Management
- Direct pressure, clips, bipolar haemostasis
- Prevention
- Strict midline peritoneal incision
- Management
- On-table imaging, urology consult, repair or stent
- Prevention
- Careful packing and entry technique
- Management
- Primary repair or resection if full thickness
- Prevention
- Avoid prolonged retraction; systemic heparin if indicated
- Management
- Embolectomy, vascular repair
Post-operative complications
- Incidence
- 1–5 percent
- Prevention
- Plexus preservation technique
- Treatment
- Alpha-agonists, fertility counselling
- Incidence
- 2–5 percent
- Prevention
- SCDs, chemoprophylaxis
- Treatment
- Anticoagulation
- Incidence
- 1–3 percent
- Prevention
- Prophylactic antibiotics, meticulous closure
- Treatment
- Antibiotics, drainage if required
- Incidence
- 2–5 percent
- Prevention
- Mass closure of the linea alba
- Treatment
- Surgical repair if symptomatic
- Incidence
- 3–8 percent
- Prevention
- Peritoneal closure, minimal bowel handling
- Treatment
- Conservative or surgical lysis
- Incidence
- 5–15 percent
- Prevention
- Adequate endplate preparation, appropriate cage
- Treatment
- Revision fusion
The risk of retrograde ejaculation after transperitoneal ALIF is reported between 1 and 5 percent in males. The risk is lower with the retroperitoneal approach (less than 1 percent) because the plexus is not directly crossed. All male patients must be counselled pre-operatively about this specific risk and the discussion documented. Sperm banking should be offered if the patient desires future fertility.
Extensile options. Extend the peritoneal incision proximally along the left side of the aorta to reach L4–L5, but this requires extra mobilisation of the left common iliac vein and L4 segmental vessels and is rarely done through a purely transperitoneal route. Distal extension is limited by the pubic symphysis and sacral curvature — the approach cannot usefully extend below S1. For a 360-degree fusion, the anterior stage is completed first, then the patient is repositioned prone for posterior pedicle screw instrumentation. If the transperitoneal route proves unexpectedly difficult (dense adhesions, obese patient, poor visualisation), convert by closing the peritoneum and developing the left retroperitoneal plane from the same incision. Recovery & monitoring. Full weight bearing is permitted from the day of surgery (anterior column support from the cage), with no heavy lifting or bending for 6–12 weeks. DVT prophylaxis (LMWH or aspirin) is started within 24 hours. The Foley remains until ileus resolves (24–48 hours), with diet advanced as tolerated. Follow-up at 2 weeks (wound check), 6 weeks (radiographs), 3 months (CT if cage position is uncertain) and 6–12 months (confirm fusion). Enquire about sexual function in male patients at 3 and 6 months and document the response. Outcomes. L5–S1 ALIF achieves fusion rates exceeding 90 percent with modern cages and graft substitutes, with clinical success (ODI improvement greater than 15 points) in 80–85 percent of primary cases. Retrograde ejaculation persists long-term in approximately 1–3 percent of males. Adjacent segment degeneration occurs at 5–10 percent per year but is often asymptomatic, and revision rates for pseudarthrosis or hardware issues are 5–10 percent at 5 years. Good prognostic factors are isolated L5–S1 pathology, no prior abdominal surgery, access surgeon involvement, meticulous plexus preservation, a large lordotic cage with good endplate coverage, and a non-smoker with good bone quality.
Procedures Through This Approach
- L5–S1 ALIF — isolated, or as the anterior stage of a 360-degree fusion with posterior lumbar decompression and fusion (PLDF).
- L5–S1 disc arthroplasty (rare).
- L5–S1 pseudarthrosis revision when the retroperitoneal plane is scarred.
- Selected high-grade spondylolisthesis reduction.
- Biopsy or debridement of an L5–S1 disc space infection.
Viva & Exam Focus
LAPAROTOMYTRANSPERITONEAL L5–S1 ALIF — key steps
Exam Viva Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old male with isolated L5–S1 degenerative disc disease and high iliac crests is planned for ALIF. Which approach would you use and how would you protect the critical structures?”
“A 35-year-old male is listed for L5–S1 ALIF. He asks specifically about the risk of retrograde ejaculation and whether the transperitoneal or retroperitoneal route is safer. How do you counsel him?”
“During transperitoneal L5–S1 ALIF, brisk bleeding occurs while mobilising the left common iliac vein. What is your immediate response and subsequent management?”
Position & incision
- Supine with 10–15 degree Trendelenburg tilt
- Access surgeon (general or vascular) essential
- Vertical midline laparotomy below the umbilicus to above the pubis
- Foley catheter for bladder decompression
- Cell saver and vascular instruments available
Plexus protection (critical)
- Superior hypogastric plexus in the presacral fascia over the promontory
- Strict midline peritoneal incision only
- Blunt dissection with Kittner or peanut only
- Visual identification then lateral sweep
- Absolute ban on monopolar diathermy in this plane
Vascular mobilisation
- Left common iliac vein crosses the disc obliquely — dominant danger
- Identify early and isolate with vessel loops
- Mobilise the vein leftward and the artery rightward
- Ligate the middle sacral vessels with bipolar or clips first
- Vein retractor protects during disc preparation
Danger structures per layer
- Abdominal wall: linea alba (split, not divided)
- Peritoneal: bowel (pack carefully)
- Presacral: plexus (blunt, midline, no monopolar)
- Vascular: left CIV (most common bleeding source)
- Lateral: ureters (stay midline)
Procedures through this approach
- L5–S1 ALIF (isolated or 360-degree fusion)
- L5–S1 pseudarthrosis revision when retroperitoneal scarred
- Selected high-grade spondylolisthesis reduction
- Biopsy or debridement of L5–S1 disc infection
Closure & consent points
- Posterior peritoneum closed with absorbable suture
- Linea alba mass-closure technique
- Discuss retrograde ejaculation (1–5 percent in males)
- Discuss vascular injury and transfusion risk
- Access surgeon involvement reduces complications
References
Guidelines & global practice. Anterior lumbar approaches are performed worldwide, and the core principles — plexus preservation, vascular safety and access surgeon involvement — are consistent across examination systems. AO Spine and NASS guidance emphasise that anterior lumbar surgery should be performed with vascular or general surgical support when the transperitoneal route is chosen; BOA and NICE guidance stress explicit consent discussion of retrograde ejaculation risk in males. Registry data (NJR, AJRR, AOANJRR) show that L5–S1 ALIF is most commonly performed as part of a 360-degree fusion with posterior pedicle screw augmentation. In high-resource centres access surgeons are routine and cell salvage is standard; in resource-limited settings the same approach may be performed by the spine surgeon alone with careful attention to the three protection rules (blunt, midline, no monopolar). The biomechanical goal — a large lordotic cage at L5–S1 with posterior supplementation — is universal. Consent (globally applicable) must cover retrograde ejaculation (1–5 percent in males), vascular injury requiring repair or transfusion, ileus, adhesions, incisional hernia, infection, and the possibility of conversion to a retroperitoneal route or abandonment of the anterior stage.
Retrograde ejaculation after anterior interbody lumbar fusion
- Classic paper quantifying the risk of retrograde ejaculation after transperitoneal ALIF
- Demonstrated that the risk is higher with transperitoneal than retroperitoneal routes
- Identified monopolar diathermy use near the plexus as a major modifiable risk factor
Retrograde ejaculation after anterior lumbar interbody fusion with and without BMP-2
- 10-year cohort controlled study of retrograde ejaculation risk after L5–S1 ALIF
Prospective comparison of laparoscopic versus mini-ALIF for anterior L4-L5 fusion
- Prospective comparison showing the laparoscopic transperitoneal approach had longer operative time but similar fusion outcomes to mini-open
Open anterior approaches for lumbar spine procedures
- Described open anterior approaches including transperitoneal for L5–S1 access and the importance of vascular mobilisation