Subacromial / supraspinatus · Gärtner Type I–III · barbotage ± arthroscopic excision
- Gärtner classification drives management: Type I (dense, homogeneous, sharply defined) is often asymptomatic and aspirates poorly; Type III (fluffy, resorptive) is the most painful stage, aspirates beautifully and may resolve spontaneously — but barbotage is first-line when acutely symptomatic.
- Barbotage (ultrasound-guided needle lavage and aspiration) is the first-line intervention after failed conservative therapy (physiotherapy, NSAIDs, a subacromial corticosteroid injection). Do not proceed to arthroscopic excision before attempting barbotage, except for a hard Type I deposit where aspiration is technically impossible.
- Arthroscopic excision is indicated after failed barbotage or for a hard Type I deposit. The supraspinatus 'critical zone' about 1–2 cm proximal to the greater tuberosity insertion is the most common site; localise the deposit with a transcutaneous 18G needle under arthroscopic vision before incising the tendon.
- Assess rotator cuff integrity before and after excision: if greater than 50% of tendon thickness is removed, a formal rotator cuff repair is required. Add subacromial decompression only where genuine concomitant impingement is documented — routine acromioplasty adds no benefit in isolated calcific tendinitis.
When & Why
The problem. Calcific tendinitis (hydroxyapatite deposition disease) is a self-limiting, reactive, cell-mediated calcification of the rotator cuff — not a degenerative process. Deposits cycle through a formative (resting) phase and a resorptive phase; the resorptive phase is intensely painful but is precisely when spontaneous resolution tends to occur. Most deposits sit in the supraspinatus, around 70–80% of cases, classically in the hypovascular 'critical zone' about 1–2 cm proximal to the greater tuberosity insertion. Management is a ladder. Climb it deliberately — examiners expect a stepwise approach and will penalise jumping straight to surgery.
NSAIDs (e.g. naproxen 500 mg BD), physiotherapy (pendulum, range of motion, posture), and a subacromial corticosteroid injection to settle acute pain and enable therapy. Extracorporeal shockwave therapy (ESWT) is an evidence-based alternative for Type I/II deposits.
Ultrasound-guided needle lavage and aspiration once conservative care has failed, particularly for soft Type II/III deposits. Combine with a subacromial corticosteroid to limit the post-procedure flare.
Reserved for failed barbotage (two attempts) or a hard Type I deposit that cannot be aspirated. Excise the deposit, assess the cuff, repair if greater than 50% thickness is lost.
Why barbotage before surgery. A randomised controlled trial (de Witte et al. 2013, PMID 23696211) showed ultrasound-guided needling and lavage combined with a subacromial corticosteroid produced significantly better Constant scores and greater deposit resorption at one year than an isolated subacromial corticosteroid injection (mean Constant 86.0 versus 73.9 at 12 months). A Level I network meta-analysis (Arirachakaran et al. 2017, PMID 27554465) ranked barbotage with subacromial corticosteroid as the treatment of choice among non-operative options. Soft resorptive (Type III) deposits aspirate readily; hard, dense formative (Type I) deposits aspirate poorly and are the recognised cause of barbotage failure. Operative thresholds (all should be met) before arthroscopic excision: 1. Persistent symptoms severe enough to affect quality of life or work. 2. Failure of a minimum 3 months of conservative treatment. 3. Failure of at least one barbotage attempt — or barbotage technically impossible (hard Type I deposit). 4. Imaging confirmation of a calcium deposit on plain film plus ultrasound. Absolute contraindications. Active shoulder infection, uncontrolled medical comorbidities, or a patient unwilling to commit to postoperative rehabilitation. Consent specifically for a post-procedure flare (barbotage) or postoperative stiffness (arthroscopic), incomplete pain relief, residual calcification on imaging, and — critically — possible rotator cuff repair, because the size of the deposit on imaging does not predict intraoperative tendon involvement. Setup. Barbotage is performed in a procedure room with the patient supine or seated and a high-frequency (15 MHz) linear ultrasound probe. Arthroscopic excision is done in the beach-chair (or lateral decubitus) position under general anaesthesia or an interscalene block.
Examiners expect a stepwise ladder: conservative care for at least three months, then barbotage, then surgery. Operating on a patient who has not had barbotage — unless aspiration is technically impossible for a hard Type I deposit — is a recognised exam failure.
The Operation
There are two operations on this page. Arthroscopic excision is the true surgical operation, and its exposure — the posterior viewing portal and lateral working portal into the subacromial space — is laid out as the opening steps below. Barbotage is the ultrasound-guided office intervention that precedes it on the ladder. Both are taught in full because the page is about how each is actually performed.

Arthroscopic excision — operative sequence
- Beach chair (preferred) or lateral decubitus, under general anaesthesia or interscalene block.
- Examine under anaesthesia: document range of motion, Hawkins-Kennedy and Neer signs, and cross-body adduction — this confirms any impingement component and guides whether a decompression is added.
- Posterior viewing portal: 2 cm inferior and 1 cm medial to the posterolateral corner of the acromion — the primary window into the subacromial space.
- Lateral working portal: 2–3 cm lateral to the midpoint of the acromion — for the shaver, burr, and any suture anchors, and for transcutaneous needle localisation.
- Anterolateral accessory portal: added only when extra working access or suture-anchor placement is needed for a cuff repair.
- Axillary nerve safety: the nerve exits the quadrilateral space and runs about 5–6 cm below the acromion. Keep every portal within 3 cm of the acromion edge so the nerve is not at risk.
- Insert the arthroscope through the posterior portal into the glenohumeral joint.
- Inspect the articular surfaces, labrum, biceps anchor, and the articular side of the rotator cuff. Document any articular-side partial tear before moving to the subacromial space.
- Withdraw the scope and redirect through the posterior portal into the subacromial space; establish the lateral working portal.
- Perform a thorough bursectomy with a motorised shaver, clearing inflamed bursal tissue off the superior cuff. A clean bursal surface is what lets you see the deposit — inadequate bursectomy is the commonest reason a deposit is missed.
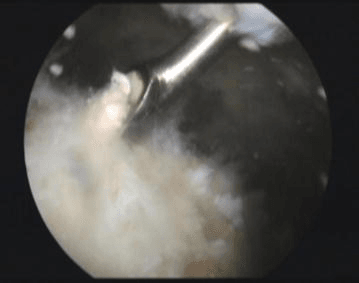
- Inspect the bursal surface of supraspinatus systematically, anterior to posterior. The deposit appears as a yellowish-white bulge or chalk-coloured mass — firm in Type I, soft and expressive in Type III.
- If no bulge is visible, palpate the cuff with a blunt probe: a focal area of firmness locates an intatendinous deposit (Type I feels hard, Type III feels slightly soft versus normal tendon).
- Pass an 18G needle transcutaneously from the lateral portal into the subacromial space, directing it toward the suspected deposit.
- Under arthroscopic vision, confirm the needle tip touching the tendon at the deposit. Localise precisely BEFORE incising the tendon — this prevents over-excision and keeps the incision over the deposit.
- Through the lateral portal, use an arthroscopic knife or electrocautery to make a longitudinal incision over the deposit, parallel to the tendon fibres to minimise strength loss.
- Curette and shave the calcium out until normal-appearing tendon is exposed; express remaining calcium with a probe and irrigate thoroughly.
- Probe the residual tendon and classify the defect by thickness: less than 25%, 25–50%, or greater than 50%.
- Less than 25% — debride the edges, no repair (heals by secondary intention). 25–50% — surgeon discretion based on tissue quality, age and demand. Greater than 50% — formal rotator cuff repair is mandatory (single-row for a defect less than 2 cm wide; double-row transosseous-equivalent for a defect 2–3 cm wide or a high-demand patient).
- Visualise the coracoacromial arch from the lateral portal. If there is a hooked acromion or a frayed coracoacromial ligament, perform an acromioplasty with the arthroscopic burr (resect 5–8 mm of the inferior acromion, smoothing to a flat/Type I profile).
- If there is no genuine impingement, preserve the coracoacromial arch — routine acromioplasty in isolated calcific tendinitis is not supported.
- Close the portal wounds. If no block was used, inject intra-articular bupivacaine/morphine for postoperative analgesia.
- Apply a sling. The rehabilitation pathway depends on whether a cuff repair was performed (see Aftercare).
Keep portals within 3 cm of the acromion — the axillary nerve lies 5–6 cm distally and is injured by portals placed too far down the arm or by aggressive retraction during decompression. Avoid excessive tendon excision: a longitudinal incision parallel to the fibres, a curette rather than an aggressive shaver, and a preserved tendon margin keep the defect under control — and if it nevertheless exceeds 50% thickness, repair it then and there rather than leaving a defect that will propagate.
Work through the sequence in order: thorough bursectomy first, then systematic palpation with a blunt probe (Type I hard, Type III soft), then transcutaneous 18G needle localisation. If it still cannot be found, use C-arm fluoroscopy to confirm the needle tip lies within the deposit seen on the plain film. Only very rarely — a purely intatendinous deposit with no bursal expression — do you need a careful longitudinal incision over the X-ray-confirmed location or conversion to a 1.5 cm mini-open exposure.
For a defect greater than 50% that needs repair: lightly burr the greater tuberosity footprint to bleeding cancellous bone (do not over-resect). Single-row for a 1–2 cm defect — one or two suture anchors at the medial footprint margin with a Mason-Allen or modified mattress suture, tied with the arm in about 30 degrees of abduction. Double-row transosseous-equivalent (TOE) for a defect 2–3 cm wide or a high-demand patient — a medial row at the articular margin and knotless lateral-row anchors 5–8 mm lateral, the sutures crossed to compress and maximise footprint contact. Confirm the repair holds without gapping in adduction.
Barbotage — ultrasound-guided lavage and aspiration
- Patient supine or seated in a high chair, arm in slight internal rotation to bring supraspinatus into view.
- High-frequency (15 MHz) linear probe in a sterile sleeve. Long-axis view of supraspinatus: the deposit is a hyperechoic focus with posterior acoustic shadowing within the tendon substance.
- Sterile skin preparation. Infiltrate 5 mL of 1% lidocaine into the skin and subcutaneous tissue along the planned needle track.
- Introduce an 18G needle in-plane with the ultrasound beam so the tip is seen dynamically, and advance onto the calcium deposit. Confirm position with a first puncture.
- Two-needle technique (one inlet for lavage, one outlet for aspiration) or a single-needle pulsed technique.
- Inject saline in 2–5 mL aliquots and aspirate back, repeating 10–15 cycles. Aspirate the chalky white or milky material — the volume aspirated varies and may be small even when fragmentation succeeds.
- Optional: 1 mL of methylprednisolone acetate 40 mg co-injected into the subacromial bursa (not into the tendon) to reduce the post-procedure flare.
- Ice, oral analgesia, and a sling for 24–48 hours.
- Expect a post-procedure flare — pain worse for 24–72 hours from a calcium crystal shower — in about 30–40% of patients. This is not a failure. Begin physiotherapy from day 3.
Aftercare & Complications
Rehabilitation The pathway depends on which intervention was performed and whether a cuff repair was added. | Procedure | 0–2 weeks | 2–6 weeks | 6–12 weeks | 12+ weeks | |-----------|-----------|-----------|------------|-----------| | Barbotage | Sling for comfort, ice, analgesia | Discard sling; pendulum and active ROM as tolerated; physiotherapy | Progressive strengthening | Return to sport/heavy work | | Arthroscopic excision (no repair) | Sling for comfort; early pendulum exercises | Discard sling; active ROM; progressive physiotherapy | Strengthening — rotator cuff, deltoid, periscapular | Return to sport/heavy work | | Arthroscopic excision + cuff repair | Sling; passive ROM only (pendulums, assisted); no active elevation | Active-assisted ROM; gradual active elevation; no resisted exercise | Progressive strengthening (bands, weights); pool therapy | Full activity; heavy overhead work from 6 months | Most patients are pain-free by about 3 months after excision without repair, with full recovery at 4–6 months; recovery is longer (6 months) when a cuff repair was performed. Expected outcomes - Barbotage: significant pain and function improvement is usual, with progressive radiographic resorption over 6–12 months; barbotage plus a subacromial corticosteroid outperforms steroid injection alone at one year (de Witte et al. 2013, PMID 23696211).
- Arthroscopic excision: reliable for deposits refractory to non-operative treatment. The original arthroscopic series (Ark et al. 1992, PMID 1637430) reported 50% good and 41% satisfactory results in chronic resistant cases; modern series report good or excellent outcomes in roughly 85–90%, with return to full function at 3–5 months (longer with a cuff repair).
- Acromioplasty: routine acromioplasty adds no benefit in isolated calcific tendinitis without structural impingement — outcome is determined by the adequacy of calcium removal, not by acromioplasty. Reserve SAD for genuine concomitant impingement.
- Recognition
- No bursal bulge; firm intatendinous Type I or small deposit; view obscured by bursa
- Prevention
- Thorough bursectomy before inspection; systematic anterior-to-posterior palpation; transcutaneous needle localisation; fluoroscopy if needed
- Management
- Extend bursectomy, palpate systematically, confirm with C-arm; rarely delayed re-arthroscopy or a 1.5 cm mini-open exposure
- Recognition
- A defect greater than 50% of tendon thickness after debridement
- Prevention
- Longitudinal incision parallel to fibres; curette over an aggressive shaver; preserve the tendon margin
- Management
- Formal rotator cuff repair (single- or double-row by defect size); document the defect and repair
- Recognition
- Distal portal placement or aggressive retraction during SAD
- Prevention
- Keep all portals within 3 cm of the acromion (nerve lies 5–6 cm distally)
- Management
- Neurology review; expectant management or exploration depending on the deficit
- Recognition
- Pain worse for 24–72 hours after the procedure
- Prevention
- Warn the patient pre-procedure; co-inject subacromial corticosteroid
- Management
- NSAIDs, ice, oral analgesia; settles spontaneously — not a failure
- Recognition
- Residual calcium on follow-up imaging
- Prevention
- Adequate lavage cycles at the index procedure
- Management
- Observe if asymptomatic; repeat barbotage or proceed to arthroscopic excision if symptomatic
- Recognition
- Post-excision adhesion, an unrepaired large defect, or excessive immobilisation
- Prevention
- Early physiotherapy; repair defects greater than 50%; a structured rehabilitation protocol
- Management
- Physiotherapy; subacromial steroid for secondary impingement; MRI if a re-tear is suspected
Viva & Exam Focus
GARTNERGARTNER — the classification that drives management
CALCIUMCALCIUM — the management ladder
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old nurse presents with 6 months of right shoulder pain. Plain radiograph shows a 2 cm calcium deposit at the supraspinatus insertion. The radiograph shows a dense, sharply-defined homogeneous opacity. How do you assess this and decide on management — and how would your approach differ if the deposit appeared fluffy with indistinct margins?”
“During arthroscopic excision of a large Type I supraspinatus deposit in a 52-year-old active man, you estimate the residual defect at about 60% of tendon thickness. What are your intraoperative and postoperative decisions?”
“A 48-year-old teacher had ultrasound-guided barbotage six weeks ago for a Type II deposit. She reports minimal improvement and the follow-up ultrasound shows the deposit largely unchanged. How do you manage her now?”
Gärtner classification
- Type I (formative): homogeneous, sharply defined, chalk-like; often asymptomatic; hard to aspirate
- Type II (transitional): mixed, intermediate density; variable symptoms
- Type III (resorptive): fluffy, indistinct margins, toothpaste consistency; most painful; aspirates well; may resolve spontaneously
- Type III most symptomatic but most likely to resolve — do not rush to surgery on a Type III
Indications
- Conservative failure: minimum 3 months of NSAIDs, physiotherapy and a subacromial steroid
- Barbotage is the first-line intervention after conservative failure, especially Type II/III
- Arthroscopic excision: failed barbotage (two attempts), impossible aspiration (hard Type I), or a large mechanical deposit
- Do not operate before a barbotage attempt — examiners penalise it
Barbotage technique
- Ultrasound-guided, 18G needle, in-plane for dynamic tip visualisation
- Two-needle (lavage + aspiration) or single-needle pulsed technique
- Saline in 2–5 mL aliquots, 10–15 cycles; end-point is chalky/milky aspirate
- Co-inject subacromial methylprednisolone 40 mg to reduce flare
- Warn the patient: 30–40% have a 24–72 hour flare before improvement
Arthroscopic key steps
- Beach chair; posterior portal for viewing, lateral portal for working
- Glenohumeral inspection first — exclude articular-side partial tears
- Thorough bursectomy to visualise the deposit
- Transcutaneous 18G needle localisation under vision before incising tendon
- Longitudinal incision parallel to fibres; curette and shaver to remove calcium
- Add SAD only if documented impingement — never routine
Rotator cuff decision
- Less than 25% thickness: debride, no repair
- 25–50%: surgeon discretion by age, demand, tissue quality
- Greater than 50%: formal suture-anchor repair mandatory
- Always consent for possible rotator cuff repair
- If repaired: sling 6 weeks, passive ROM only 0–6 weeks, strengthening from 12 weeks
Key anatomy
- Supraspinatus critical zone: 8–10 mm proximal to insertion, relatively avascular (Moseley and Goldie 1963) — commonest deposit site
- Subacromial space height 7–14 mm; contents: bursa, coracoacromial ligament, cuff bursal surface
- Axillary nerve 5–6 cm below the acromion — no risk if portals stay within 3 cm
- Posterior viewing portal: 2 cm inferior, 1 cm medial to the posterolateral acromion corner
Complications
- Post-barbotage flare (30–40%): calcium crystal shower; settles 24–72 hours
- Incomplete aspiration: more common with Type I — repeat or ESWT before surgery
- Cuff defect after excision: repair if greater than 50% thickness
- Failure to identify deposit: thorough bursectomy and needle localisation
- Post-excision stiffness: early physiotherapy; longer immobilisation if repaired
Background & Evidence
Epidemiology. Radiographic calcific deposits are found in roughly 3–8% of adult shoulders, with a higher proportion among symptomatic patients. Peak presentation is age 30–60 years with a slight female predominance, and deposits are bilateral in 10–25%. Calcific tendinitis is distinct from degenerative rotator cuff disease: patients are typically younger and the cuff is usually intrinsically intact. Natural history. This is a self-limiting reactive (cell-mediated) calcification, not a degenerative process. Deposits cycle through a formative (resting) phase and a resorptive phase; the resorptive phase (Gärtner Type III) is intensely painful but is precisely when spontaneous resolution occurs, frequently over a few weeks. Formative (Type I) deposits may persist for years with inconsistent symptoms. Spontaneous resorption is the rule rather than the exception (Gärtner and Heyer 1995, PMID 7617385). Pathoanatomy. Calcification most commonly occurs in supraspinatus (around 70–80% of cases), classically about 1–2 cm proximal to the greater tuberosity insertion — the 'critical zone' of relative hypovascularity described by Moseley and Goldie (1963). Poor blood supply in this zone impairs healing and explains why calcification and rotator cuff tears cluster in the same region. Less common sites are infraspinatus and subscapularis. The subacromial space is 7–14 mm high on outlet view (average 9–10 mm); reduction to less than 6 mm suggests impingement or a full-thickness cuff tear. The coracoacromial arch (coracoid, coracoacromial ligament, acromion) protects the superior cuff; a Bigliani Type III (hooked) acromion increases impingement risk but is not the cause of calcific tendinitis per se.
- Radiographic appearance
- Dense, homogeneous, sharply defined borders
- Consistency & symptoms
- Chalk-like, hard; often asymptomatic; aspirates poorly
- Typical management
- Conservative; ESWT; arthroscopic excision if refractory
- Radiographic appearance
- Mixed, partly homogeneous and partly inhomogeneous
- Consistency & symptoms
- Intermediate density; variable symptoms
- Typical management
- Conservative then barbotage; excision if it fails
- Radiographic appearance
- Fluffy, cloudy, indistinct margins
- Consistency & symptoms
- Soft, toothpaste-like; MOST acutely painful; aspirates well; may resolve spontaneously
- Typical management
- Barbotage first-line; rarely needs surgery
Key evidence. Gärtner and Heyer (1995, PMID 7617385) defined the three-type classification and the two-phase natural history, reporting needling resorption rates of about 33% for Type I and 71% for Type II, with Type III resolving over about 2–3 weeks with or without treatment. de Witte et al. (2013, PMID 23696211) randomised barbotage plus subacromial corticosteroid versus steroid alone and found superior Constant scores (86.0 versus 73.9 at one year) and greater deposit resorption. Gerdesmeyer et al. (2003, PMID 14625334) showed both high- and low-energy ESWT beat sham, with high-energy superior. Arirachakaran et al. (2017, PMID 27554465) pooled the evidence in a Level I network meta-analysis and ranked barbotage with subacromial corticosteroid as the treatment of choice among non-operative options. The consistent message — a non-operative ladder led by barbotage, with surgery reserved for genuine failures — is why arthroscopic excision is the last, not the first, step.
References
Calcific tendinitis of the shoulder — radiographic classification and natural history
- Defines the three-type radiographic classification: Type I dense and sharply circumscribed (formative), Type III translucent and cloudy without clear margins (resorptive), Type II intermediate/indeterminate.
- Frames calcific tendinitis as a two-phase, largely self-limiting disease: formative deposits may persist for years while the acute resorptive phase causes 2–3 weeks of severe pain followed by resolution.
- Reported needling resorption rates of approximately 33% for Type I and 71% for Type II deposits, with about 50% of patients becoming pain-free.
- Type III deposits undergo resorption in about 2–3 weeks with or without treatment.
Ultrasound-guided needling and lavage versus subacromial corticosteroids: a randomized controlled trial
- 48 patients randomised to barbotage plus subacromial corticosteroid injection versus isolated subacromial corticosteroid injection.
- At 1 year the mean Constant score was 86.0 in the barbotage group versus 73.9 with steroid alone (P =.005).
- Mean calcification size decreased by 11.6 mm with barbotage versus 5.1 mm with steroid alone (P =.001).
- Adjusted treatment effect of about 20.5 Constant points in favour of barbotage.
Extracorporeal shock wave therapy for chronic calcifying tendonitis of the rotator cuff: a randomized controlled trial
- Double-blind placebo-controlled trial of 144 patients comparing high-energy ESWT, low-energy ESWT and sham.
- Both ESWT groups improved the 6-month Constant-Murley score significantly more than sham (high-energy +31.0, low-energy +15.0, sham +6.6 points).
- High-energy ESWT was significantly superior to low-energy ESWT (P less than.001).
- ESWT also reduced self-rated pain and the radiographic size of calcific deposits.
ESWT, ultrasound-guided lavage, corticosteroid injection and combined treatment for rotator cuff calcific tendinopathy: a network meta-analysis of RCTs
- Network meta-analysis of seven RCTs comparing barbotage, ESWT, subacromial corticosteroid injection and combinations.
- Combined ultrasound-guided needling plus subacromial corticosteroid injection most reduced pain (VAS), improved Constant score and decreased deposit size.
- No significant difference in adverse events between treatment groups.
- Identified barbotage with subacromial corticosteroid as the treatment of choice among non-surgical options.
Arthroscopic treatment of calcific tendinitis of the shoulder
- Case series of 23 patients with chronic resistant calcific tendinitis treated by arthroscopic calcium removal and subacromial bursectomy.
- Results: 50% good (full motion, complete pain relief), 41% satisfactory, 9% unsatisfactory at mean 26-month follow-up.
- Partial calcium removal occurred in 13 of 23 and complete removal in 9 of 23 patients.
- Established arthroscopic excision with bursectomy as a reasonable option for deposits resistant to conservative treatment.
The arterial pattern of the rotator cuff of the shoulder — the critical zone
Defined the arterial supply of the rotator cuff and the 'critical zone' — a region about 8–10 mm proximal to the supraspinatus insertion on the greater tuberosity that is relatively hypovascular. This zone of reduced perfusion is the most common site of calcium deposition and of rotator cuff tearing, and underpins the rationale for careful tendon-sparing excision and repair.