Unipolar or bipolar release of the sternocleidomastoid for persistent congenital muscular torticollis · intermediate
- The deformity is a contracture of the sternocleidomastoid (SCM): the head TILTS toward the affected (tight) side and the chin ROTATES AWAY to the opposite side. The classic mnemonic is that the chin points away from the lesion. A fibrous 'sternomastoid tumour' (pseudotumour) is palpable within the muscle belly in early infancy in a subset of cases.
- Always screen for associated conditions before labelling it muscular: developmental dysplasia of the hip (DDH) co-exists in roughly 5-20% of cases and the hips MUST be examined and imaged; also look for metatarsus adductus and for plagiocephaly with facial hemihypoplasia on the affected side.
- Non-muscular causes must be excluded before surgery - ocular torticollis, Klippel-Feil and congenital vertebral anomalies, atlantoaxial rotatory subluxation (Grisel syndrome), posterior fossa tumour and Sandifer syndrome can all mimic CMT. A short, non-tilting, non-fibrotic 'torticollis' that does not respond to stretching is a red flag for a non-muscular cause.
- Early physiotherapy and stretching resolves the great majority (around 90% or more), especially when begun before 1 year of age. Surgery is reserved for persistent contracture, typically after age 1 year, after failed physiotherapy beyond about 12-18 months, with a residual deficit of rotation or tilt greater than about 15 degrees and a palpable tight band.
When & Why
Indication. Surgical release is reserved for the minority of infants with congenital muscular torticollis (CMT) whose contracture persists despite a genuine trial of conservative treatment. The typical criteria are: - Persistent contracture, usually addressed after age 1 year (commonly between 1 and 4 years, and before school age so facial remodelling can still occur).
- Failed physiotherapy continued for at least about 12-18 months.
- A residual deficit of rotation or lateral flexion greater than about 15 degrees.
- A persistent tight, palpable SCM band and/or established or progressing facial asymmetry. Contraindications. Any non-muscular cause not yet excluded (image first), active local infection at the operative site, or a torticollis that is still improving with conservative treatment. Exclude a non-muscular cause before ever planning a release. Operating on a non-muscular torticollis is a never-event. The mimics below all need to be considered and ruled out:
- Distinguishing features
- Tilt to compensate for strabismus or vertical squint; corrects when lying down or with eyes closed; no SCM contracture
- Action
- Ophthalmology referral; do NOT operate on the neck
- Distinguishing features
- Short webbed neck, low posterior hairline, painless restricted rotation; failed fusion or hemivertebrae
- Action
- Cervical spine radiographs; MRI; screen for renal and cardiac anomalies
- Distinguishing features
- Acute, painful 'cock-robin' posture, often after a URTI or ENT surgery; muscle is in spasm, not fibrotic
- Action
- Dynamic CT of C1-C2; treat with rest, collar, traction - not muscle release
- Distinguishing features
- Progressive tilt with neurological signs, headache, vomiting, ataxia
- Action
- Urgent MRI brain - red flag
- Distinguishing features
- Intermittent dystonic posturing related to gastro-oesophageal reflux and feeds
- Action
- Reflux assessment and treatment; resolves with reflux control
- Distinguishing features
- Recurrent self-limiting episodes of tilt in infancy, often with pallor or vomiting
- Action
- Reassurance; often migraine-associated; no surgery
A torticollis without a tight SCM band, without the typical tilt-toward and chin-away posture, or one that does not improve at all with stretching, is not CMT until proven otherwise. Image the cervical spine and consider MRI before ever planning a muscle release.
Screen for the associations. In every infant with CMT, examine and image the hips (Ortolani and Barlow; ultrasound under 6 months, radiograph after) because DDH co-exists in a clinically important proportion, and look for metatarsus adductus and other foot deformities. Plagiocephaly and facial hemihypoplasia on the affected side are markers of long-standing deformity.
DDH is the single most important association to exclude, and missing it is a classic exam and medicolegal trap. The hips MUST be examined and imaged alongside the neck assessment.
The one decision that matters. Once a true muscular contracture is confirmed, the choice is how much of the muscle to release:
Divides the sternal and clavicular heads at the inferior (clavicular) end. The workhorse for most cases of moderate contracture.
Divides the distal (sternal and clavicular) AND the proximal (mastoid) ends. Reserved for severe or long-standing contracture, the older child, or a very tight band.
Divides the distal heads through small ports. Selected centres only; offers a cosmetic incision benefit but requires specific expertise and equipment.
Lengthens rather than completely divides the muscle, used to preserve the sternal-head neck contour in carefully selected cases.
Consent specifically for recurrence or under-correction (the most common problem), neurovascular injury at the inferior release (carotid sheath, great veins) or the superior release (spinal accessory nerve, marginal mandibular branch of the facial nerve), an unsightly or hypertrophic scar with possible loss of the normal neck contour, and - critically - the likelihood that established facial asymmetry and plagiocephaly will only partly remodel if the child presents late.
The Operation
The goal is to lengthen the contracted SCM and restore a full, symmetrical range of cervical rotation and lateral flexion while protecting the deep neurovascular structures. For most cases a unipolar distal release of both heads is performed; a proximal (mastoid) release is added (making it a bipolar release) for severe or residual contracture. The exposure is laid out in full as the first steps below.
Operative sequence - unipolar distal release (with optional bipolar extension)
- Position: supine with a shoulder roll, the neck extended and the head rotated toward the contralateral (normal) side, so the tight SCM is placed on stretch and brought into prominence. A head ring stabilises the head.
- Anaesthesia: general anaesthesia with the airway secured and well taped to the non-operative side. Avoid a long-acting muscle relaxant if facial nerve monitoring is desired during a high (mastoid) dissection.
- Preparation: prep and drape the whole hemi-neck from mandible to clavicle, including the mastoid if a bipolar release is planned, with the ear and angle of the mandible visible as landmarks.
- Mark a transverse incision about 1-2 finger-breadths above the clavicle, within a natural skin crease, centred over the two heads of the SCM. A low, crease-line incision gives the best scar.
- Keep it low and transverse: an incision placed too high or too anterior risks the marginal mandibular branch of the facial nerve, and an incision directly on the clavicle gives a poor, tethered scar.
- Incise skin and platysma in the line of the marked crease.
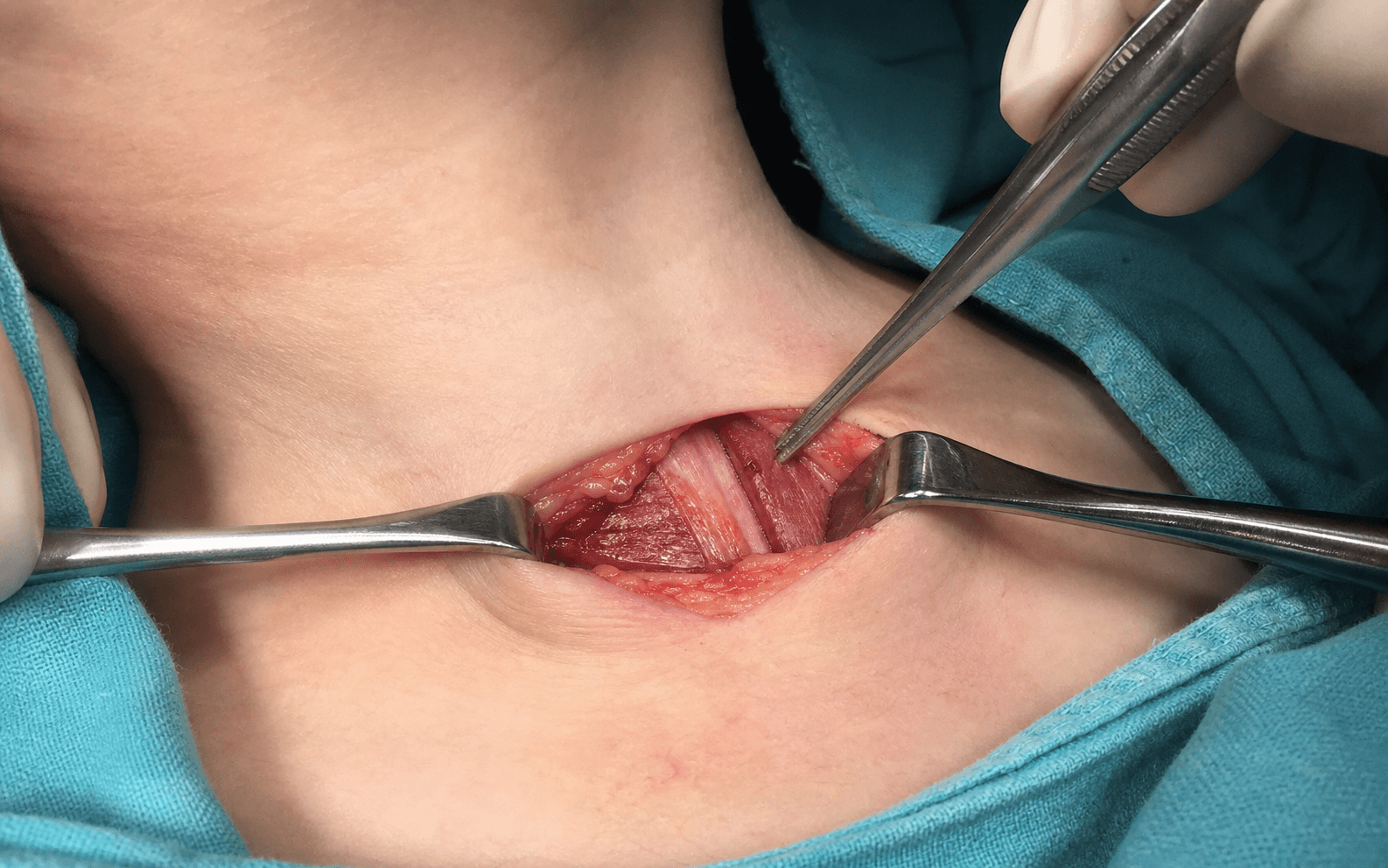
- Identify the two distinct heads of the SCM: the rounded, tendinous sternal head medially and the flatter, fleshy clavicular head laterally.
- Define the border between the two heads and elevate them in the subplatysmal plane so each can be controlled individually.
- Pass a blunt instrument (a clamp or right-angle) deep to each head, staying on the muscle and lifting it away from the floor of the neck. This isolates each head and protects the carotid sheath and jugular veins lying deep and medial.
- Never plunge deep to the muscle - the carotid sheath (carotid artery, internal jugular vein, vagus) lies immediately deep and medial, and the external and anterior jugular veins cross the field and should be identified, ligated or coagulated rather than avulsed.
- With each head isolated and protected over the clamp, divide it transversely under direct vision. Typically about 1-2 cm of muscle or tendon is resected or divided so the ends retract and do not simply re-adhere.
- Divide BOTH the sternal and the clavicular heads completely. An incomplete release of one head is a common cause of recurrence.
- After dividing the heads, rotate and tilt the head into the corrected and slightly over-corrected position.
- Palpate for any residual tight bands of deep cervical fascia or remaining muscle fibres and divide them until the neck moves freely.
- Confirm full passive rotation toward the tight side and full lateral flexion away from it, achieving over-correction.
- If a significant deficit persists despite a complete distal release - particularly in an older child or a very tight muscle - proceed to a proximal (mastoid) release (Step 8).
- Through a separate small transverse incision in a skin crease just below the mastoid process, expose the SCM insertion onto the mastoid and divide the tendinous insertion close to the bone.
- The spinal accessory nerve (CN XI) enters the deep surface of the upper SCM - stay on the tendinous insertion close to the mastoid bone and avoid deep dissection high on the muscle. The facial nerve (marginal mandibular branch) and the great auricular nerve are nearby superficially, so keep the incision low and handle tissue gently.
- Achieve haemostasis - the open neck veins can ooze.
- Close platysma and skin with absorbable subcuticular sutures for the best scar. A small drain may be used if oozing is significant.
- Apply a soft dressing, then maintain the corrected posture.
The carotid sheath (common carotid artery, internal jugular vein and vagus nerve) lies immediately deep and medial to the sternal and clavicular heads at the level of the inferior release. Plunging deep to the muscle during the clavicular or sternal release can injure the great vessels. Isolate each head over a protected clamp, stay on the muscle, divide under direct vision with the deep structures shielded by a retractor, and control the crossing external and anterior jugular veins deliberately rather than avulsing them.
CN XI enters the deep surface of the SCM in the upper third and emerges at the posterior border near Erb's point. At a superior (mastoid) release in a bipolar procedure, aggressive dissection high on the muscle risks the nerve and a subsequent trapezius palsy with shoulder droop. Stay close to the mastoid bone and divide only the tendinous insertion; consider nerve monitoring, and keep the superior incision low and transverse to protect the marginal mandibular branch of the facial nerve.
After the release, always take the head to the over-corrected position and confirm that rotation and lateral flexion are full and symmetrical. Any residual block means a remaining band - find and divide it before closing, because under-correction is the main cause of recurrence.
Confusing which way the head tilts and the chin turns determines the operative side. The contracted SCM pulls the mastoid toward the sternoclavicular joint, so the head TILTS toward the affected (tight) side and the chin ROTATES AWAY. Operate on the side TOWARD which the head is tilted (the short, tight muscle), not the side the chin points to.
Aftercare & Complications
Rehabilitation. The release is only half the treatment - maintaining the correction is essential to prevent recurrence. | Phase | Element | Typical approach | |-------|---------|------------------| | Early (days to weeks) | Corrected positioning | Hold the head in the over-corrected posture; a soft collar, TOT collar or moulded orthosis may maintain correction | | Early | Passive stretching | Begin gentle caregiver-delivered stretching once the wound is comfortable | | Ongoing (several months) | Structured physiotherapy | Daily stretching to maintain rotation and lateral flexion; night bracing in the corrected posture in selected children | | Ongoing | Active correction | Positioning and play to encourage active correction as the child grows | | Healing | Scar care | Scar massage and silicone once healed | Most children return to normal activity within a few weeks, but a committed stretching and bracing programme continues for several months.
- Structure at risk
- Carotid sheath - carotid artery, internal jugular vein, vagus nerve
- Consequence of injury
- Catastrophic haemorrhage; vagal injury (hoarseness, bradycardia)
- Protection
- Isolate each head over a protected clamp; never dissect deep to the muscle
- Structure at risk
- External and anterior jugular veins
- Consequence of injury
- Troublesome bleeding; rare air embolism
- Protection
- Identify, ligate or coagulate; avoid avulsion; control before head-up positioning
- Structure at risk
- Spinal accessory nerve (CN XI)
- Consequence of injury
- Trapezius palsy, shoulder droop, weak abduction
- Protection
- Stay on the tendinous insertion close to the mastoid; avoid deep high dissection
- Structure at risk
- Facial nerve - marginal mandibular branch
- Consequence of injury
- Lower-lip asymmetry, drooping of the corner of the mouth
- Protection
- Keep the superior incision low; gentle retraction near the mandibular angle
- Structure at risk
- Great auricular nerve
- Consequence of injury
- Numbness of the lower ear and angle of the jaw
- Protection
- Recognise it crossing the SCM; preserve where possible
- Structure at risk
- Phrenic nerve (on the scalenes, deep)
- Consequence of injury
- Hemidiaphragm paralysis (rare with a deep low dissection)
- Protection
- Stay superficial on the muscle; do not dissect the deep neck floor
- Incidence
- Most common; higher in older children and after incomplete release
- Recognition
- Persistent or returning head tilt and rotation deficit after surgery
- Prevention and management
- Prevention: divide BOTH heads completely, release residual bands, achieve over-correction on the table, add a proximal release for severe cases, commit to post-op stretching and bracing. Management: physiotherapy and bracing first; revision release with a proximal release if a definite residual band persists
- Incidence
- Rare but catastrophic
- Recognition
- Major intra-operative bleeding; postoperative hoarseness or swallowing change (vagus)
- Prevention and management
- Prevention: isolate each head over a protected clamp, divide under direct vision, never plunge deep to the muscle. Management: immediate vascular control, vascular and ENT input as required
- Incidence
- Uncommon (risk at the proximal or mastoid release)
- Recognition
- Trapezius weakness, shoulder droop, loss of full shoulder abduction
- Prevention and management
- Prevention: stay on the tendinous insertion close to the mastoid, avoid deep high dissection; consider nerve monitoring. Management: observation for neurapraxia; physiotherapy; exploration if a sharp division is suspected
- Incidence
- Uncommon (superior incision)
- Recognition
- Asymmetry of the lower lip or corner of the mouth
- Prevention and management
- Prevention: keep the superior incision low and transverse, gentle retraction near the mandibular angle. Management: most neurapraxias recover; refer if persistent
- Incidence
- Variable
- Recognition
- Visible transverse neck scar; loss of the normal sternal-head 'V' contour at the base of the neck
- Prevention and management
- Prevention: low crease-line incision, subcuticular closure; consider Z-lengthening to preserve the sternal-head contour. Management: scar massage, silicone, occasionally scar revision
- Incidence
- Common if treated late
- Recognition
- Persistent hemifacial hypoplasia and skull flattening despite a successful release
- Prevention and management
- Prevention: treat early - facial remodelling potential declines with age. Management: limited late remodelling; counsel parents pre-operatively that late surgery corrects motion, not established facial changes
- Incidence
- Low
- Recognition
- Neck swelling, pain, erythema, fever
- Prevention and management
- Prevention: meticulous haemostasis of neck veins, sterile technique, selective drain. Management: evacuate a significant haematoma (airway concern); antibiotics for infection
Viva & Exam Focus
TORTICOLLISTORTICOLLIS - assessing the infant
RELEASERELEASE - operative principles of SCM release
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 4-week-old infant is referred with a head tilt. The mother noticed a firm lump in the side of the neck. On examination the head is tilted to the right and the chin points to the left, with a firm fusiform swelling in the right sternocleidomastoid. How do you assess and manage this child?”
“A 3-year-old child has a persistent right-sided congenital muscular torticollis. Despite a supervised stretching programme since infancy, there is a fixed head tilt with a tight palpable band and a rotation deficit of about 25 degrees, plus early facial asymmetry. You decide to operate. Talk me through your surgical plan and the structures you must protect.”
“A 2-year-old is referred with a head tilt that the GP has labelled 'torticollis'. The neck moves through a full painless range, there is no palpable tight band, and the tilt seems to vary - it disappears when the child lies down. What is your approach?”
Key diagnosis points
- Head TILTS toward the tight (affected) SCM; chin ROTATES AWAY to the opposite side
- Sternomastoid tumour (pseudotumour of infancy) is benign fibrosis, not a neoplasm, and usually resolves
- Examine AND image the HIPS in every infant - DDH is the key association
- Other associations: metatarsus adductus, plagiocephaly, facial hemihypoplasia
- Exclude non-muscular causes before labelling it muscular
Differential diagnosis (exclude first)
- Ocular torticollis - corrects when lying down or eyes closed; ophthalmology referral
- Klippel-Feil or vertebral anomaly - short neck, low hairline; cervical radiographs; screen renal and cardiac
- Atlantoaxial rotatory subluxation (Grisel) - acute, painful 'cock-robin', post-URTI or ENT; dynamic CT C1-C2
- Posterior fossa tumour - progressive tilt with neurological signs; urgent MRI brain
- Sandifer syndrome - dystonic posturing with reflux; benign paroxysmal torticollis - recurrent episodes
Non-operative treatment (first-line)
- Early physiotherapy and stretching resolves around 90% or more, best before 1 year
- Passive stretch: lateral flexion AWAY from the tight side, rotation TOWARD it
- Positioning, tummy time and environmental modification
- Plagiocephaly: repositioning first; a moulding helmet for persistent moderate-severe deformity
- TOT collar as an adjunct in older infants with residual tilt
Indications for surgery
- Persistent contracture, usually after age 1 year (commonly 1-4 years)
- Failed physiotherapy continued for about 12-18 months
- Residual rotation or tilt deficit greater than about 15 degrees with a tight palpable band
- Established or progressing facial asymmetry
- Always exclude a non-muscular cause before operating
Operative technique - key steps
- Operate on the tight side (the side the head tilts TOWARD)
- Position supine, shoulder roll, head rotated to the normal side to stretch the SCM
- Low transverse crease incision two finger-breadths above the clavicle
- Identify the sternal and clavicular heads; isolate each over a protected clamp
- Divide BOTH heads completely (unipolar distal release); excise a short segment
- Add a proximal (mastoid) release for severe or older cases (bipolar release)
- Confirm over-correction with full passive rotation and lateral flexion before closure
- Subcuticular closure; maintain correction post-op with stretching and bracing
Danger zones
- Inferior release: carotid sheath (carotid artery, IJV, vagus) deep and medial - never dissect deep to the muscle
- Inferior release: external and anterior jugular veins - ligate or coagulate, avoid avulsion
- Superior (mastoid) release: spinal accessory nerve (CN XI) - stay on the tendinous insertion near the mastoid
- Superior release: facial nerve marginal mandibular branch - keep the incision low
- Great auricular nerve at the superior incision; phrenic nerve deep in the neck floor
Complications
- Recurrence or under-correction - most common; complete the release and maintain correction
- Neurovascular injury (carotid sheath or great veins) - rare but catastrophic
- Spinal accessory nerve injury - trapezius palsy, shoulder droop (proximal release)
- Facial nerve (marginal mandibular) injury - lower-lip asymmetry (superior incision)
- Unsightly scar or loss of neck contour; residual facial asymmetry if treated late
Outcomes and counselling
- Best results when treated young - facial and skull remodelling potential declines with age
- A complete release plus disciplined post-op stretching and bracing gives good correction in most
- Established facial asymmetry may only partly remodel after late surgery
- Main cause of a poor outcome: late presentation; main technical cause of recurrence: incomplete release
- Counsel parents that surgery corrects motion, not necessarily established facial changes
Background & Evidence
Aetiology and pathology. Congenital muscular torticollis is the most common cause of torticollis in infancy. The primary lesion is fibrosis and contracture of the sternocleidomastoid muscle. Several theories exist for the cause, and more than one may apply: - Intrauterine crowding or packaging - abnormal foetal position, supported by the association with breech presentation, primigravida mothers and oligohydramnios.
- Compartment syndrome or ischaemia - localised ischaemia of the SCM leading to fibrosis, consistent with the histology of the sternomastoid tumour.
- Birth trauma - historically proposed, but CMT also occurs after uncomplicated and caesarean deliveries.
- Hereditary or connective tissue factors - a minority show a familial pattern. The sternomastoid tumour (pseudotumour of infancy). A firm, mobile, fusiform swelling within the SCM belly, typically appearing in the first few weeks of life and usually resolving over months. Histology shows fibroblast proliferation and collagen deposition replacing muscle - it is NOT a neoplasm. Its presence is associated with a tighter contracture and a slightly higher rate of needing surgery, but most still resolve with physiotherapy. The classic posture and pathoanatomy. The contracted SCM shortens the distance between the mastoid process and the sternoclavicular joint, producing a head tilt toward the affected (tight) side and chin rotation away to the opposite side. Long-standing deformity drives plagiocephaly (skull flattening) and facial hemihypoplasia on the affected side. One operates on the side toward which the head is tilted (the short, tight muscle). Non-operative management is the cornerstone. Early conservative treatment resolves the great majority of cases. The programme combines passive stretching (gentle, sustained lateral flexion away from the tight side and rotation toward it, taught to caregivers for daily home practice), active positioning (toys, cot and feeding arranged to encourage rotation toward the tight side and tilt away from it), tummy time (neck strengthening and plagiocephaly prevention), and environmental modification. Plagiocephaly is managed with repositioning first, with a cranial moulding helmet reserved for persistent moderate-severe deformity within the window of rapid skull growth, and a TOT (tubular orthosis for torticollis) collar is an adjunct in older infants with residual tilt.
- Favourable (better non-operative outcome)
- Younger, especially under 3-6 months
- Unfavourable (higher chance of surgery)
- Older, especially after 1 year
- Favourable (better non-operative outcome)
- Small deficit (less than about 15 degrees)
- Unfavourable (higher chance of surgery)
- Large fixed deficit
- Favourable (better non-operative outcome)
- Absent or small
- Unfavourable (higher chance of surgery)
- Dense palpable pseudotumour or fibrotic band
- Favourable (better non-operative outcome)
- Responds within months
- Unfavourable (higher chance of surgery)
- Persisting beyond about 12-18 months
- Favourable (better non-operative outcome)
- Absent
- Unfavourable (higher chance of surgery)
- Established hemihypoplasia or plagiocephaly
Outcomes. The best results are achieved when treatment - operative or not - is undertaken young, because the potential for facial and skull remodelling declines with age. A complete release combined with a committed post-operative stretching and bracing programme gives good correction of head posture and rotation in the majority. Established facial asymmetry and plagiocephaly may improve only partially after late surgery: the deformity of motion is corrected, but the structural facial changes may persist. The main determinant of a poor outcome is late presentation or treatment; the main technical determinant of recurrence is an incomplete release combined with a failure to maintain correction.
Early non-operative treatment cures most children and prevents facial asymmetry. When surgery is needed, a complete release plus a disciplined stretching and bracing programme gives a good result - but if the child presents late, counsel the family that neck movement can be restored while the established facial asymmetry may only partly remodel.
References
The clinical presentation and outcome of treatment of congenital muscular torticollis in infants - a study of 1,086 cases
Large cohort defining the presentation, the sternomastoid tumour subtype and the excellent outcomes achievable with early manual stretching.
Clinical determinants of the outcome of manual stretching in the treatment of congenital muscular torticollis in infants - a prospective study of 821 cases
Prospective study identifying the prognostic factors that predict success or failure of conservative management.
Physical therapy management of congenital muscular torticollis - a 2018 evidence-based clinical practice guideline
Evidence-based clinical practice guideline for the non-operative management of congenital muscular torticollis.
Ultrasonographic study of the coexistence of muscular torticollis and dysplasia of the hip
Documents the coexistence of congenital muscular torticollis and developmental dysplasia of the hip, supporting routine hip screening.
Change of craniofacial deformity after sternocleidomastoid muscle release in pediatric patients with congenital muscular torticollis
Demonstrates partial remodelling of craniofacial deformity after release and the influence of age at surgery on the cosmetic outcome.
Muscular torticollis - a modified surgical approach
Describes the bipolar release technique and the surgical principles for resistant congenital muscular torticollis.