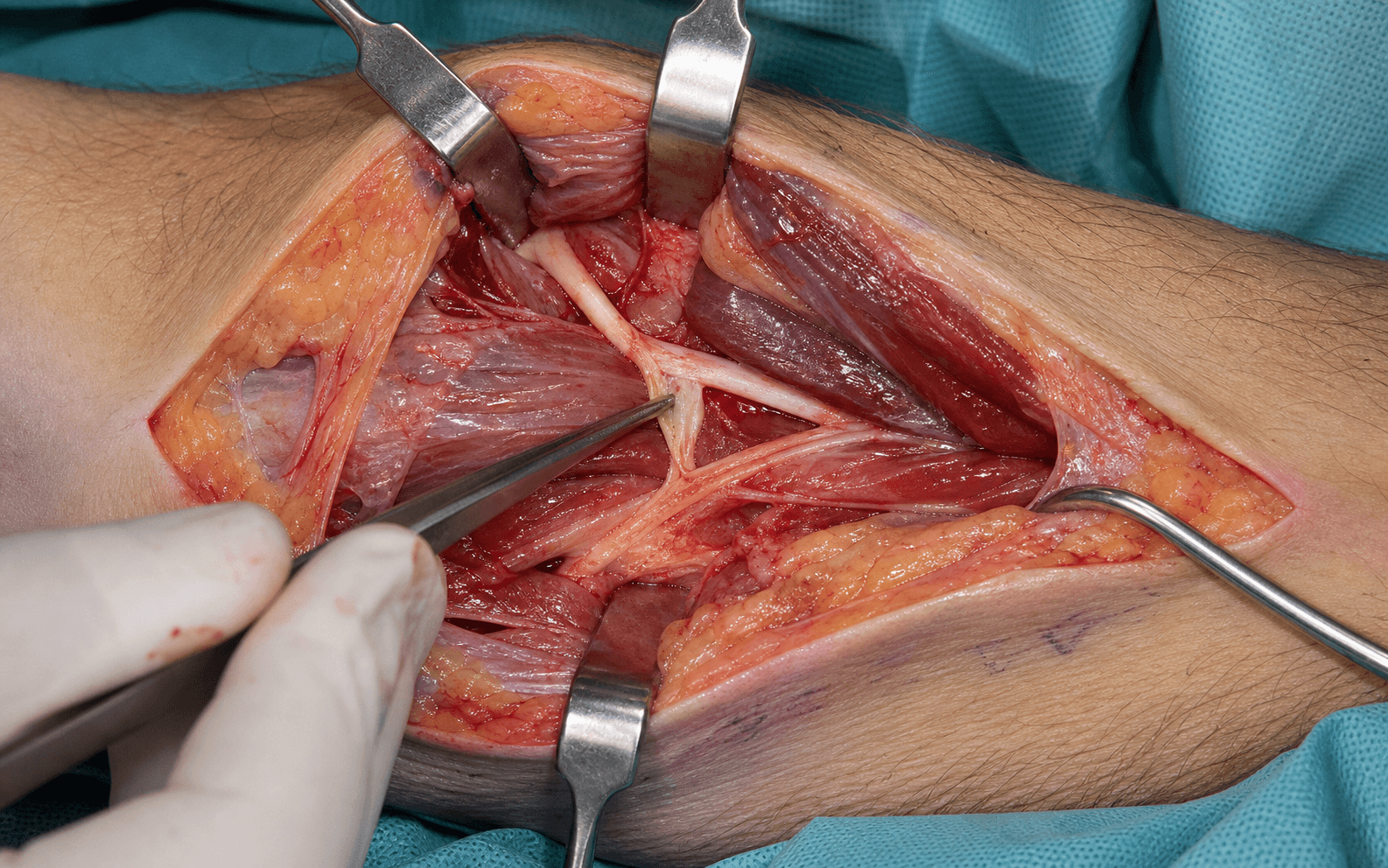
Volar approach to the median nerve and AIN in the proximal forearm, following the AIN as it dives deep toward the interosseous membrane
- AIN syndrome is a PURE motor weakness of FPL, FDP to the index and middle fingers, and pronator quadratus, with NO sensory loss — the OK sign test is pathognomonic (a flattened pinch instead of a round circle).
- Most idiopathic AIN palsies are now regarded as a neuritis (neuralgic amyotrophy / hourglass fascicular constriction) rather than a true entrapment, so most are observed for at least 6 to 12 months before surgery. The JAAOS consensus quotes a minimum of 12 months with no motor improvement before decompression, unless a mass is present or weakness is progressive.
- When operating, the dominant compression site is the FDS arch (50 to 70 percent); also search for a Gantzer's accessory FPL head (present in 45 to 65 percent of people) and a mass lesion.
- Decompression means releasing the FDS arch, excising a compressing Gantzer's, removing any mass, and external neurolysis only — AVOID internal neurolysis (opening the epineurium).
- Protect the medial antebrachial cutaneous nerve branches (the most common nerve injured in this approach) and the radial artery, which runs deep to FPL during distal exploration.
- “Pure motor, no sensory loss — differentiates AIN palsy from median nerve compression at pronator or carpal tunnel.
- “Recovery is proximal to distal: FPL first (3 to 6 months), FDP index next (4 to 8 months), pronator quadratus last (6 to 12 months); EMG at 3 months looks for reinnervation potentials.
- “Complete release of the FDS arch is essential — verify the AIN glides freely with pronation and supination after release.
When & Why
Indication. AIN syndrome — pure motor weakness of FPL, FDP to the index and middle fingers, and pronator quadratus, with no sensory loss, a flattened OK sign, and EMG showing denervation confined to FPL, FDP index-middle and pronator quadratus with normal sensory studies — in one of three settings: - No motor recovery after prolonged observation (commonly 6 to 12 months; the JAAOS consensus quotes a minimum of 12 months of no improvement for purely idiopathic or neuritic disease);
- Progressive weakness during observation; or
- A demonstrated compressive lesion on MRI — a ganglion, lipoma, schwannoma or aberrant vessel — or a traumatic injury with no recovery. The single most important step before offering surgery is to exclude neuralgic amyotrophy (Parsonage-Turner), which is now thought to account for most idiopathic AIN palsies and is managed by observation, not decompression.
Most idiopathic AIN palsies are a neuritis (neuralgic amyotrophy, hourglass fascicular constriction). Observe for at least 6 months and commonly up to 12 months. Recovery is frequent but often slow and incomplete, and routine early surgery has not been shown to help.
No recovery after prolonged observation, or progressive weakness. Release the FDS arch, excise a compressing Gantzer's muscle, and perform external neurolysis only — the standard volar operation laid out below.
MRI shows a discrete compressive lesion (ganglion, lipoma, tumour) or there is a traumatic injury. Earlier surgery is justified; remove the lesion while preserving the AIN.
Confirm the diagnosis before operating. The OK sign test is the bedside key (a flattened pinch from weak FPL and FDP index). Examine for isolated weakness of FPL, FDP index-middle and pronator quadratus, and crucially for any sensory loss — numbness means this is not isolated AIN palsy. EMG and nerve conduction studies confirm denervation in FPL, FDP index-middle and pronator quadratus with normal sensory studies. MRI of the forearm (T1, T2 fat-saturated and post-contrast) rules out a mass, and high-resolution imaging may show hourglass fascicular constriction. Plain radiographs exclude a fracture or bone lesion. Know the mimics. Pronator syndrome and carpal tunnel syndrome both carry sensory loss (AIN does not). C7 radiculopathy weakens triceps and FCR with radiating neck pain and a reduced triceps reflex. An FPL tendon rupture has full passive IP range and a normal EMG. Posterior interosseous nerve palsy affects the extensors, not the flexors. And neuralgic amyotrophy is heralded by acute severe shoulder and arm pain, often after a viral illness or vaccination. Setup. Supine, arm on an armboard, shoulder abducted 90 degrees, elbow extended, forearm supinated; upper-arm tourniquet to 250 mmHg. Loupe magnification (and a headlight for the deep distal work) is mandatory — identifying a 1.5 to 3 mm motor nerve among the forearm flexors is the whole operation.
The Operation
The goal is to expose the median nerve and AIN through a lazy-S volar approach, release every compression site (most often the FDS arch, then a Gantzer's muscle or a mass), confirm the nerve is mobile and well perfused, and avoid the cutaneous nerve and radial artery throughout. The exposure is laid out in full as the first steps below — finding and protecting the structures is the heart of the operation.
Operative sequence
- Supine, arm on an armboard, shoulder abducted 90 degrees, elbow extended, forearm supinated; upper-arm tourniquet to 250 mmHg.
- Loupe magnification and a headlight on from the start — nerve identification is the whole operation.
- Mark the antecubital fossa, the medial border of the mobile wad (brachioradialis) and a lazy-S incision from about 2 cm proximal to the elbow crease, running 8 to 12 cm distally along the radial border of FDS and FCR.
- A lazy-S (not linear) incision avoids a scar contracting the flexion crease, and can be extended proximally or distally as the pathology demands.
- Incise the skin and carefully develop the subcutaneous plane.
- Identify and protect the medial antebrachial cutaneous nerve branches — multiple fine branches cross the field throughout and are the single most common nerve injured in this approach.
- Ligate crossing veins (median cubital and basilic branches) with care, away from the cutaneous nerve branches.
- Incise the antebrachial fascia longitudinally.
- Find the brachial artery first — it is pulsatile and the reliable landmark; the median nerve lies immediately medial to it.
- Place a vessel loop around the proximal median nerve. Release the lacertus fibrosus (bicipital aponeurosis) if present, and separate the two heads of pronator teres if the nerve passes between them — the same proximal moves as a pronator syndrome release.
- The aim is a cleanly identified, mobile median nerve so the AIN branch point can be found.
- Follow the median nerve distally from the antecubital fossa.
- The AIN branches 4 to 8 cm distal to the lateral epicondyle (range 2 to 10 cm — highly variable), diving posteriorly away from the main trunk toward the interosseous membrane.
- It is smaller than the median nerve (1.5 to 3 mm). Its direction — diving deep and posterior — is the key to recognising it.
- The anterior interosseous artery accompanies it and is often easier to see first; find the pulsatile artery and the AIN lies alongside. Mark the AIN with a vessel loop.
- Follow the AIN distally as it dives deep beneath the flexor digitorum superficialis arch — a fibrous arch at the FDS origin from the radius, about 4 to 5 cm distal to the elbow.
- This is the most common compression site (50 to 70 percent). Divide the arch completely and longitudinally, lifting it away from the nerve.
- After release the AIN must be freely mobile. If it is tight or indurated from chronic compression, a gentle external neurolysis may help.
- Do not perform aggressive internal neurolysis (opening the epineurium) — see Step 8.
- Look for Gantzer's muscle (an accessory head of FPL), present in 45 to 65 percent of people, arising from the medial epicondyle or coronoid process and crossing the AIN to reach the FPL tendon; it compresses the nerve in roughly 30 to 40 percent of those who have it.
- If present and compressing, excise the muscle belly at its origin and insertion (bipolar haemostasis first — it is vascular), preserving the FPL tendon and main muscle belly.
- Inspect for a mass lesion — ganglion (most common), lipoma, schwannoma or aberrant vessel — and excise it carefully, identifying the AIN proximal and distal to the mass and protecting it with vessel loops. Send any mass for histology.
- If proximal release is inadequate or distal pathology is suspected, extend the exploration distally.
- Follow the AIN deep between FPL (retracted radially) and FDP (retracted ulnarly), running on the anterior surface of the interosseous membrane.
- The radial artery lies deep to FPL — palpate the radial pulse before and after retraction and stay on the interosseous membrane to avoid it.
- Trace distally toward pronator quadratus, releasing any further fascial bands, and identify the motor branches to FDP (index and middle) and to pronator quadratus.
- Assess the decompressed AIN. A healthy nerve is pink, soft and mobile with a visible fascicular pattern; an unhealthy nerve is pale or dusky, indurated, scarred and tethered.
- If the nerve is encased in scar, perform external neurolysis — freeing it from surrounding scar with microscissors in the plane between epineurium and tissue. This is safe and often helpful.
- Avoid internal neurolysis (opening the epineurium and separating fascicles) — it risks devascularising the fascicles and has no evidence of benefit; most nerve surgeons avoid it.
- For a neuroma-in-continuity or complete division (rare in AIN syndrome, more so in trauma), nerve action potential testing guides whether to observe or to resect and graft.
- Confirm every compression site is released: FDS arch fully divided, Gantzer's or other anomalous muscle excised, any mass removed, no kinking along the course.
- Pronate and supinate the forearm — the AIN should glide smoothly without catching.
- The nerve should be mobile from origin to distal branches, and pink and well perfused.
- If the release was extensive you may close the deep fascia loosely to maintain anatomy, but it must not be tight (which recreates compression); some surgeons leave it open after extensive neurolysis.
- Release the tourniquet and achieve meticulous haemostasis, controlling anterior interosseous artery branches. Irrigate thoroughly.
- Close in layers; deep fascia, if closed, must be loose with no compression. Subcutaneous 3-0 absorbable, then skin with nylon or a subcuticular suture.
- Do not place a drain — drains risk adhesions and nerve injury in nerve surgery.
- Apply a bulky dressing with the forearm in neutral; a posterior splint for comfort is optional and removed at 3 to 7 days to begin early motion.
The medial antebrachial cutaneous nerve branches are the most frequently injured structure in this volar approach — identify and protect every branch in the subcutaneous plane, using skin hooks rather than forceps on the skin edges and avoiding electrocautery near them. The radial artery runs deep to FPL in the mid and distal forearm and is vulnerable when you retract FPL for distal AIN exploration: palpate the pulse before and after retraction, stay on the interosseous membrane, and consider marking the artery with Doppler preoperatively if the distal course is uncertain. If injured, control with direct pressure and repair primarily, confirming ulnar inflow first.
When the AIN origin is hard to identify, find the anterior interosseous artery first — it is pulsatile and runs with the AIN throughout its course, and the nerve lies alongside. Start proximally from the brachial artery (the median nerve is medial to it) and work distally, never dissecting blindly in the depths.
Freeing the AIN from surrounding scar (external neurolysis) is safe and often beneficial. Opening the epineurium to separate individual fascicles (internal neurolysis) is controversial, risks devascularising the nerve, has no evidence of benefit, and is avoided by most peripheral nerve surgeons.
Aftercare & Complications
Rehabilitation | Phase | Timing | Splint and activity | Therapy focus | |-------|--------|---------------------|---------------| | 1 | 0 to 1 week | Posterior splint for comfort (removed at 3 to 7 days); bulky dressing, fingers free | Elevation, ice, oedema control | | 2 | 1 to 3 weeks | Splint off; light activities of daily living | Gentle active ROM — pronation/supination, wrist, fingers, thumb; passive FPL and FDP stretch | | 3 | 3 to 6 weeks | Light activities | Progressive strengthening — putty, grip, pinch; scar massage from 10 to 14 days | | 4 | 3 to 6 months | Full activity as tolerated | Strengthening; expect gradual motor return | | 5 | 6 to 18 months | Full | Monitor recovery; consider salvage if plateaued | Recovery timeline. Reinnervation proceeds proximal to distal: FPL recovers first (3 to 6 months), then FDP to the index (4 to 8 months), then pronator quadratus last (6 to 12 months). EMG at 3 months looks for reinnervation potentials, a favourable sign. Most recovery is complete by 12 months, with little gain beyond 18 months.
- Recognition
- OK sign still abnormal at 12 to 18 months; EMG shows no reinnervation
- Prevention
- Appropriate selection (avoid neuritis); operate before chronic axonal loss; complete decompression; honest counselling
- Management
- Observe to 18 months for late return; consider salvage tendon transfers (BR to FPL, ECRL to FDP index) or thumb IP arthrodesis
- Recognition
- Numbness, dysesthesia or a tender Tinel over the medial forearm
- Prevention
- Careful subcutaneous dissection; identify and preserve every branch; skin hooks not forceps
- Management
- Usually settles; desensitisation, topical lidocaine, gabapentin; rare neuroma excision
- Recognition
- New median sensory loss and thenar weakness; Tinel sign at the injury
- Prevention
- Loupes; vessel loops for gentle retraction; sharp dissection under direct vision
- Management
- Intraoperative primary repair if clean division; postoperative EMG and explore if complete
- Recognition
- Bright pulsatile bleeding when retracting FPL; loss of radial pulse
- Prevention
- Gentle FPL retraction; palpate the pulse; stay on the interosseous membrane
- Management
- Direct pressure; primary repair (6-0 or 7-0); confirm ulnar inflow first
- Recognition
- Initial improvement then return of weakness at 3 to 6 months
- Prevention
- Complete initial release; loose fascial closure; early mobilisation
- Management
- MRI to localise; revision decompression with realistic expectations (lower success)
- Recognition
- Increasing pain, tense swelling, expanding forearm girth
- Prevention
- Meticulous haemostasis on tourniquet release; no drains; bulky dressing
- Management
- Small — observe and elevate; large or expanding — return to theatre for evacuation
- Recognition
- Disproportionate pain, stiffness, shiny or mottled skin, allodynia
- Prevention
- Early mobilisation; adequate analgesia; vitamin C may reduce risk
- Management
- Early — hand therapy, desensitisation, gabapentin; stellate ganglion block if severe
- Recognition
- Limited ROM versus the contralateral side
- Prevention
- Early ROM from 3 to 7 days; hand therapy referral
- Management
- Aggressive therapy; dynamic splinting; rare adhesiolysis if refractory
Realistic expectations. Neuralgic amyotrophy often recovers spontaneously but slowly and frequently incompletely, and routine early surgery has not been shown to help. A discrete compressive lesion released before chronic axonal loss has the best prognosis. Longer symptom duration means progressively poorer and often incomplete recovery. Precise percentage outcomes cannot be promised — the literature is small and heterogeneous — so honest counselling over many months is essential.
Viva & Exam Focus
FIG PIEFIG PIE — the AIN syndrome triad
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old carpenter presents with 4 months of thumb and index finger weakness. He cannot pinch properly. How do you assess and diagnose this patient?”
“You are performing an AIN decompression. After releasing the FDS arch and excising Gantzer's muscle, the nerve still appears pale and indurated. What do you do? What is the controversy regarding neurolysis?”
“What conditions mimic AIN syndrome, and how do you differentiate them clinically and with investigations?”
Indications
- No recovery after 6 to 12 months of observation (12 months for idiopathic or neuritic disease)
- Progressive weakness despite conservative management
- Space-occupying lesion on MRI (ganglion, lipoma, tumour)
- Traumatic AIN injury with no recovery
- Exclude neuralgic amyotrophy — observe, surgery not beneficial
Key anatomy
- AIN is a pure motor branch of the median nerve, branching 4 to 8 cm distal to the lateral epicondyle (range 2 to 10 cm)
- Dives posteriorly between FPL and FDP to the interosseous membrane
- Supplies FPL, FDP to index and middle, and pronator quadratus
- Runs with the anterior interosseous artery; radial artery lies deep to FPL (danger)
Compression sites
- FDS arch (most common, 50 to 70 percent)
- Gantzer's accessory FPL head (present in 45 to 65 percent)
- Mass lesion (10 to 15 percent — ganglion most common)
- Fibrous bands; and neuritis (Parsonage-Turner) for most idiopathic cases
Critical steps
- Lazy-S volar incision 8 to 12 cm, protect medial antebrachial cutaneous branches
- Find the brachial artery — median nerve lies medial to it
- Identify the AIN branch point, mark with a vessel loop
- Release the FDS arch completely; excise a compressing Gantzer's (preserve the FPL tendon)
- External neurolysis only — never internal; verify with pronation and supination
- No drains; loose fascial closure
Danger zones
- Medial antebrachial cutaneous nerve — the commonest injury
- Brachial artery and bifurcation
- Radial artery deep to FPL in the distal forearm
- The AIN itself — small calibre, use loupes
- Motor branches to FPL, FDP index-middle and PQ
Recovery and salvage
- Proximal to distal: FPL 3 to 6 months, FDP index 4 to 8 months, PQ 6 to 12 months
- Plateau by 18 months
- Salvage: BR to FPL, ECRL to FDP index, thumb IP arthrodesis
- Observe 6 to 12 months (12 for idiopathic) before surgery
Background & Evidence
Why an AIN palsy happens. AIN syndrome is no longer seen as a simple entrapment. Three broad mechanisms overlap: - Neuritic or spontaneous — now thought to account for most idiopathic cases. Neuralgic amyotrophy (Parsonage-Turner) is an immune-mediated brachial plexopathy that preferentially involves AIN fascicles, often after a viral illness, surgery or vaccination, and high-resolution imaging not infrequently shows hourglass fascicular constriction or torsion within the median nerve trunk.
- Compressive — a structural lesion at a defined site (the FDS arch, a Gantzer accessory head, a fibrous band) or a space-occupying lesion (ganglion, lipoma, schwannoma, thrombosed vessel).
- Traumatic — forearm fractures (both-bone, Monteggia), elbow dislocation, penetrating injury, compartment syndrome, or iatrogenic injury from plating or vascular access.
- Frequency and notes
- Most common structural site (50 to 70 percent); fibrous arch at the FDS origin, 4 to 5 cm distal to the elbow
- Implication for surgery
- Release the arch completely and longitudinally
- Frequency and notes
- Present in 45 to 65 percent; compresses the AIN in 30 to 40 percent of those who have it
- Implication for surgery
- Excise the muscle belly, preserve the FPL tendon
- Frequency and notes
- 10 to 15 percent — ganglion most common, then lipoma, schwannoma, aberrant vessel
- Implication for surgery
- Excise earlier, preserving the AIN; send for histology
- Frequency and notes
- Thickened fascia or aberrant fascial condensations
- Implication for surgery
- Divide during systematic exploration
- Frequency and notes
- Thought to account for most idiopathic cases
- Implication for surgery
- Observe — surgery is generally not beneficial
Recovery potential. Recovery depends chiefly on mechanism and duration. The figures below are approximate and directional, drawn from small case series:
- Typical recovery
- About 80 percent full recovery
- Features
- Neuralgic amyotrophy with an improving trend; release within 3 months; young patient; isolated site; early reinnervation on EMG
- Typical recovery
- About 50 to 60 percent significant recovery
- Features
- Chronic compression of 3 to 12 months; multiple sites; middle-aged with comorbidity; no reinnervation on EMG at 3 months
- Typical recovery
- About 30 percent recovery
- Features
- Chronic compression over 12 to 18 months; complete division needing repair or graft; elderly or diabetic; complete denervation with no motor units
References
Pronator syndrome and anterior interosseous nerve syndrome
- AIN syndrome is a pure motor palsy of any or all of FPL, FDP to the index and middle, and pronator quadratus, with normal sensory studies.
- AIN syndrome is increasingly regarded as a neuritis that frequently resolves spontaneously after prolonged observation.
- The stated surgical indication is a minimum of 12 months with no signs of motor improvement (versus greater than 6 months of persistent symptoms for pronator syndrome).
Anterior interosseous nerve palsy. A review of 16 cases
- 16 patients (19 limbs) reviewed at a mean of 6.4 years; a high incidence of incomplete lesions and of associated neurological lesions in the same or opposite limb.
- A discrete compressive cause or visible AIN change was found in only 3 of 8 explored limbs.
- Conservatively treated and surgically explored patients showed no difference in onset, time to, or extent of recovery; incomplete lesions recovered well regardless of treatment.
The clinical spectrum of neuralgic amyotrophy in 246 cases
- Prospective study of 246 neuralgic amyotrophy patients (199 idiopathic, 47 hereditary); the brachial plexus is affected in a patchy fashion and the AIN is a recognised target.
- Recovery was less favourable than usually assumed, with persisting pain and/or paresis in approximately two-thirds of patients followed for 3 years or more.
- Recurrent attacks occurred in about a quarter of idiopathic cases over a mean 6-year follow-up.
Anterior interosseous nerve lesions. Clinical and electrophysiological features
- Consecutive series of 13 patients referred for electrodiagnosis; only 3 had a correct initial clinical diagnosis and 3 were mislabelled as tendon ruptures.
- All patients showed electrophysiological abnormalities, most commonly involving the pronator quadratus.
- Late spontaneous recovery was common and only one patient underwent surgical exploration.
The anterior interosseous-nerve syndrome, with special attention to its variations
- Classic anatomic and clinical description defining the syndrome and its variations.
- Identified the principal compression sites including the FDS arch, the Gantzer accessory head of FPL, and aberrant fibrous bands.
- Established the surgical principles for decompression when a structural lesion is present.
Spontaneous anterior interosseous nerve palsy with hourglass-like fascicular constriction within the main trunk of the median nerve
- Interfascicular neurolysis revealed hourglass-like fascicular constrictions in 8 of 9 patients with spontaneous AIN palsy.
- Supports a neuritic and constrictive mechanism rather than a purely entrapment aetiology for idiopathic disease.