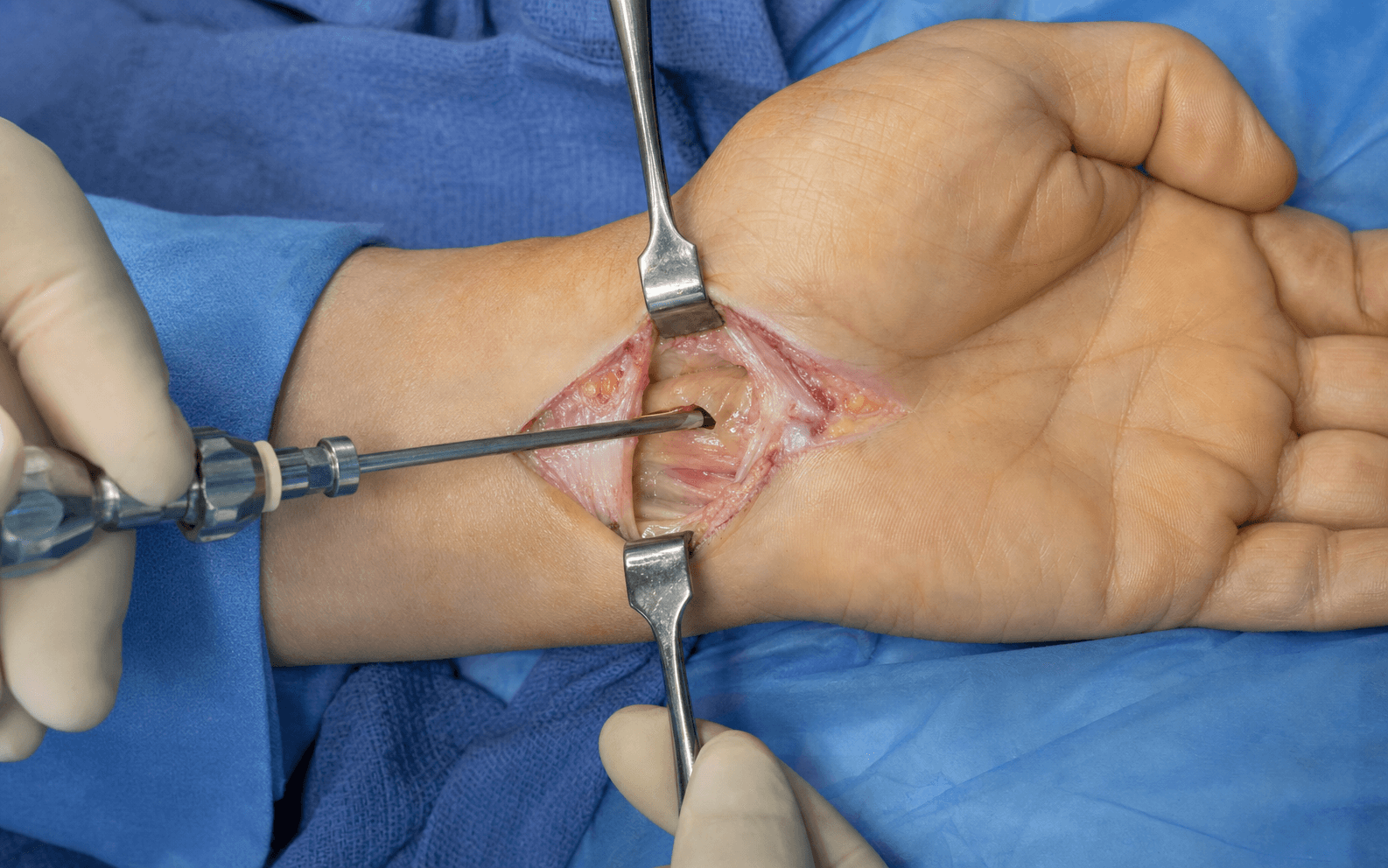
Single-portal endoscopic technique (Agee) · proximal wrist incision | advanced
- Single-portal (Agee) technique uses a proximal wrist incision between palmaris longus and FCR; the endoscope sits on the radial side of the tunnel with its blade slot radial, the camera faces ulnarly, so the blade cuts radially AWAY from a median nerve held on the ulnar (left) side of the screen throughout.
- Patient selection is the critical determinant of success: EXCLUDE masses in the tunnel, a bifid median nerve, anomalous muscles, revision surgery and severe tenosynovitis or wrist arthritis limiting extension. Unsuitable anatomy drives the complication rate up dramatically.
- The distal fat pad is the critical STOP sign: the yellow fatty tissue marks the end of the transverse carpal ligament (TCL) and prevents superficial palmar arch injury if the blade is carried too distally.
- Incomplete release (2-8 percent) is the most common endoscopic-specific complication - higher than open (1-3 percent) - usually from an inadequate distal release or missed bridging fibers, and is prevented by meticulous withdrawal and re-inspection before closure.
- Multiple RCTs and the Cochrane review show EQUIVALENT long-term outcomes to open CTR but faster return to work (about 8 days earlier) and faster grip strength recovery (50 percent by 2 weeks versus 6 weeks). Endoscopic carries higher equipment cost; choice is driven by recovery speed and preference, not by superior cure rates.
- Conversion to open (1-5 percent) is appropriate surgical judgement, not failure. The learning curve is 25 or more cases for proficiency, with higher complication rates in the first 25 cases.
When & Why
Indication. Symptomatic carpal tunnel syndrome (CTS) - numbness and tingling in the median distribution, nocturnal waking, thenar weakness if severe, a positive Phalen's test and Tinel's sign - confirmed electrodiagnostically (EMG/NCS showing moderate-to-severe median nerve slowing across the wrist), that has failed conservative management (a nocturnal wrist splint, activity modification, NSAIDs and at least one corticosteroid injection). The corticosteroid injection gives reliable short-term relief (around three months) but surgery is superior long-term. Assess suitability for the endoscopic route specifically. Endoscopic CTR trades a smaller scar and faster recovery for a restricted view and a learning curve, so it is a technique for correctly selected patients in correctly trained hands.
Isolated idiopathic CTS with electrodiagnostic confirmation (moderate-severe slowing), normal wrist anatomy, no masses or variants, a wrist that extends comfortably to 20-30 degrees, and a patient who wants the fastest possible return to work. The surgeon should be past the 25-case learning curve.
A mass in the tunnel (ganglion, tumour, thrombosed persistent median artery), a bifid median nerve, anomalous muscles (lumbrical origin in the tunnel, an accessory FDS belly), revision CTR (scarring distorts anatomy), and severe wrist arthritis that prevents the extension needed for scope insertion.
Severe tenosynovitis (rheumatoid arthritis, gout) that obscures visualisation, pregnancy (defer - CTS often resolves postpartum), acute CTS with a space-occupying lesion, and a surgeon still in the learning curve (the first 25 cases).
Consent specifically for the endoscopic-specific risks: an incomplete release rate of 2-8 percent (higher than open at 1-3 percent, and higher again in the learning curve), nerve injury 0.5-2 percent, and the possibility of intraoperative conversion to open (1-5 percent). Document that long-term outcomes are equivalent to open CTR. Counselling and contemporaneous consent documentation are essential in any medico-legal environment. Setup. Supine with the arm abducted 90 degrees on a hand table, an upper-arm tourniquet (250 mmHg, exsanguinate with an Esmarch bandage or elevation). The wrist is extended 20-30 degrees on a commercial holder or folded towels; the fingers are relaxed in natural cascade with NO traction; the forearm is fully supinated. Loupe magnification is recommended and a working monitor is positioned for the surgeon's direct viewing. Anaesthesia is most commonly a regional block (axillary or supraclavicular); wide-awake local anaesthesia no tourniquet (WALANT, 1 percent lidocaine with 1:100,000 epinephrine) is an alternative - the patient can move the fingers to demonstrate the release - though bleeding may obscure the endoscopic view.
The Operation
The goal: divide the transverse carpal ligament (TCL) completely from its proximal to its distal edge under endoscopic vision, with the median nerve held safely on the ulnar side of the screen and the blade cutting radially away from it, stopping at the distal fat pad, then inspect for completeness before a splint-free closure. The portal and exposure are laid out in full below - they are the heart of the operation.
Operative sequence
- Supine, hand table, upper-arm tourniquet, wrist in 20-30 degrees extension, fingers relaxed, forearm supinated, monitor at the head.
- Mark the anatomy with the patient awake: the palmaris longus (PL) tendon (flex the wrist against resistance), the FCR tendon radial to it, the pisiform, the ring-finger ray (the alignment line), and the distal wrist crease (approximate proximal TCL edge).
- The portal site is 1 cm proximal and ulnar to the pisiform, between PL and FCR, aligned with the ring finger. If PL is absent (15 percent of people), use FCR and the ring-finger alignment, entering just ulnar to FCR.
- Make a 1-2 cm transverse or longitudinal incision at the distal wrist crease between PL and FCR. Deepen through subcutaneous fat with blunt spreading dissection.
- Protect the palmar cutaneous branch of the median nerve, which exits the nerve 5-8 cm proximal to the wrist, pierces the antebrachial fascia between PL and FCR and runs subcutaneously to the thenar skin. Staying between PL and FCR and deep to the fat protects it; a portal-site neuroma occurs in 2-3 percent if it is injured.
- Identify the glistening antebrachial fascia and make a 1-2 cm longitudinal opening in it; this is continuous with the TCL proximally and opens into the tunnel.
- Use a Freer elevator or mosquito to sweep synovium and fat off the tunnel floor, creating a space that accepts the scope WITHOUT forcing. Visualise the proximal TCL edge - the transverse white fibres where the tunnel roof begins - before proceeding. Obtain haemostasis with bipolar cautery (sparing, never near the nerve).
- Confirm the wrist is in 20-30 degrees extension (a goniometer helps): this straightens the carpal tunnel axis, aligns the scope with the tunnel long axis, and opens the proximal tunnel. More than 30 degrees narrows the tunnel as the carpal bones approximate and raises median nerve pressure.
- Fingers must be relaxed, never tractioned - traction pulls the flexor tendons and with them the median nerve volarward toward the blade. The forearm is fully supinated (palm up), which carries the nerve ulnarly and is protective.
- Tourniquet to 250 mmHg for a bloodless field; note the inflation time (aim for less than 30 minutes). Check the light source, camera focus, blade deployment, and irrigation before the scope enters the tunnel.
- The Agee single-portal scope has the blade slot on the radial side and the camera facing ulnarly. The defining safety check: the median nerve must appear on the ULNAR (left) side of the screen throughout, because the blade cuts radially, away from the nerve.
- Insert along the tunnel long axis at roughly 10-15 degrees to the forearm, gliding along the tunnel floor (carpal bones dorsally) with minimal resistance. If there is resistance, STOP - re-check wrist position, enlarge the portal, or reassess; never force.
- Identify the proximal TCL edge (transverse white fibres), the median nerve on the ulnar side (yellowish, fascicles sometimes visible), the smooth whitish tunnel floor (scaphoid, capitate), and the flexor tendons ulnar to the nerve.
- If the nerve appears on the RADIAL (right) side, the scope is mal-positioned - withdraw and reinsert. If orientation is lost or the view is poor despite irrigation and repositioning, convert to open.
- Advance slowly under continuous vision, keeping the nerve on the ulnar (left) side and the transverse TCL fibres overhead. At mid-tunnel (about 1-1.5 cm in) the TCL is thickest (2-3 mm) and the nerve may show a chronic indentation or flattening.
- Watch for the DISTAL FAT PAD: yellow fatty tissue appearing once the last transverse TCL fibres end. This is the STOP sign - the superficial palmar arch lies 1-2 cm beyond it.
- Before cutting, confirm the whole tunnel has been visualised (proximal edge, mid-tunnel, distal fat pad) and that no variant is present. If a bifid nerve (two bundles), a persistent median artery, anomalous muscle, or severe proliferative tenosynovitis is seen, STOP and convert to open.
- With the scope at the proximal TCL, deploy the blade through its radial slot (5-8 mm). Apply gentle steady upward pressure of the blade against the TCL toward the roof - let it cut; do not jab or force.
- Begin at the proximal edge. Some surgeons make partial-thickness passes first then deepen them; others cut full-thickness in one pass. Watch the individual transverse fibre bundles divide and the TCL begin to gap open. Minimal bleeding is expected (the TCL is relatively avascular).
- The blade cuts radially, away from the nerve. If it tracks ulnarly toward the nerve, STOP and reposition. If resistance is met, check blade deployment and angle before continuing.
- Advance the scope 1-2 mm at a time, maintaining upward cutting pressure, dividing the TCL continuously from proximal to distal. Confirm at every step that the nerve stays on the ulnar side, the fibres divide overhead, and there is no bleeding.
- At mid-tunnel (thickest TCL) do not force - ensure full-thickness division so the gap opens 5-10 mm before advancing further.
- Continue until the transverse fibres END and the distal fat pad is clearly visible, then STOP. The blade must not extend beyond the fat pad. Retract the blade fully once the release is complete. The commonest error is stopping too proximal and leaving distal bridging fibres.
- With the blade retracted, withdraw the scope slowly under vision, inspecting the whole release: TCL edges gap 5-10 mm throughout, the median nerve is rounded and decompressed with no indentation, the distal fat pad is visible, and there is no arterial bleeding.
- Now re-inspect: withdraw to the portal and re-advance, viewing the whole tunnel again from a fresh perspective. A single inspection misses bridging fibres; two full-length views are the minimum.
- Look specifically for bridging fibres distally (the commonest site), along the deep ulnar edge, and in the superficial radial fibres. If bridges are found, re-deploy the blade and divide them under direct vision, then re-inspect. If the view is inadequate to confirm completeness, convert to open.
- Withdraw the scope. Endoscopic CTR causes little bleeding because the TCL is avascular and there is no large dissection plane.
- Release the tourniquet before closure to reveal any arterial bleeding it was masking. Brisk bleeding after release suggests a vessel injury and demands exploration.
- Irrigate the portal. Close the subcutaneous layer with 3-0 or 4-0 absorbable suture and the skin with 4-0 or 5-0 nylon (removed 7-10 days), a subcuticular Monocryl, or skin adhesive.
- Apply a soft, non-compressive dressing - NO splint. Immediate mobilisation is one of the key benefits of the endoscopic route; splinting negates it and raises CRPS and stiffness risk. Elevate the hand above the heart.
- Median nerve and recurrent motor branch - keep the nerve on the ULNAR (left) side and the blade cutting radially; a Type III Lanz motor branch (about 23 percent) crosses superficial to the distal TCL and is at risk during the distal cut. 2. Superficial palmar arch - stop at the distal fat pad; the arch is 1-2 cm distal to the TCL. 3. Ulnar neurovascular bundle (Guyon's canal) - 5-10 mm ulnar to the tunnel; keep the portal radial and never angle the scope ulnarly. 4. Palmar cutaneous branch - protected by a portal between PL and FCR; injury gives a painful thenar neuroma. 5. Flexor tendons - keep the scope on the tunnel floor and do not cut tendons; severe tenosynovitis is a relative contraindication.
In the Agee single-portal system the blade slot is radial and the camera faces ulnarly, so with the median nerve on the ulnar (left) side of the screen the blade cuts radially, AWAY from the nerve. Wrist extension of 20-30 degrees straightens the tunnel axis, and relaxed (non-tractioned) fingers keep the nerve sitting naturally on the ulnar side. These three points - nerve ulnar, blade radial, wrist extended - are the safety spine of the operation.
A low threshold for conversion is a sign of safe practice. Convert for: poor visualisation despite irrigation and repositioning, an anatomical variant (bifid nerve, anomalous muscle, persistent median artery), suspected nerve or vessel injury, inability to advance safely, equipment failure, or any doubt about completeness. Extend the proximal incision distally into the palm along the standard open trajectory and complete the release under direct vision; outcomes equal a primary open CTR.
Aftercare & Complications
Rehabilitation | Phase | Timing | Management | Milestones | |-------|--------|-----------|------------| | 1 | 0-48 hours | Soft dressing only, NO splint; elevate; begin finger/thumb active ROM hourly; ice 20 min on/off | Pain control, neurovascular checks | | 2 | Day 1 to 2 weeks | Remove bulky dressing for a simple adhesive bandage; keep dry until sutures out (7-10 days); light ADLs; start scar massage once epithelialised | Return to office/light work 7-14 days | | 3 | 2-6 weeks | Therapy putty and graded grip strengthening; moderate activities | Grip 50 percent of baseline by 2 weeks, 80 percent by 6 weeks | | 4 | 6-12 weeks | Heavy activities, manual labour, contact sports based on grip recovery | Grip 80-90 percent by 6 weeks, full by 12-16 weeks | | 5 | 3-12 months | Scar maturation; address any residual pillar pain | Final strength plateau by 4-6 months | Return to work depends on demand: office/sedentary 7-14 days (about 5-7 days earlier than open); light manual 2-3 weeks; moderate manual 3-6 weeks; heavy manual 6-12 weeks. Around 90-95 percent report significant symptom relief, with 85-90 percent satisfaction and 2-5 percent recurrence at 5-10 years (the same as open). Simple analgesia (paracetamol, a short opioid course) covers postoperative pain; an anti-staphylococcal antibiotic is first-line if infection occurs, guided by local antimicrobial policy. Liaise with the relevant workers-compensation insurer for a structured return-to-work plan where applicable. Complications
- Recognition
- Persistent median symptoms postoperatively (numbness, nocturnal waking), positive Phalen's and Tinel's; EMG at 6-8 weeks shows persistent slowing; ultrasound may show residual TCL fibres. Most common endoscopic complication.
- Prevention
- Meticulous inspection before closure; withdraw and re-inspect the whole tunnel (second view); cut to the distal fat pad; look for bridging fibres especially distally; low threshold to convert.
- Management
- Confirm with exam and EMG. Revision CTR using an OPEN approach (not endoscopic - scarring). Good results if pure incomplete release (about 90 percent relief), poorer if nerve injury coexists.
- Recognition
- Intraop: disrupted epineurium or bleeding from the nerve. Postop: dense median numbness, loss of thumb opposition, progressive weakness, neuroma pain. Higher in the learning curve.
- Prevention
- Nerve ulnar on screen throughout, blade radial, clear vision always, never force; convert if anatomy unclear.
- Management
- Intraop recognition: convert to open, microsurgical repair (8-0/9-0 nylon). Postop: urgent EMG; explore a complete injury within 72 hours; observe a partial injury 3-6 months; graft or transfer if no recovery.
- Recognition
- Thenar atrophy over weeks-months, weak opposition/abduction; sensation intact. EMG shows thenar denervation.
- Prevention
- Know the Lanz Type III anatomy (branch crossing superficial to distal TCL); limit the distal cut to the fat pad; if thenar wasting suggests a high branch, choose open.
- Management
- If recognised intraop, microsurgical repair (8-0 nylon). If recognised late, explore within 72 hours if complete; otherwise observe 3-6 months; consider opponensplasty (EIP or FDS) if no recovery by 6 months.
- Recognition
- Brisk arterial bleeding during the distal release; pulsatile flow; haematoma; rarely digital ischaemia (collaterals usually adequate). May appear only after tourniquet release.
- Prevention
- STOP cutting at the distal fat pad; never extend beyond it; preoperative Doppler if a high arch is suspected.
- Management
- Stop cutting, convert to open, identify the vessel (usually ulnar artery or arch), control with pressure then vascular clamps, repair with 6-0/7-0 prolene; check distal perfusion; ligate only if unrepairable and collateral flow adequate.
- Recognition
- Ulnar-sided numbness, weak intrinsics (clawing), haematoma or ulnar-digit ischaemia.
- Prevention
- Portal between PL and FCR; keep the scope radial; never force or angle ulnarly.
- Management
- As for median nerve injury: identify extent, microsurgical repair if complete; control bleeding and check perfusion; monitor for compartment syndrome.
- Recognition
- Painful thenar neuroma at the portal site, hypersensitivity, a positive Tinel at the scar; often delayed weeks-months.
- Prevention
- Portal between PL and FCR; blunt subcutaneous dissection deep to the fat; protect the branch if seen.
- Management
- Conservative first: desensitisation, scar massage, silicone, gabapentin/pregabalin. A confirmed neuroma: excision and burial into deeper tissue or muscle.
- Recognition
- Disproportionate pain, allodynia, hyperalgesia, autonomic changes (swelling, warmth, colour), reduced ROM. Budapest criteria. Same rate as open CTR.
- Prevention
- Avoid splinting; encourage early mobilisation; adequate perioperative pain control; vitamin C 500 mg daily (limited evidence).
- Management
- Early recognition is critical. Multimodal: neuropathic agents (gabapentin/pregabalin), hand therapy (desensitisation, graded motor imagery, mirror therapy), psychological support, stellate ganglion blocks if severe, multidisciplinary pain clinic.
- Recognition
- Increasing pain, erythema, warmth, purulent drainage; fever suggests deep infection (flexor tenosynovitis, septic arthritis). Usually Staphylococcus aureus.
- Prevention
- Sterile technique; minimise portal trauma; optimise diabetic glucose control; prophylactic antibiotics where indicated (routine use for clean hand surgery is debated).
- Management
- Superficial: oral anti-staphylococcal antibiotic (e.g. flucloxacillin or cephalexin), wound care, close follow-up. Deep: emergency washout, IV antibiotics (flucloxacillin or vancomycin if MRSA risk), send cultures, extended course.
- Recognition
- Excessive or progressive swelling, a tense compartment feel; a large haematoma can compress the nerve and cause recurrent symptoms.
- Prevention
- Meticulous haemostasis; release the tourniquet before closure to find arterial bleeding; avoid perioperative anticoagulation where safe; non-compressive dressing.
- Management
- Small: observe, elevate, compress. Large or expanding: return to theatre for evacuation and haemostasis; culture if evacuated.
- Recognition
- Not a complication but appropriate judgement: poor visualisation, a variant, suspected injury, inability to advance, equipment failure, or doubt about completeness.
- Prevention
- Good patient selection and surgeon experience reduce the rate; a low threshold protects the patient.
- Management
- Extend the incision distally into the palm (3-5 cm total), complete the release under direct vision, address the reason for conversion; outcomes equal a primary open CTR.
Viva & Exam Focus
SAFE-ESAFE-E for endoscopic CTR safety
PORTALPORTAL for single-portal setup
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old secretary with severe bilateral CTS requests endoscopic release because a colleague returned to work within a week. She takes apixaban for atrial fibrillation. How do you counsel her on endoscopic versus open CTR, and what does the evidence show?”
“During an Agee single-portal release, after what you believe is complete, you withdraw the scope and see a small strand of tissue bridging the TCL edges distally. The patient is a manual labourer who wanted endoscopic for a faster return to work. How do you manage this intraoperative finding, and what are the implications of incomplete release?”
“A 38-year-old electrician presents 48 hours after an endoscopic CTR (by another surgeon) with severe burning pain across the whole hand, marked swelling, shiny skin, allodynia (cannot tolerate clothing contact) and a hand warmer than the other side. Sutures are intact, no infection signs. What is your differential, most likely diagnosis, and management plan?”
Indication and selection
- Symptomatic CTS failing conservative care, confirmed with EMG/NCS (moderate-severe median slowing)
- Exclude masses, bifid nerve, anomalous muscles, revision surgery, severe tenosynovitis, wrist arthritis limiting extension
- Higher equipment and disposable cost than open; equivalent long-term outcomes - recovery speed and preference drive choice
Critical anatomy
- TCL 2-3 cm long, 2-3 mm thick; the distal fat pad (yellow fat) is the STOP sign
- Median nerve enters radially and courses ulnarly - keep it on the ULNAR (left) of the screen; recurrent motor branch exits radially (Lanz types)
- Superficial palmar arch 1-2 cm distal to the TCL; palmar cutaneous branch exits 5-8 cm proximal and runs between PL and FCR
- Agee system: blade slot RADIAL, camera faces ULNAR, blade cuts radially AWAY from the nerve; wrist 20-30 degrees extension
Critical steps
- Portal 1-2 cm between PL and FCR, 1 cm proximal/ulnar to the pisiform, aligned with the ring finger; incise the antebrachial fascia
- Insert with the nerve on the ULNAR (left) side; advance to the distal fat pad under continuous vision
- Cut from proximal TCL to the fat pad with steady upward pressure; the TCL should gap 5-10 mm
- Withdraw and RE-INSPECT the whole tunnel (second view); look for bridging fibres especially distally; convert if any doubt
Danger zones
- Median nerve and recurrent motor branch (Lanz Type III, about 23 percent, crosses superficial to the distal TCL)
- Superficial palmar arch (1-2 cm distal to the TCL - stop at the fat pad)
- Ulnar neurovascular bundle in Guyon's canal (5-10 mm ulnar)
- Palmar cutaneous branch (2-3 percent neuroma) and the flexor tendons
Technique pearls
- Wrist 20-30 degrees extension; fingers RELAXED (traction pulls the nerve volar toward the blade)
- Distal fat pad is the STOP sign - must be seen before stopping
- Always withdraw and re-inspect; the commonest error is stopping too proximal
- Learning curve 25+ cases for proficiency; conversion 1-5 percent is appropriate judgement
Complications
- Incomplete release 2-8 percent (versus 1-3 percent open); revision is OPEN, about 90 percent relief if pure incomplete
- Nerve injury 0.5-2 percent; CRPS 5-10 percent (same as open); arch injury 0.3-1 percent; infection less than 1 percent
- Conversion to open 1-5 percent - not a complication
Post-op and outcomes
- Immediate ROM, soft dressing NO splint, sutures 7-10 days
- Return to work 7-14 days light (about 5-7 days earlier than open); 3-6 weeks heavy manual
- Grip 50 percent by 2 weeks (versus 6 weeks open), full by 12-16 weeks
- Long-term outcomes EQUIVALENT to open; recurrence 2-5 percent at 5-10 years
Background & Evidence
The condition. Carpal tunnel syndrome is compression of the median nerve beneath the transverse carpal ligament at the wrist. When it persists despite a splint and a corticosteroid injection, surgical division of the ligament is the definitive treatment. Endoscopic release divides the same ligament and decompresses the same nerve as open release - it simply does so through a smaller wrist incision under camera vision, in exchange for a restricted view and a learning curve. Applied anatomy for the endoscopic route. The TCL (flexor retinaculum) is a dense band 2-3 cm long and 2-3 mm thick, attaching radially to the scaphoid tubercle and trapezium ridge and ulnarly to the pisiform and hook of hamate. When fully divided it gaps 5-10 mm and its edges retract. The median nerve enters the tunnel radial to the centre and courses ulnarly; in the endoscopic view it must sit on the ulnar (left) side of the screen throughout. The tunnel also carries the nine digital flexor tendons (4 FDS, 4 FDP, FPL) ulnar to the nerve. The superficial palmar arch (chiefly the ulnar artery) lies 1-2 cm distal to the TCL; the palmar cutaneous branch leaves the median nerve 5-8 cm proximally and runs between PL and FCR. Relevant variants include a persistent median artery (about 10 percent), a bifid median nerve (1-3 percent), and anomalous lumbrical origins or accessory FDS bellies (2-3 percent) - all are reasons to choose open.
- Course of the motor branch
- Extraligamentous - exits radially BEYOND the distal TCL edge
- Risk in endoscopic release
- Safest; the branch is protected during release
- Course of the motor branch
- Subligamentous - exits at or just distal to the TCL edge, may run partly under it
- Risk in endoscopic release
- Moderate; careful distal release required
- Course of the motor branch
- Transligamentous - crosses superficial to the distal TCL to reach the thenar muscles
- Risk in endoscopic release
- Highest; the blade can transect it during the distal cut. If thenar wasting suggests a high branch, consider open
- Course of the motor branch
- Supraligamentous - exits proximally and runs over the whole TCL
- Risk in endoscopic release
- Rare; usually identified intraoperatively
Single-portal versus two-portal. The single-portal (Agee) technique uses one proximal wrist incision with the blade and camera in one assembly; it cannot directly see the palmar cut surface of the TCL but has a shorter learning curve and no palmar incision, and is the most widely used route internationally. The two-portal (Chow) technique adds a distal palm portal so both sides of the TCL can be seen, at the cost of a palmar incision (more early palmar pain) and a higher superficial arch injury risk, with a longer learning curve. Meta-analyses show no significant difference in outcomes, complications or incomplete-release rates between the two - surgeon familiarity drives the choice.
- Open release
- 3-5 cm palm incision crossing the wrist crease
- Single-portal endoscopic
- 1-2 cm wrist incision at the distal crease only
- Open release
- Direct view of the whole TCL, nerve and arch; variants seen easily
- Single-portal endoscopic
- Limited scope view; cannot see the palmar side of the TCL; variants may be missed
- Open release
- 14-28 days moderate work; 6-12 weeks heavy work
- Single-portal endoscopic
- 7-14 days light/moderate (about 5-7 days earlier); 3-6 weeks heavy work
- Open release
- 50 percent at 6 weeks, 80 percent at 12 weeks, full by 6 months
- Single-portal endoscopic
- 50 percent at 2 weeks, 80 percent at 6 weeks, full by 3-4 months
- Open release
- 1-3 percent (usually distal TCL or antebrachial fascia), easily revised
- Single-portal endoscopic
- 2-8 percent, higher in the learning curve; bridging fibres commonest; needs revision open CTR
- Open release
- 0.3-1 percent; usually recognised and repaired at once
- Single-portal endoscopic
- 0.5-2 percent, higher in the learning curve; may not be recognised until postop
- Open release
- Minimal; taught in residency
- Single-portal endoscopic
- 25+ cases for proficiency, 100 for expertise; higher early complications
- Open release
- Low - standard instruments, minimal disposables
- Single-portal endoscopic
- Higher - capital system plus single-use blade/cannula per case
- Open release
- 85-95 percent satisfaction; recurrence 2-5 percent
- Single-portal endoscopic
- Equivalent; 85-95 percent satisfaction; same recurrence (Level 1 evidence)
Key evidence. The defining trial of this technique is the original Agee multicentre RCT (1992): a 10-centre study of 122 patients (147 hands) in which median return to work for single-affected-hand patients was 21.5 days earlier with the endoscopic device, with two reoperations (only one a true incomplete release) and two transient ulnar neurapraxias. The Vasiliadis Cochrane review (2014, 28 trials, 2586 hands) found equivalent long-term symptom relief and an equal major complication rate, with return to work about 8 days earlier after endoscopic (mean difference -8.1 days, 95 percent CI -14.3 to -1.9) but more transient nerve symptoms. The Scholten Cochrane review of surgical techniques (2007, 33 trials) found no alternative superior to standard open release and an earlier return to work with endoscopic (weighted mean difference -6 days, 95 percent CI -9 to -3). The Atroshi 5-year RCT confirmed durable equivalence in symptom severity, function, pillar-type pain and reoperation (3 per group). The consistent message - equivalent long-term outcomes and faster recovery, but a higher incomplete-release rate that falls with experience - is why strict patient selection, cutting to the distal fat pad, and meticulous re-inspection are the operation's safety spine, and why this is a perennial viva topic.
References
Endoscopic release for carpal tunnel syndrome (Cochrane systematic review)
- 28 randomised/quasi-randomised trials, 2586 hands, comparing endoscopic (ECTR) with open carpal tunnel release (OCTR)
- Return to work or daily activities was on average 8 days earlier after ECTR (mean difference -8.1 days, 95% CI -14.3 to -1.9)
- No difference in symptom severity, functional status, or long-term overall improvement; grip strength slightly favoured ECTR
- Major complication rates equal (RR 1.00); ECTR had fewer minor/wound complications but more transient nerve symptoms; recurrence and reoperation rates comparable
Endoscopic release of the carpal tunnel: a randomized prospective multicenter study (original Agee single-portal trial)
- 10-centre RCT, 122 patients (147 hands), single-portal endoscopic device versus conventional open release
- For patients with one affected hand, median return to work was 21.5 days earlier in the endoscopic device group
- Strength and tenderness variables were the best predictors of return to work and to activities of daily living
- Two device-group patients required reoperation (only one a true incomplete release); two had transient ulnar neurapraxia
Open compared with 2-portal endoscopic carpal tunnel release: a 5-year follow-up of a randomized controlled trial
- Single-centre RCT, 128 patients with electrophysiologically confirmed idiopathic CTS; 126 reviewed at 5 years
- No difference in CTS symptom severity (mean difference in change 0.03, 95% CI -0.21 to 0.27) or functional status at 5 years
- Persistent scar/proximal palm pain in 11 open versus 10 endoscopic patients (no meaningful difference in pillar-type pain)
- Repeat surgery for persistent/recurrent symptoms in 3 patients per group
Anatomical variations of the median nerve in the carpal tunnel (basis of the Lanz classification)
- 246 operatively explored hands plus pooled literature, classifying median nerve variations into four groups
- Thenar (recurrent motor) branch course (Poisel cadaver data): extraligamentous 46%, subligamentous 31%, transligamentous 23%
- High (bifid) division of the median nerve and accessory branches proximal and distal to the tunnel are described variants
- Emphasises approaching the median nerve from the ulnar side when opening the carpal tunnel
Surgical treatment options for carpal tunnel syndrome (Cochrane review of surgical techniques)
- 33 RCTs of surgical techniques; no alternative offered better short- or long-term symptom relief than standard open release
- Across 3 trials (294 participants), endoscopic release gave earlier return to work/activities (weighted mean difference -6 days, 95% CI -9 to -3)
- No strong evidence to replace standard open release with any alternative procedure
- Choice between endoscopic and open release is guided by surgeon and patient preference
Complications of endoscopic and open carpal tunnel release (the learning curve)
- Prospective series of 200 consecutive endoscopic CTR cases characterising the learning curve
- First 25 cases: 8% incomplete release, 2 nerve injuries; cases 26-100: 3% incomplete release, no nerve injuries; cases 101-200: 1% incomplete release (equivalent to open)
- Operative time fell from 45 min initially to 15 min after 100 cases
- Conclusion: 25 cases minimum for proficiency, 100 for expertise