Emergency posterior midline decompression · intermediate
- Cauda equina syndrome (CES) is a surgical emergency: decompress as soon as safely feasible and within 48 hours of onset to optimise neurological recovery, especially bladder function.
- Classic features: saddle anaesthesia, bladder dysfunction (retention progressing to overflow incontinence), and bilateral lower-limb neurological deficit. Confirm the level and the cause on emergency MRI before operating.
- The commonest cause is a massive L4-5 or L5-S1 disc herniation (around 70 percent); also tumour, abscess, haematoma or trauma — the decompression follows the same principle whatever the cause.
- Adequate decompression means a complete laminectomy with visualisation of all compressed roots, clearing the lateral recesses and confirming dural pulsation before closure.
- The two cardinal avoidable errors are wrong-level surgery (prevented by systematic counting and fluoroscopy) and dural tear (prevented by keeping the Kerrison foot-plate on bone, never on dura).
When & Why
Indication. Acute cauda equina syndrome — a clinical diagnosis of compression of the cauda equina nerve roots demanding emergency decompression. Operate when there is confirmed CES on examination (saddle anaesthesia, bladder dysfunction, bilateral leg weakness) together with MRI confirmation of a compressive lesion (disc, tumour, haematoma or abscess), particularly with a progressive neurological deficit. A high-suspicion CES-S picture (bilateral radiculopathy with bladder or bowel symptoms but a normal examination) and a severe isolated unilateral radiculopathy that may progress are relative indications to image and operate. Contraindications are few and mostly relative: a patient medically unfit for anaesthesia (discuss with anaesthetics — most can be optimised rapidly), complete cauda equina transection with no recovery potential (rare), symptoms of very long duration (less likely to recover but surgery still prevents progression), and concomitant deformity needing instrumented fusion (may warrant a staged or different strategy). A delayed presentation is never a reason not to operate. Timing — the evidence (state it precisely; examiners probe this). - The 48-hour threshold. Ahn et al. (Spine 2000, meta-analysis of 322 patients) found a statistically significant advantage for decompression within 48 hours versus beyond 48 hours for sensory, motor, urinary and rectal recovery — but no significant difference between the under-24-hour and 24-48-hour groups. The older dogma that one "must operate within 24 hours" is not supported by this dataset.
- Within 24 hours still matters in incomplete CES. Srikandarajah et al. (Spine 2015, 200 patients) showed that in CES-incomplete (CES-I), decompression within 24 hours of autonomic symptom onset reduced bladder dysfunction at follow-up, whereas in CES-retention (CES-R) the timing of surgery made no significant difference to the bladder outcome.
- Do not pool CES-R and CES-I. DeLong et al. (J Neurosurg Spine 2008) showed later surgery predicts a worse urinary outcome and that CES-R and CES-I behave differently — they must be analysed separately.
- Beyond 48 hours, returns diminish for recovery but surgery is still indicated to prevent further deterioration. The defensible, evidence-based position: aim to decompress as soon as safely feasible and within 48 hours of CES onset; in CES-I there is additional benefit to operating within 24 hours; a delayed presentation still warrants urgent decompression. Avoid quoting a rigid single recovery percentage tied to a precise hour cut-off unless you can attribute it correctly.
The default for a true CES emergency. Wide exposure, complete decompression, direct visualisation of every root, and able to deal with unexpected tumour or abscess.
Predominantly unilateral pathology with some contralateral involvement. Preserves the midline ligaments by undercutting the spinous process and contralateral lamina.
Tubular, unilateral laminotomy with medial facetectomy crossing the midline. Selected central discs without stenosis only — not for a true CES emergency, where speed and completeness matter.
Add a concurrent fusion when there is pre-existing spondylolisthesis (Meyerding grade 2 or more), degenerative scoliosis with coronal imbalance, iatrogenic instability, or a bilateral facetectomy is required; it adds about 60-90 minutes, so in the emergency decompress first and stage the fusion if needed. Consent specifically for residual bladder, bowel and sexual dysfunction (common even after well-timed surgery), incomplete recovery of motor and sensory deficit, dural tear with CSF leak, infection, and the small but real risk of recurrent herniation. CES is among the most litigated spinal conditions — document timing, baseline neurology and the consent discussion meticulously. Setup. Prone on a Wilson frame or Jackson table with the abdomen hanging free (this drops epidural venous pressure and improves the field), hips flexed to open the interspinous spaces, shoulders abducted less than 90 degrees, face on a horseshoe or prone-view headrest, and all pressure points padded. Lateral fluoroscopy is mandatory for level confirmation.
The Operation
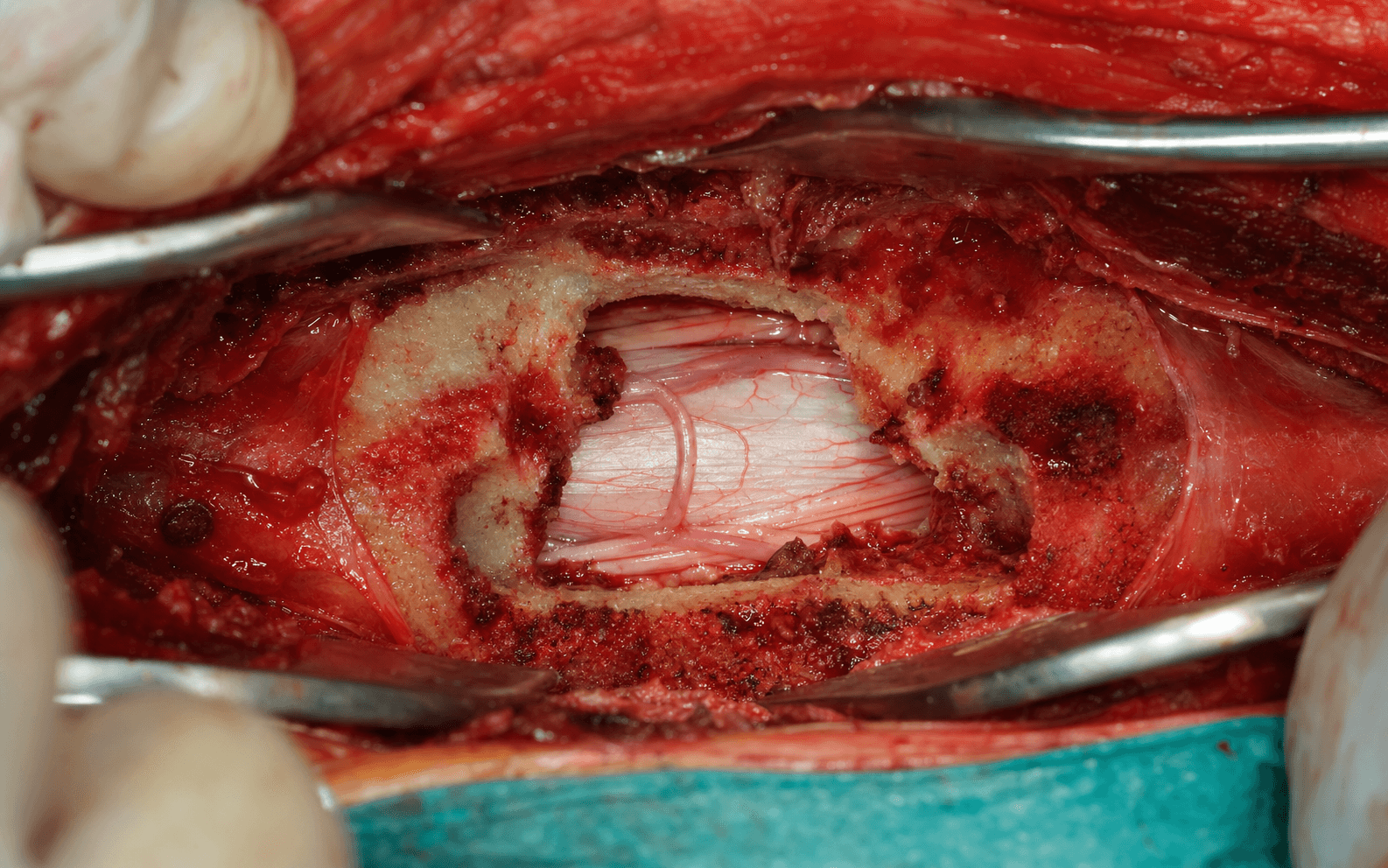
The goal: through a posterior midline approach, expose the laminae at the level of maximum compression, perform a complete laminectomy and lateral recess decompression while protecting the dura and nerve roots, remove the compressive pathology (most often a large sequestrated disc fragment), confirm a free and pulsating thecal sac, and close in layers. The exposure — getting safely onto the correct lamina — is the first and most important part of the case.
Operative sequence
- Review the MRI immediately before surgery to identify the exact level of maximum compression, the extent of decompression required (single versus multi-level), the type of pathology (disc, tumour, abscess, haematoma), and any anatomical variant (transitional vertebra, spondylolisthesis, vascular anomaly).
- Count vertebrae on the sagittal MRI from the sacrum upwards or from C2 downwards to avoid counting errors. Lumbosacral transitional vertebrae (Bertolotti's syndrome) occur in 10-15 percent — correlate with plain radiographs.
- Look specifically for cranial or caudal disc migration, common in CES, so the decompression spans it.
- Induce general anaesthesia with full muscle relaxation for safe intubation and turning.
- Position prone on a Wilson frame or Jackson table. The abdomen must hang free — pass a hand underneath the patient to confirm; this drops epidural venous pressure by 40-50 percent and dramatically improves the field.
- Hips flexed to open the interspinous spaces; shoulders abducted less than 90 degrees to avoid brachial plexus stretch; face on a horseshoe or prone-view rest with the eyes free; pad knees, chest and iliac crests.
- Prepare the skin with chlorhexidine or povidone-iodine from the mid-thoracic spine to the sacrum; drape to expose the spinous processes from L3 to the sacrum. Allow alcohol-based prep to dry fully — it is a fire hazard with diathermy.
- Palpate the spinous processes of L4, L5 and the sacrum; in obese patients use lateral fluoroscopy to mark the skin before incision.
- Make a strictly midline incision centred on the pathology: 6-8 cm for a single L4-5 level, 5-7 cm for L5-S1, adjusted for multi-level disease. Incise skin and subcutaneous fat to the supraspinous ligament with cutting diathermy.
- Using a Cobb elevator or cutting diathermy, perform subperiosteal dissection from the spinous processes onto the laminae bilaterally, out to the medial facet joints. Keep the elevator against bone at all times to keep bleeding paraspinal.
- Place a self-retaining Taylor or McCulloch retractor to hold the paraspinal muscles laterally. Do not violate the facet capsule — dissection too lateral causes bleeding and risks instability.
- Place a radiopaque marker (artery clip or K-wire) on the spinous process or lamina of the suspected level and obtain a lateral fluoroscopy image.
- Confirm by counting from the sacrum upwards (S1 is the first bony structure below the lucent L5-S1 disc). If in doubt, take an AP view and count ribs on the lateral view (T12 carries the last rib). Mark the level with a pen on the spinous process.
- Never proceed without absolute certainty of the correct level.
- With a Leksell or heavy bone-cutting rongeur, remove the spinous process of the affected level(s) and the interspinous ligament, exposing the cranial and caudal laminae.
- This creates the working space for the laminectomy and reduces the risk of inadvertent dural injury. Save bone fragments if fusion may be needed later; control cancellous bleeding with bone wax.
- With a Penfield dissector or Woodson elevator, clear muscle and soft tissue off the lateral lamina to expose the ligamentum flavum — yellow, elastic, normally 3-5 mm thick (7-10 mm when hypertrophied in stenosis).
- It extends from the antero-inferior edge of the cranial lamina to the anterosuperior edge of the caudal lamina. Once identified, you are at the boundary of the spinal canal. Use a ball-tip probe to develop the plane between ligamentum flavum and dura before resecting it.
- With a 2 mm or 4 mm Kerrison rongeur, remove the cranial lamina systematically from caudal to cranial, working from one lateral edge to the midline then midline to the other lateral edge. Repeat for the caudal lamina.
- The cardinal rule: keep the foot-plate of the Kerrison against bone at all times, never against the dura. Take deliberate 2-3 mm bites, not aggressive larger ones. Place cottonoid patties between dura and remaining bone to protect it.
- For L4-5 remove the inferior L4 and superior L5 laminae; for L5-S1 remove the inferior L5 and superior S1 laminae (the S1 lamina is often thick and may need thinning with a burr first).
- Perform a medial facetectomy with the Kerrison and/or high-speed burr to open the lateral recesses, removing the medial 25-30 percent of the facet (never more than 50 percent).
- The medial pedicle line (identifiable on lateral fluoroscopy) is the lateral limit of safe decompression — go beyond it and you destabilise the segment. Use a ball-tip probe to confirm each exiting root is decompressed and mobile, then repeat on the contralateral side.
- Inspect the epidural space. Most often a large sequestrated disc fragment is found posterolaterally or centrally; tumour is vascular and firm, abscess is purulent (send culture and histology), haematoma is dark and organised.
- Gently mobilise the dural sac away with a nerve hook or Penfield, placing a cottonoid patty between dura and fragment. If the dura is densely adherent, leave a thin sliver of disc on it and remove the bulk — chasing a complete dissection risks a tear.
- Grasp the fragment with pituitary rongeurs and remove it in a controlled, piecemeal fashion; CES fragments are often large (2-4 cm). Explore the disc space with angled curettes for loose material, but avoid aggressive intradiscal curettage (no benefit for recurrence and it increases back pain). An intradural fragment (3-5 percent) requires a durotomy.
- With a ball-tip probe or nerve hook, systematically check the L4, L5, S1 and S2 roots bilaterally. Decompressed roots are round and mobile; compressed roots are flattened and pale.
- Explore cranially and caudally from the disc space for migrated fragments (10-15 percent of cases), correlating with the pre-operative MRI. Cranial migration is commoner than caudal.
- Perform a systematic check: the dural sac pulsates freely, all roots are visualised and mobile, the lateral recesses are clear, and there is no residual compression.
- Ask the anaesthetist for a Valsalva manoeuvre (raise ventilator pressure to 30-40 cm H2O for 10 seconds): the dural sac should expand and bulge into the decompression. If it does not pulsate or expand, suspect residual compression or a CSF block and explore further.
- Achieve meticulous haemostasis: bipolar coagulation at low settings (20-30 W) for epidural ooze, bone wax for cancellous bleeding, gelfoam with thrombin or a haemostatic agent (Floseal) for persistent ooze. Epidural bleeding often settles once compression is relieved and the patient lies flat.
- Inspect the entire dural exposure for tears. Repair a tear primarily with 4-0 or 5-0 non-absorbable suture (Prolene or Nurolon), 2-3 mm bites and 2-3 mm apart, reinforce with a dural sealant, and confirm water-tightness with a Valsalva test.
- Irrigate with 1-2 litres of warm saline; perform a systematic cottonoid count before closure.
- Drain placement is surgeon preference — none for a single-level discectomy with a water-tight dura; consider one for a multi-level laminectomy or a coagulopathic patient, removed when output is less than 50 ml per 24 hours. Do not place a drain if there is a dural tear (it encourages ongoing CSF leak).
- Close the fascia water-tight with 1-Vicryl or PDS (1 cm bites, 1 cm apart), the subcutaneous layer to obliterate dead space, and the skin with absorbable subcuticular suture or clips. Apply a waterproof dressing.
- Before leaving theatre, perform and document a baseline examination: power in hip flexion, knee extension, ankle dorsiflexion and plantarflexion; dermatomal sensation; perianal sensation and anal tone; and bladder function (catheter output, and a trial of voiding within 24-48 hours).
- Worsening neurology immediately post-op demands urgent imaging for haematoma, wrong level or nerve injury.
Wrong-level decompression is a medicolegal catastrophe that demands a second operation and is almost entirely preventable. Avoid it by counting vertebrae systematically on the pre-operative MRI (from the sacrum upwards), marking the skin before positioning, confirming the level with intra-operative lateral fluoroscopy using a marker on the spinous process, accounting for transitional vertebrae (sacralised L5 or lumbarised S1 — a long lateral film resolves the doubt), and never proceeding without absolute certainty. Document the level check in the operative note.
Incidental durotomy occurs in 8-15 percent of primary cases (around 20 percent in revision surgery, where normal anatomy is replaced by scar). Prevent it by keeping the foot-plate of every Kerrison bite against bone, placing cottonoid patties to protect the dura, using magnification, and avoiding excessive retraction of adherent roots. If a tear occurs, repair it primarily with non-absorbable suture, reinforce with sealant, confirm water-tightness with a Valsalva, keep the fascial closure water-tight, and omit the drain. Entrap a nerve root in the repair and you cause a permanent radiculopathy.
Keeping the abdomen hanging free reduces epidural venous pressure by 40-50 percent. The engorged Batson epidural plexus is the main source of bleeding in acute CES; an abdomen-free position turns a bloody, obscured field into a clear one. Confirm it by passing a hand under the patient after turning.
Over-resecting the facet causes iatrogenic instability requiring fusion. Remove no more than the medial 25-30 percent of the facet (never more than 50 percent), use the medial pedicle line on lateral fluoroscopy as the lateral limit, and preserve the pars interarticularis. If a bilateral facetectomy is unavoidable, plan for a fusion.
Aftercare & Complications
Recovery timeline | System | Expected recovery | |--------|-------------------| | Motor | 70 percent improved by 6 weeks, 85 percent by 6 months | | Sensory | Slower — about 60 percent by 6 months | | Bladder | Around 50 percent back to normal by 3 months; little further recovery after 6 months | | Sexual function | Often a persistent deficit (about 50 percent of males) | Rehabilitation. Neurological observations every 2 hours for the first day; mobilise within 4-6 hours if there is no dural tear, with physiotherapy support. Manage the bladder with intermittent self-catheterisation if retention persists and refer to urology if there is no recovery by 6 weeks. Avoid bending, lifting and twisting for 6 weeks, no driving for 2 weeks, and a graded return — sedentary work at 4-6 weeks, light manual at 8-12 weeks, heavy manual and contact sports from 12 weeks. Recurrent disc herniation occurs in 5-10 percent (same level, same side); risk factors are young age, male sex, heavy occupation and smoking. Counsel patients pre-operatively that surgery prevents deterioration and optimises recovery, but residual deficits are common — document this discussion, as CES is highly litigious.
- Recognition
- CSF leak in the field; post-op clear wound discharge, positional headache, pseudomeningocele on MRI
- Prevention
- Kerrison foot-plate on bone, cottonoid protection, magnification, gentle retraction
- Management
- Primary repair 4-0/5-0 non-absorbable, dural sealant, water-tight fascia, no drain; bed rest 24-48 h if large
- Recognition
- New dermatomal sensory loss or myotomal weakness not present pre-op; foot drop (L5), weak plantarflexion (S1)
- Prevention
- Identify roots before manipulation, gentle retraction, avoid thermal injury, check all roots before closure
- Management
- Document mechanism; most neuropraxia recovers in 6-12 weeks; AFO for foot drop; EMG at 6 weeks; explore a complete deficit
- Recognition
- Retention beyond 48 h, incomplete emptying on bladder scan, overflow incontinence
- Prevention
- Early surgery, complete decompression, avoid root injury
- Management
- Intermittent self-catheterisation teaching, urology referral, urodynamics at 6 weeks, pelvic-floor physiotherapy
- Recognition
- Worsening neurology, severe pain, a progressing deficit; haematoma on urgent MRI/CT
- Prevention
- Meticulous haemostasis, correct coagulopathy, consider a drain in high-risk patients
- Management
- Urgent return to theatre for evacuation if a neurological deficit; observe if small and stable
- Recognition
- Wound erythema, discharge, fever; deep: severe back pain, raised CRP/ESR, endplate erosion
- Prevention
- Pre-op IV antibiotics within 60 min, aseptic technique, water-tight fascia, diabetic and smoking control
- Management
- Superficial: oral antibiotics and wound care. Deep: washout, cultures, IV antibiotics for 6-12 weeks
- Recognition
- Return of leg pain weeks to months post-op, the same distribution, new herniation on MRI
- Prevention
- Remove free fragments only; avoid aggressive intradiscal curettage; smoking cessation
- Management
- Conservative first; re-operation if it fails (higher complication rate); consider fusion if same level and side
- Recognition
- Mechanical back pain, dynamic translation more than 3 mm on flexion-extension films
- Prevention
- Preserve more than 50 percent of facets bilaterally, respect the medial pedicle line, keep the pars intact
- Management
- Conservative first with physiotherapy and bracing; instrumented fusion (TLIF or posterolateral) if it fails
- Recognition
- Inadequate improvement; MRI shows pathology at a different level
- Prevention
- Systematic MRI counting, fluoroscopic confirmation, count from the sacrum, team timeout
- Management
- Immediate disclosure, urgent re-operation at the correct level, full documentation and incident reporting
- Recognition
- Calf pain and swelling; shortness of breath and chest pain; confirmed on Doppler or CTPA
- Prevention
- Mechanical prophylaxis, early mobilisation, chemical prophylaxis if high risk
- Management
- Therapeutic anticoagulation; balance early post-op bleeding risk
- Recognition
- Persistent back or leg pain beyond 3-6 months, neuropathic features
- Prevention
- Appropriate selection, complete but not excessive decompression, expectation management
- Management
- Multidisciplinary pain management, neuropathic analgesia, physiotherapy; avoid repeat surgery without clear structural pathology
Viva & Exam Focus
SADDLESADDLE — the CES red flags
KERRISONKERRISON — safe laminectomy technique
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old man presents at 2 am with 24 hours of bilateral leg pain and numbness, saddle paraesthesia and urinary retention needing catheterisation. MRI shows a large L4-5 disc herniation with complete canal stenosis. The on-call anaesthetist says theatre is not available until the 8 am list tomorrow. How do you manage this?”
“During an emergency L5-S1 decompression with a Kerrison rongeur you notice clear fluid leaking and realise you have made a dural tear about 8 mm long, with neural tissue visible through it. How do you manage this intra-operatively?”
“A 62-year-old man has CES from an L4-5 disc herniation — bilateral leg weakness and saddle numbness over a week, with urinary retention for 48 hours. He takes rivaroxaban 20 mg daily for atrial fibrillation, last dose this morning. How do you proceed?”
Indication & timing
- Confirmed CES (saddle anaesthesia, bladder dysfunction, bilateral leg weakness) plus MRI compression — emergency decompression
- Decompress within 48 hours (Ahn 2000); within 24 hours adds bladder benefit in CES-I (Srikandarajah 2015); do not pool CES-R and CES-I (DeLong 2008)
- Delayed presentation still warrants urgent decompression — never use delay as a reason not to operate
Anatomy
- Conus ends at L1-L2; cauda equina roots descend in the thecal sac, each exiting below its pedicle (L5 below L5)
- Dural sac ends at S2, normally 10-15 mm (5-8 mm in CES); ligamentum flavum 3-5 mm (7-10 mm if hypertrophied)
- Adamkiewicz T8-L2 (left in 80 percent); the engorged Batson plexus is the main bleeding source
- The medial pedicle line is the lateral limit; preserve more than 50 percent of each facet
Critical steps
- Pre-op MRI: confirm level (count from the sacrum), pathology, extent, migration
- Fluoroscopic level confirmation — never proceed without certainty
- Laminectomy with the Kerrison foot-plate always on bone, cranial then caudal lamina
- Lateral recess decompression (medial 25-30 percent of facet, never more than 50 percent)
- Remove the fragment piecemeal, explore behind the roots and for migration
- Confirm adequacy: dural pulsation and a positive Valsalva test
Danger zones
- Dura and roots: foot-plate on bone, cottonoids, gentle retraction (tear 8-15 percent)
- Traversing and exiting roots: identify before manipulation
- Epidural plexus: abdomen-free position drops venous pressure 40-50 percent
- Facets and pars: stop at the medial pedicle line
- Anterior (PLL, great vessels): no blind instrumentation, check the MRI for a vascular anomaly
Complications
- Dural tear (8-15 percent): repair, sealant, no drain
- Incomplete bladder recovery (30-50 percent): ISC, urology, urodynamics at 6 weeks
- Nerve root injury (1-3 percent), haematoma (1-2 percent), infection (superficial 2-4 percent, deep 0.5-2 percent)
- Recurrence (5-10 percent), instability (2-5 percent), wrong level (less than 1 percent)
Exam tips
- Quote the timing studies accurately; do not quote an unsourced single-hour percentage
- Frame CES as a time-dependent emergency analogous to stroke or cord injury
- Demonstrate medicolegal awareness — document timing, neurology, consent
- Counsel for realistic residual deficits
- Anticoagulation: balance urgency against bleeding with an MDT
Background & Evidence
Epidemiology. CES is uncommon — an incidence of about 0.3-0.5 per 100,000 per year in community populations (Hoeritzauer 2020), with older estimates around 1-3 per 100,000 per year (Podnar 2007). Among patients referred with suspected CES only about 19 percent have radiologically and clinically confirmed disease, so the low prior probability never justifies delaying an emergency MRI when red flags are present. The commonest cause is disc herniation (around 45-70 percent of cases), followed by spinal stenosis, tumour, trauma and other causes; the most frequent levels are L4-5 (around 70 percent) and L5-S1 (around 20 percent). Classification. CES is stratified by the bladder examination because retention carries a worse, less time-sensitive prognosis than incomplete dysfunction. The Fraser/Srikandarajah framework underpins both counselling and the timing evidence.
- Clinical features
- Painless urinary retention with overflow incontinence, reduced anal tone, saddle anaesthesia
- Prognosis
- Worse; the timing of surgery makes no significant difference to the bladder outcome
- Clinical features
- Urinary frequency, urgency or altered sensation, but no retention
- Prognosis
- Better; operating within 24 hours of autonomic onset protects the bladder
- Clinical features
- Bilateral radiculopathy with bladder or bowel symptoms but a normal examination
- Prognosis
- Investigate and image; the findings determine management
Pathoanatomy and mechanism. Neural injury in CES is multifactorial: direct mechanical compression of the nerve roots, secondary ischaemia from compromise of the radicular and segmental arterial supply, and inflammatory cascades driven by nucleus pulposus. The conus medullaris ends at L1-L2 in about 90 percent of adults, so a lesion below that level compresses the cauda equina (lower motor neuron) roots rather than the cord itself. Outcome predictors.
- Unfavourable
- Complete painless urinary retention
- Unfavourable
- Duration more than 72 hours
- Unfavourable
- Complete saddle anaesthesia; absent bulbocavernosus reflex
- Unfavourable
- Tumour or infection; diabetes (delayed nerve recovery)
Key evidence. Ahn et al. (Spine 2000) established the 48-hour threshold and refuted the rigid 24-hour rule. Srikandarajah et al. (Spine 2015) refined it: a 24-hour target matters for the bladder outcome specifically in CES-I, while CES-R is less time-sensitive. DeLong et al. (J Neurosurg Spine 2008) warned against pooling the two groups. Korse et al. (Eur Spine J 2017) showed recovery is slow and frequently incomplete — at follow-up, micturition dysfunction persisted in 48 percent, defecation dysfunction in 42 percent and sexual dysfunction in 53 percent — underscoring the need for honest pre-operative counselling. Gleave and Macfarlane (2002) and Gardner et al. (2011) frame the medicolegal reality: CES accounts for a large share of UK spinal litigation, and delayed diagnosis is the commonest failing.
References
Cauda equina syndrome secondary to lumbar disc herniation: a meta-analysis of surgical outcomes
Meta-analysis of 322 patients; 42 of 104 studies met inclusion criteria. A statistically significant advantage to decompression within 48 hours versus beyond 48 hours for sensory, motor, urinary and rectal recovery, and no significant difference between the under-24-hour and 24-48-hour groups. Pre-operative chronic back pain and rectal dysfunction predicted a worse urinary outcome. The source of the 48-hour threshold.
Cauda equina syndrome secondary to lumbar disc herniation (CES-I versus CES-R)
Classic description of CES pathophysiology and surgical technique that introduced the CES-I (incomplete) versus CES-R (retention) distinction now used worldwide in prognostication.
Medical realities of cauda equina syndrome secondary to lumbar disc herniation
CES-I has a better prognosis than CES-R (around 70 percent versus 40 percent complete recovery). Sexual dysfunction is a common residual (about 50 percent of males). Functional outcome correlates with the pre-operative neurological status.
Timing of surgery in cauda equina syndrome with urinary retention: meta-analysis of observational studies
Meta-analysis of observational cohorts (16 of 27 studies analysable). Later surgery predicted a worse fair/poor urinary outcome (relative risk for later timing in the 1.77-2.19 range). CES-R and CES-I behave differently and must not be pooled.
Does early surgical decompression in cauda equina syndrome improve bladder outcome?
Retrospective cohort of 200 patients (61 CES-R, 139 CES-I). In CES-I, decompression within 24 hours of autonomic symptom onset significantly reduced bladder dysfunction at follow-up; in CES-R the timing (24, 48 or 72 hours) made no significant difference. The basis for a 24-hour target in CES-I specifically.
Cauda equina syndrome: what is the relationship between timing of surgery and outcome?
Medicolegal analysis of CES cases; the median delay to surgery was 29 hours and delayed diagnosis was the commonest issue. Only 20 percent achieved complete recovery in the litigation series (selection bias). Emphasises early recognition and documentation.
Cauda equina syndrome: a review of the current clinical and medicolegal position
Comprehensive medicolegal review. CES accounts for a large share of spine-related litigation in the UK; delayed diagnosis and treatment are the commonest issues.
Cauda equina syndrome: presentation, outcome, and predictors with focus on micturition, defecation and sexual dysfunction
Cohort of 75 operated patients. Recovery is slow and frequently incomplete — at second follow-up, micturition dysfunction persisted in 48 percent, defecation dysfunction in 42 percent and sexual dysfunction in 53 percent. Predictors of poor outcome: complete pre-operative retention, symptom duration more than 48 hours, absent bulbocavernosus reflex.
Epidemiology of cauda equina and conus medullaris lesions
Epidemiological study; incidence of CES around 1-3 per 100,000 per year. Disc herniation accounts for about 45 percent, then spinal stenosis (27 percent), tumour (9 percent) and trauma (7 percent). Most common levels L4-5 (70 percent) and L5-S1 (20 percent).
Cauda equina syndrome: a review of clinical progress
Comprehensive review of CES pathophysiology (compression, ischaemia, inflammation), diagnostic criteria and surgical techniques.
What is the incidence of cauda equina syndrome? A systematic review
PRISMA systematic review (26 of 1281 studies). Incidence approximately 0.3-0.5 per 100,000 per year in community populations; CES in roughly 0.27 percent of low-back-pain presentations to secondary care; only about 19 percent of adults investigated for suspected CES had confirmed disease.