L4-5 and L5-S1 access · retroperitoneal dissection · superior hypogastric plexus at risk
- The anterior retroperitoneal approach gives direct access to the L4-5 and L5-S1 disc spaces for ALIF, mobilising the great vessels to release the anterior longitudinal ligament and seat a large lordotic interbody graft with wide endplate contact. Favourable fusion biology gives circumferential fusion a 92% union rate versus 80% for posterolateral fusion (Christensen 2002).
- At L5-S1 the left common iliac vein is the single most vulnerable structure — thin-walled, crossing the disc, and giving off the ascending lumbar (iliolumbar) vein that avulses during mobilisation. It is the commonest source of significant bleeding in anterior lumbar surgery (Inamasu 2006).
- Ligate the ascending lumbar (iliolumbar) vein BEFORE mobilising the main vein, then mobilise gently with a soft retractor released every 15-20 minutes. If the main vein is injured: direct pressure first, then primary repair with 5-0 Prolene — NEVER ligate the main left common iliac vein (causes venous congestion, leg swelling and DVT).
- The superior hypogastric plexus is a diffuse midline pre-sacral sympathetic plexus over the L5-S1 disc and sacral promontory controlling emission/ejaculation. Its injury causes retrograde ejaculation in 0.5-5% of males, generally permanent and worst with a transperitoneal or bilateral midline dissection (Tiusanen 1995). Prevent it with a retroperitoneal approach, a blunt midline sweep to one side, and bipolar (not monopolar) cautery.
- Approach by level: L4-5 is typically approached LEFT retroperitoneally (aorta and left common iliac artery mobilised medially, IVC stays right); L5-S1 is reached through a MIDLINE pre-sacral window between the iliac vessels, below the iliocaval confluence.
When & Why
What it exposes. The anterior retroperitoneal approach gives direct access to the L4-5 and L5-S1 disc spaces for anterior lumbar interbody fusion (ALIF), total disc replacement, vertebral body procedures and anterior release for deformity. The dissection stays retroperitoneal (NOT transperitoneal — the bowel remains within the peritoneal sac), and the great vessels (aorta, IVC, common iliac vessels) are mobilised to expose the anterior longitudinal ligament (ALL) and disc space. Why anterior (the fusion biology). Anterior interbody support offers three biomechanical advantages over posterior interbody techniques (PLIF/TLIF): (1) a large lordotic graft with wide endplate contact — the disc is cleared end-to-end and a footprint-maximising cage seated, with ALL release allowing powerful segmental lordosis restoration; (2) compression loading — the anterior column carries roughly 80% of axial load, so an anteriorly placed graft is loaded in compression (favourable for healing); and (3) a preserved posterior tension band — the posterior longitudinal ligament (PLL), facets and paraspinal musculature stay intact. A randomised trial found that adding an ALIF cage to posterior fixation (circumferential fusion) improved union (92% vs 80%) and cut reoperation (7% vs 22%) versus instrumented posterolateral fusion alone (Christensen 2002). Approach by level. The level dictates the corridor. At L4-5 the aorta lies left and the IVC right; the standard approach is left retroperitoneal, mobilising the aorta and left common iliac artery medially while the IVC stays out of field. At L5-S1 the aorta and IVC have already divided, so the disc is reached through a midline pre-sacral window between the common iliac vessels, below the bifurcation and iliocaval confluence. Indications. Single- or two-level degenerative disc disease with mechanical low back pain, painful degenerative discs with preserved motion, low-grade spondylolisthesis, recurrent disc herniation with mechanical pain, and deformity requiring anterior release and lordosis restoration. Higher levels (L2-3, L3-4) are rarely approached anteriorly because the aorta and IVC are more midline and harder to mobilise, and the sympathetic chain (causing bowel dysmotility if injured) runs along the anterolateral bodies. Contraindications. Prior left retroperitoneal surgery (scarring obscures planes), prior left nephrectomy or left kidney pathology (difficult retroperitoneal mobilisation), and abdominal aortic aneurysm (vascular surgery required first). Relative: severe osteoporosis (high subsidence risk for a stand-alone construct — add posterior fixation). Global practice, guidelines and registries. ALIF is widely used for single-level degenerative L4-5 and L5-S1 disease across advanced orthopaedic practice and advanced orthopaedic practice practice, with registry and database trends showing growth of anterior and lateral interbody techniques. Exposure is performed either with a dedicated access (vascular or general) co-surgeon — the traditional model for supine retroperitoneal ALIF — or by the spine surgeon alone, increasingly so for oblique/lateral L5-S1 (OLIF51) provided meticulous attention is paid to left common iliac vein anatomy (Barber 2024). Standard workup is lumbar MRI, standing flexion/extension radiographs, non-contrast CT (bone quality and vascular anatomy/iliocaval confluence) and DEXA where bone-density risk is suspected (Barber 2024). Pre-operative counselling about retrograde ejaculation and infertility is a mandatory consent standard for male patients in every jurisdiction; sperm banking should be offered to young men. Chemical VTE prophylaxis with low-molecular-weight heparin plus early mobilisation is standard peri-operatively.
The Exposure
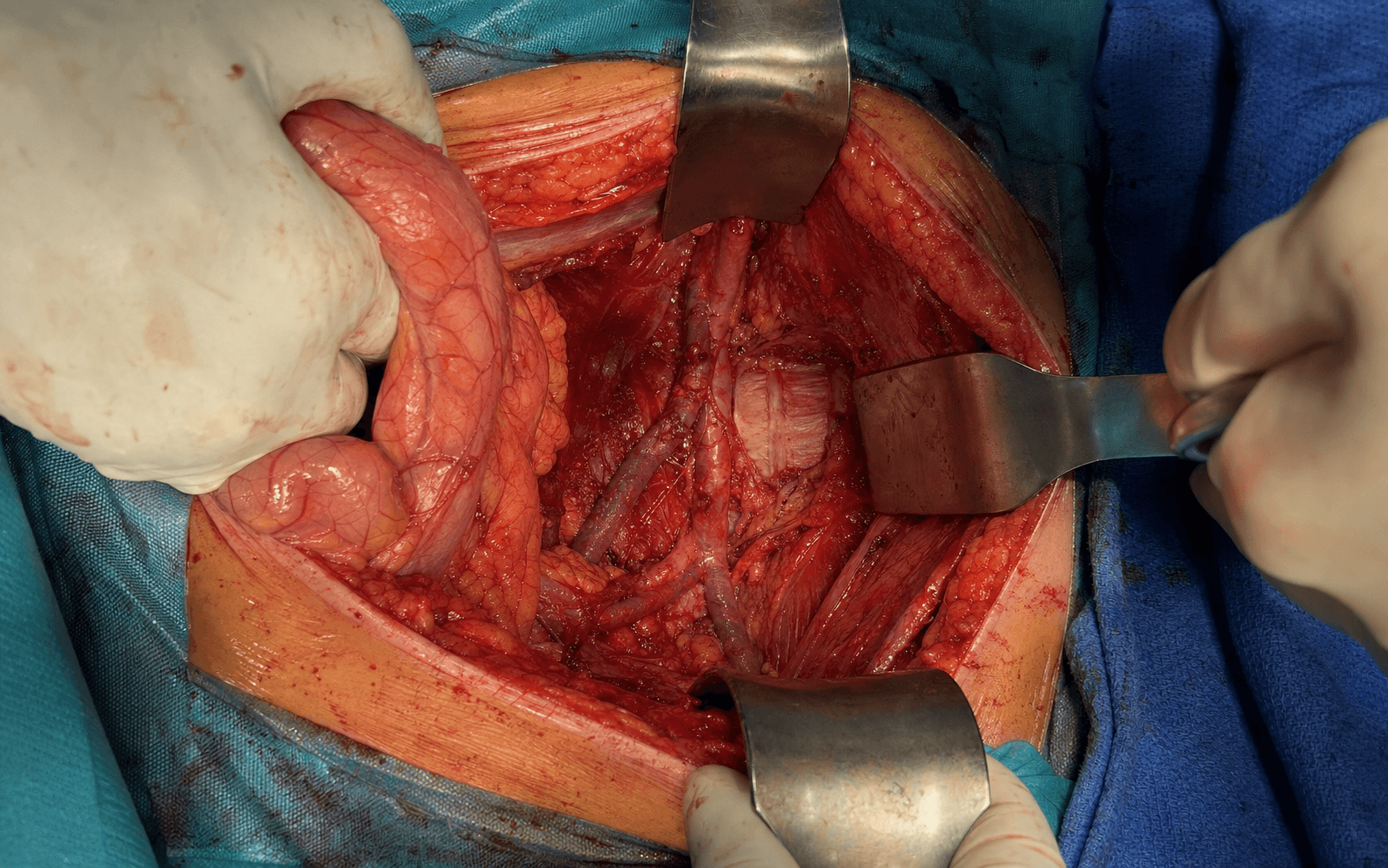
The heart of the approach is a controlled retroperitoneal dissection that develops a working plane between the peritoneum (anterior) and the psoas (posterior), then mobilises the great vessels to expose the disc — differently at L4-5 (left-sided, aorta mobilised medially) and L5-S1 (midline window between the iliac vessels, left common iliac vein defined and protected).
Exposure sequence
- Position: supine with the left side elevated 15-20 degrees (or true right lateral decubitus, gravity assisting peritoneal mobilisation); arms on boards or across the chest; fluoroscopy set for AP and lateral lumbar views. General anaesthesia (the patient must be completely still for vascular dissection) with a urinary catheter to monitor output and decompress the bladder.
- Incision for L4-5: palpate the LEFT anterior superior iliac spine (ASIS); an 8-12 cm oblique incision from 2-3 cm medial to the ASIS curving toward the umbilicus, placed 2-3 cm above the inguinal ligament. For L5-S1 a lower transverse (Pfannenstiel-type) or oblique suprapubic incision gives access below the bifurcation.
- Incise skin and subcutaneous tissue down to external oblique fascia; split it in line with its fibres (parallel to the inguinal ligament). Deep to it, split internal oblique and transversus abdominis BLUNTLY in line with their fibres — this avoids denervating them (the iliohypogastric and ilioinguinal nerves run within these muscles; injury causes groin numbness).
- Identify the glistening peritoneum and use blunt (finger or sponge-stick) dissection to mobilise it ANTERIORLY and MEDIALY, creating the retroperitoneal pocket between peritoneum (anterior) and psoas (posterior). Do NOT violate the peritoneum — transperitoneal dissection is the wrong plane (exposes bowel, risks bowel injury, and at L5-S1 raises retrograde ejaculation risk). If opened, close it with 3-0 absorbable suture and continue retroperitoneally.
- Continue blunt mobilisation of the peritoneum anteriorly and medially. Palpate the psoas muscle posteriorly (firm longitudinal fibres along the left side of the spine) — the lateral border of exposure. The ureter runs within the peritoneal reflection (palpate as a peristaltic cord); keep it within the peritoneal sac so it mobilises anteriorly with the peritoneum.
- Identify the medial landmarks by palpation: the pulsatile iliac artery, the softer iliac vein, and the anterior lumbar vertebral bodies. Place a self-retaining retractor (e.g. Omni-Tract, Bookwalter) to hold the peritoneum anteriorly and maintain the retroperitoneal exposure.
- L4-5 (left-sided, standard): the aorta bifurcates into the common iliac arteries at L4 (variable, L3-L5 in 10-15%). Clear loose areolar tissue off the aorta and left common iliac artery, identify the small ascending lumbar (iliolumbar) veins ascending along the left vertebral body, and LIGATE them before mobilising (vascular clips or fine ties — this prevents the avulsion that is the commonest bleeding event). Then retract the aorta/left iliac artery MEDIALLY with a handheld malleable or Deaver retractor (assistant-held — never a self-retaining blade on the aorta) to expose the L4-5 disc.
- L5-S1 (midline pre-sacral window): work down to the bifurcation and develop the corridor between the common iliac vessels. The left common iliac vein crosses the disc obliquely as it ascends to the right to form the IVC — define it FIRST, ligate its ascending lumbar (iliolumbar) tributary before any mobilisation, then sweep the vein gently (usually to the left) with a soft vein retractor. An unfavourably low iliocaval confluence or scarring favours a lateral/oblique (OLIF51) corridor or an access co-surgeon (Barber 2024).
- Over the L5-S1 disc and sacral promontory, use BLUNT midline dissection only and sweep the pre-sacral soft tissue (with the plexus) to one side as a single intact layer. Avoid monopolar cautery — use bipolar or blunt technique to protect the diffuse sympathetic fibres controlling ejaculation.
- The middle sacral artery and vein run in the midline over the promontory — coagulate or ligate them to clear the midline disc face.
- Place a radiopaque marker on the anterior disc and obtain lateral and AP fluoroscopy. Count vertebrae from L5 (the most caudal lumbar vertebra with a disc before the sacrum) upward to confirm the level, and confirm midline positioning of the marker.
- Wrong-level surgery is a NEVER EVENT and a medicolegal catastrophe — ALWAYS confirm the level fluoroscopically before discectomy.
- Make a vertical incision through the ALL over the disc (full height, superior to inferior endplate); the ALL is vascular, so cauterise bleeding from it and the anterior annulus. Place blunt retractors (e.g. Cloward) on the endplates above and below to define the disc boundaries.
- With pituitary rongeurs, curettes and angled instruments, remove ALL disc material — nucleus then annulus, circumferentially — down to bleeding cancellous endplate. Preserve the PLL (the posterior boundary separating disc from thecal sac); confirm it is intact by palpating the posterior disc with a nerve hook (smooth ligament, not pulsatile dura). Violating the PLL causes CSF leak and nerve root injury.
- Using curettes or endplate scrapers, remove the thin cartilaginous endplate (0.5-1 mm) from both endplates to expose bleeding cancellous bone — necessary for graft incorporation.
- Preserve the dense subchondral bone beneath it — this is the structural support for the cage. Over-aggressive preparation that breaches the subchondral plate predisposes to subsidence (cage migration into soft cancellous bone, around 10-12% of stand-alone fusions — Tempel 2017).
- Measure disc height and AP depth with trial spacers. Target a height that restores pre-degenerative disc height (typically 10-12 mm at L4-5; the L4-5 disc is larger than L5-S1), a maximum safe AP depth of 25-30 mm (about 75-80% of vertebral body AP diameter — never more than 30 mm, which risks posterior migration), and 6-10 degrees of lordosis.
- Pack the cage cavity with graft (iliac-crest autograft, allograft chips, or bone graft substitute/BMP). Insert under continuous lateral fluoroscopy to a depth of typically 25-28 mm, then confirm a central, endplate-parallel position on AP and lateral views. Under-sizing causes pseudarthrosis (no compression across the graft); over-sizing causes subsidence — a trial that needs FIRM impaction is the goal.
- Confirm haemostasis (ascending lumbar veins, anterior annulus, ALL), remove all vascular retractors and let the vessels return to anatomical position. Do NOT attempt to close the peritoneum (it heals spontaneously); just ensure it is intact.
- Close transversus abdominis, internal oblique and external oblique fascia in layers with 0 or #1 absorbable suture (Vicryl or PDS), close subcutaneous tissue with 2-0 absorbable to obliterate dead space, and close skin with subcuticular monocryl or staples. A drain is usually NOT needed (the retroperitoneal space is not closed and fluid is absorbed by the peritoneum).
- A stand-alone construct is supplemented with an LSO (lumbosacral orthosis) brace for 6-12 weeks; supplemental posterior fixation (a second-stage prone percutaneous pedicle-screw construct) is added for poor bone quality, multilevel fusion, or instability, and then a brace is not required.
The left common iliac vein is the single most vulnerable structure in anterior lumbar surgery and the commonest source of significant haemorrhage (Inamasu 2006). It crosses the L5-S1 disc obliquely, lying directly on the anterior disc with minimal overlying tissue, thin-walled and easily torn. The three injury patterns are: (1) AVULSION of the ascending lumbar (iliolumbar) tributary during mobilisation — the commonest, causing brisk venous bleeding; (2) LACERATION of the main vein during disc access, mobilisation or cage insertion; and (3) THROMBOSIS (delayed, 2-7 days post-op, presenting with left-leg swelling). PROTECTION: define the vein early and mark it with a vessel loop; LIGATE the ascending lumbar (iliolumbar) vein BEFORE mobilising the main vein; mobilise gently with a soft handheld retractor (never a self-retaining blade applying point pressure) released every 15-20 minutes; and keep dissection sub-ligamentous on bone. IF INJURED: direct pressure first (5-10 minutes while vascular instruments are obtained), then PRIMARY REPAIR with 5-0 or 6-0 Prolene. NEVER ligate the main left common iliac vein — it causes venous congestion, leg swelling and DVT and must be reconstructed. Have an access/vascular surgeon, vascular instruments (DeBakey, vascular clamps, 5-0 Prolene), and typed/screened blood available, and a plan to extend to laparotomy if retroperitoneal control fails.
The superior hypogastric plexus is a diffuse midline pre-sacral sympathetic plexus over the lower L5 body, L5-S1 disc and sacral promontory that controls emission/ejaculation (sympathetic stimulation closes the bladder neck and contracts the seminal vesicles so semen passes antegrade). Injury causes retrograde ejaculation in 0.5-5% of males and is generally PERMANENT (sympathetic nerves do not reliably regenerate); orgasm sensation is preserved but there is no antegrade ejaculate, causing infertility. The strongest association is with a TRANSPERITONEAL approach — in Tiusanen's series every patient with permanent retrograde ejaculation had been operated transabdominally (Tiusanen 1995). PREVENT: use a RETROPERITONEAL (not transperitoneal) approach in males; use BLUNT midline dissection, sweeping the pre-sacral tissue to ONE side as a single intact layer rather than stripping both sides; AVOID monopolar cautery over the disc (bipolar or blunt only); and limit pre-sacral stripping to what is needed to seat the cage. MANDATORY CONSENT: counsel every male patient pre-operatively about retrograde ejaculation and infertility (a medicolegal standard worldwide) and offer sperm banking to young men.
Whatever the level, release vascular retraction every 15-20 minutes and periodically palpate distal pulses (dorsalis pedis, posterior tibial) to confirm lower-limb perfusion. Sustained retraction risks both ischaemia and intimal injury leading to delayed left common iliac vein thrombosis (2-7 days post-op).
Dangers & Extensions
Structures at risk, by layer and level
- Structure at risk
- Left common iliac vein — thin-walled, crosses the disc; ascending lumbar (iliolumbar) vein avulses on mobilisation
- Protection
- Define early and loop it; LIGATE the ascending lumbar vein before mobilising; soft retractor released every 15-20 min; primary repair if injured — NEVER ligate the main vein
- Structure at risk
- Aorta and left common iliac artery; the small ascending lumbar veins
- Protection
- Left-sided approach; mobilise the aorta/artery medially; ligate ascending lumbar veins first; stay sub-periosteal on bone
- Structure at risk
- Superior hypogastric plexus — retrograde ejaculation in 0.5-5% of males
- Protection
- Retroperitoneal (not transperitoneal) approach; blunt midline sweep to one side; bipolar (not monopolar) cautery
- Structure at risk
- Iliohypogastric and ilioinguinal nerves (groin numbness)
- Protection
- Split internal oblique and transversus bluntly in line with their fibres
- Structure at risk
- Psoas and lumbar plexus (genitofemoral nerve on the psoas surface)
- Protection
- Stay medial to the psoas; do not enter the muscle body
- Structure at risk
- Ureter (crosses the iliac vessels at the bifurcation)
- Protection
- Keep it within the peritoneal sac; mobilise anteriorly with the peritoneum; maintain the retroperitoneal plane
L4-5 vs L5-S1 — the corridor and the key vessel differ by level
- L4-5
- Left retroperitoneal; aorta/left iliac artery mobilised medially, IVC stays right
- L5-S1
- Midline pre-sacral window between the common iliac vessels, below the bifurcation
- Key point
- The bifurcation level (usually L4) sets the corridor
- L4-5
- Aorta / left iliac artery and the ascending lumbar vein
- L5-S1
- Left common iliac VEIN crossing the disc (thin-walled, fragile)
- Key point
- Define and protect the left common iliac vein at L5-S1
- L4-5
- Ligate before mobilising the aorta/iliac vessels
- L5-S1
- Ligate before mobilising the left common iliac vein
- Key point
- Commonest avulsion site — ligate it early at BOTH levels
- L4-5
- Less exposed (condenses lower, over L5-S1)
- L5-S1
- Directly in the field — blunt midline sweep, bipolar only
- Key point
- Retrograde ejaculation risk is concentrated at L5-S1
- L4-5
- Usually not encountered
- L5-S1
- Run in the midline over the promontory — coagulate/ligate
- Key point
- Control before midline disc work at L5-S1
- L4-5
- Oblique left lower-abdominal incision toward the umbilicus
- L5-S1
- Lower transverse (Pfannenstiel-type) or oblique suprapubic incision
- Key point
- Place the incision over the target level
Extensile options. Extend proximally along the retroperitoneal plane to reach L3-4 or L2-3 (increasingly difficult as the aorta/IVC become more midline and the sympathetic chain lies on the bodies). Extend distally below L5-S1 only when necessary (the common iliac vessels divide into external and internal branches at the pelvic brim, and the ureter crosses here). Where the L5-S1 iliocaval confluence is unfavourably low or scarred, convert to a lateral/oblique (OLIF51) corridor or involve an access co-surgeon rather than forcing a high-risk midline window (Barber 2024). Complications by timing
- Complication (rate)
- Vascular injury 2-5% (left common iliac vein commonest — Inamasu 2006)
- Management
- Direct pressure first; primary venous repair with 5-0/6-0 Prolene; NEVER ligate the main vein; call access/vascular surgery for arterial injury
- Complication (rate)
- Bowel injury (rare, less than 1%)
- Management
- Two-layer enterotomy repair (mucosa then serosa); general surgery consult; if unrecognised, presents as peritonitis needing laparotomy
- Complication (rate)
- Ureteral injury (rare, less than 0.5%)
- Management
- Urology urgently; retrograde/antegrade stenting; early primary repair; nephrectomy if delayed with severe hydronephrosis
- Complication (rate)
- Ileus 10-15%
- Management
- Conservative: NPO, IV fluids, NG tube if vomiting, ambulation, minimise opioids; resolves 2-4 days
- Complication (rate)
- Retrograde ejaculation 0.5-5% of males (permanent — Tiusanen 1995)
- Management
- No restorative treatment; counsel on permanence; fertility via bladder sperm retrieval after urinary alkalinisation then IUI/IVF
- Complication (rate)
- DVT/PE 2-5% (lower than posterior fusion)
- Management
- Venous duplex / CT pulmonary angiography; therapeutic anticoagulation for 3 months
- Complication (rate)
- Left common iliac vein thrombosis 1-2% (delayed 2-7 days)
- Management
- Venous duplex; therapeutic anticoagulation 3-6 months; consider IVC filter if anticoagulation contraindicated
- Complication (rate)
- Subsidence 5-15% overall, 28% if osteoporotic (Tempel 2017)
- Management
- Observe if low grade/asymptomatic; supplemental posterior fixation if high grade or symptomatic with a well-positioned cage; revision ALIF if malpositioned/pseudarthrosis
- Complication (rate)
- Pseudarthrosis 5-10%
- Management
- CT at 6-12 months; smoking cessation, avoid NSAIDs; revision with posterior fixation ± larger cage/BMP
- Complication (rate)
- Adjacent segment disease 10-20% at 10 years
- Management
- Conservative first (PT, NSAIDs, ESI); extend fusion if refractory; maintain lordosis at the index fusion
Anterior thoracolumbar fusion overall. In a large multicentre review of 1223 anterior thoracic and lumbar fusions the complication rate attributable to the anterior surgery was 11.5% — serious events were rare (death 0.3%, paraplegia 0.2%, deep infection 0.6%) and concentrated in patients over 60, women, and the medically comorbid (Faciszewski 1995). Complications are approach-specific, reinforcing careful approach selection and an experienced exposure team. Post-operative course. Most patients go to a regular ward (no routine ICU/HDU). Multimodal analgesia (acetaminophen, NSAIDs if not contraindicated, low opioid requirements), out of bed day 0-1, catheter removed day 1, and discharge typically day 2-3 (shorter than posterior fusion). For a stand-alone construct wear an LSO brace for 6-12 weeks during upright activity; avoid bending, lifting greater than 10 pounds, and twisting; resume walking immediately and driving at 2-4 weeks off opioids. Typical return to sedentary work is 4-8 weeks and to manual labour 3-6 months, guided by fusion progression.
Procedures Through This Approach
- Anterior lumbar interbody fusion (ALIF) at L4-5 and L5-S1 — the principal operation, stand-alone or with supplemental posterior fixation (circumferential/360 degree fusion).
- Total disc replacement (arthroplasty) at L4-5 / L5-S1.
- Anterior release for deformity — ALL release for lordosis restoration in flatback or sagittal deformity correction.
- Vertebral body / corpectomy procedures and revision disc surgery (where the circumferential construct's lower reoperation rate is advantageous — Christensen 2002).
- Circumferential fusion constructs for major instability, revision, or multi-level disease.
Viva & Exam Focus
VASCULARVASCULAR — protecting vessels during anterior lumbar surgery
EJACULATEEJACULATE — preventing retrograde ejaculation at L5-S1
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“During an L5-S1 ALIF you are mobilising the left common iliac vein and encounter sudden brisk venous bleeding. Your assistant applies direct pressure. How do you manage this vascular injury?”
“A 35-year-old man returns 6 weeks after L5-S1 ALIF reporting 'no semen during orgasm' since resuming sexual activity. What is the mechanism, prognosis, and how do you counsel him?”
“A 68-year-old woman with poor bone quality (T-score -2.8) had a stand-alone L4-5 ALIF (cage only, no posterior fixation). At 4 months she develops recurrent back pain and radiographs show 5 mm cage subsidence into the L5 superior endplate. How do you manage this?”
Approach by level
- L4-5: LEFT retroperitoneal — aorta/left iliac artery mobilised medially, IVC stays right
- L5-S1: MIDLINE pre-sacral window between the iliac vessels, below the iliocaval confluence
- Aortic bifurcation usually at L4 (variable L3-L5 in 10-15%)
Signature dangers
- Left common iliac vein at L5-S1 — commonest source of major bleeding (Inamasu 2006)
- Ascending lumbar (iliolumbar) vein — ligate BEFORE mobilising (commonest avulsion)
- Superior hypogastric plexus — retrograde ejaculation 0.5-5% of males, permanent (Tiusanen 1995)
- Ureter and bowel — protected by staying retroperitoneal (peritoneum anterior)
Vascular injury rules
- Direct pressure first (5-10 minutes)
- Primary venous repair with 5-0/6-0 Prolene
- NEVER ligate the main left common iliac vein (causes DVT); only the ascending lumbar tributary can be ligated
- Call access/vascular surgery for uncontrolled or arterial injury
Preventing retrograde ejaculation
- Retroperitoneal (not transperitoneal) approach in males
- Blunt midline pre-sacral dissection, sweep the plexus to one side as a single layer
- Bipolar (not monopolar) cautery over the disc
- Mandatory consent and offer of sperm banking
Fusion biology & subsidence
- Circumferential fusion: 92% union vs 80% posterolateral, reoperation 7% vs 22% (Christensen 2002)
- Subsidence ~10-12% stand-alone; high grade predicts revision OR ~12 (Tempel 2017)
- Add posterior fixation for poor bone quality, multilevel, or instability
References
Vascular Injury and Complication in Neurosurgical Spine Surgery
- Comprehensive literature review of vascular injury across spinal procedures, categorised by approach (cervical fixation, ALIF, disc arthroplasty, discectomy, posterior surgery)
- Vascular injury is uncommon but not rare, and its consequences can be devastating; incidence can be reduced by understanding the mechanism of injury for each procedure
- Vascular injury associated with ALIF is highlighted as a particular concern that may be underestimated in the literature
- Anterior lumbar exposure places the iliac vessels and inferior vena cava directly at risk; meticulous anatomical knowledge and careful technique are the principal protective measures
Retrograde Ejaculation After Anterior Interbody Lumbar Fusion
- Retrospective study of 40 male patients after anterior interbody lumbar fusion (mean age 31.9 years, mean follow-up 5 years)
- Retrograde ejaculation occurred in 9 patients and became permanent in 7 (17.5%); all of these had been operated through a transabdominal (transperitoneal) approach
- Seven of the affected patients had undergone two-level (L4-S1) surgery and several had had previous spine operations — reoperation and multilevel surgery increase risk
- The authors explicitly recommend AGAINST the transabdominal approach in male patients because of the retrograde ejaculation risk
Circumferential Fusion (ALIF Cage + Posterior) vs Instrumented Posterolateral Fusion — RCT
- Prospective randomised trial of 148 patients (146 analysed) with severe chronic low back pain, 2-year follow-up: circumferential fusion (ALIF Brantigan cage plus posterior instrumentation) vs instrumented posterolateral fusion alone
- Posterolateral fusion rate was higher in the circumferential group (92% vs 80%, p less than 0.04)
- Reoperation rate (including implant removal) was markedly lower with circumferential fusion (7% vs 22%, p less than 0.009)
- Circumferential fusion better restored and maintained sagittal lordosis and showed less peak back pain at 2 years and less leg pain at 1 year
Perioperative Complications of Anterior Thoracolumbar Spinal Fusion — 1223 Procedures
- Retrospective review of 1223 anterior thoracic and lumbar spinal fusions (T1-S1) in adults over 1969-1992
- Complication rate directly attributable to the anterior surgery was 11.5%; serious events were rare — death 0.3%, paraplegia 0.2%, deep wound infection 0.6%
- Risk of complication was increased in patients over 60 years, in women, and in those with multiple pre-existing medical problems
- Complications were frequently approach-specific, underscoring the importance of approach selection and meticulous exposure technique
Graft Subsidence as a Predictor of Revision After Stand-Alone Interbody Fusion
- Retrospective review of 297 patients undergoing stand-alone interbody fusion; 34 (11.4%) had radiographic subsidence and 18 (6.1%) required revision surgery
- Median subsidence grade was 2.5 (Marchi criteria) in those needing revision vs 1 in those who did not
- High-grade subsidence was a strong independent predictor of revision (OR ~12, 95% CI 1.29-13.6), whereas age, BMI, DEXA T-score and number of levels were not significant in this model
- Seven of 18 revision patients (38.9%) had an associated vertebral body fracture
ALIF — Patient Selection and Pre-operative Workup
- Review of patient-selection criteria and workup for ALIF, emphasising the unique complication profile of the anterior corridor
- Key selection variables include age, sex, bone density, BMI, nicotine use, comorbidity, and the anatomy of the distal iliac vein / aorta / iliac bifurcation / iliocaval confluence
- Prior abdominal surgery, infection or radiotherapy, operative level, surgical goals, and availability of an approach co-surgeon all influence suitability
- Recommended minimum workup: lumbar MRI, standing flexion/extension and long-cassette radiographs, non-contrast lumbar CT, and DEXA