Plantar-based racquet flap · disarticulation through the talonavicular and calcaneocuboid joints · advanced
- Chopart amputation is disarticulation through the transverse tarsal joint - the talonavicular joint medially plus the calcaneocuboid joint laterally - preserving the talus and calcaneus.
- The dominant complication is equinoVARUS deformity: Achilles overpull (equinus) plus unopposed tibialis posterior against the lost peroneus brevis (varus). Tendon balancing at the index operation roughly halves the wound-failure rate (46 percent conventional versus 28 percent modified Chopart).
- The racquet incision uses a LONG plantar flap and a SHORT dorsal flap. The plantar skin is sensate, thick and durable - ideal for weight-bearing - and the medial and lateral plantar nerves MUST be preserved for protective sensation.
- Healing requires adequate perfusion: TcPO2 greater than 30mmHg and ankle-brachial index greater than 0.5 (many units target TcPO2 over 40mmHg). Revascularise first if marginal, otherwise choose a higher level.
- Balancing is mandatory, not optional: Achilles lengthening for equinus PLUS tibialis anterior transfer to the talar neck for varus; a talocalcaneal (subtalar) arthrodesis is the alternative for a rigid or recurrent deformity.
- Many surgeons now prefer a balanced (modified) Chopart, a Pirogoff or Syme stump, or a primary transtibial amputation over a conventional un-balanced Chopart, given the high wound-failure, deformity and revision rates.
When & Why
Indication. A Chopart amputation is performed when the forefoot must be sacrificed but the hindfoot (talus and calcaneus) is viable, perfused and free of infection - the aim being to preserve a sensate, weight-bearing stump at the most distal level that will reliably heal. Absolute indications are severe irreparable forefoot trauma with a viable hindfoot; diabetic forefoot gangrene or osteomyelitis with intact hindfoot perfusion; a malignant forefoot tumour requiring negative margins; multiple failed ray amputations leaving a non-functional forefoot remnant; and chronic forefoot osteomyelitis unresponsive to medical and surgical management. Relative indications include severe Charcot forefoot deformity with irreparable midfoot collapse, a congenital forefoot deformity requiring reconstruction, extensive forefoot soft-tissue loss with exposed bone, and peripheral vascular disease where a more distal amputation would be inadequate. Contraindications are the conditions that make the hindfoot stump fail: inadequate perfusion (TcPO2 less than 30mmHg or ABI less than 0.5), active hindfoot infection or osteomyelitis, an ischaemic heel or Achilles region, severe PVD mandating a higher level, a non-ambulatory patient (a transtibial amputation fits a prosthesis better), and a psychiatric or cognitive inability to cooperate with prolonged rehabilitation. The level-selection decision. Once the forefoot is lost and the hindfoot is viable, the real choice is which hindfoot-preserving level gives this patient the best function. Each option trades stump length against prosthetic reliability:
Most distal level; preserves talus and calcaneus. Sensate plantar weight-bearing surface, but a short lever arm and a strong tendency to equinoVARUS. Needs tendon balancing plus long-term AFO or prosthesis.
Ankle disarticulation with a heel flap (Pirogoff preserves the calcaneus tilted up onto the tibia; Syme removes it). Better prosthetic fit and a longer lever arm than Chopart, at the cost of the ankle joint.
Most reliable prosthetic ambulation and the longest lever arm. Preferred for the non-ambulatory or severely dysvascular patient in whom a Chopart stump will not heal or function.
Guidelines, registries and global practice. Across the IWGDF (International Working Group on the Diabetic Foot), AOFAS and BOA/BOAST limb-loss guidance the principle is the same: amputate at the most distal level that will reliably heal while delivering a functional, prosthetically fittable limb. There is no implant registry for amputation; the evidence is case series and systematic reviews. - Perfusion thresholds. Healing is unlikely with TcPO2 under 30mmHg or ABI under 0.5; many vascular units target TcPO2 over 40mmHg or toe pressure over 30mmHg at the proposed level before committing. Restore inflow first if marginal.
- Antibiotic prophylaxis. A first-generation cephalosporin (cefazolin 2g IV, 3g if over 120kg) within 60 minutes of incision is standard; add MRSA cover (vancomycin or teicoplanin) where colonisation or local prevalence is high. For established diabetic foot infection give culture-directed therapeutic antibiotics per IWGDF/IDSA rather than prophylaxis alone.
- Practice variation. In high-resource settings with ready prosthetics and vascular support, a balanced (modified) Chopart or a primary transtibial amputation are both reasonable; in lower-resource settings a heel-bearing midfoot stump or a Pirogoff/Syme stump that allows barefoot household ambulation without a prosthesis may be preferred. The level must match the patient's rehabilitation and prosthetic ecosystem. Consent specifically for wound breakdown or flap necrosis, an insensate stump if the plantar nerves are injured, progressive equinoVARUS deformity, phantom-limb pain, the high likelihood of long-term AFO or prosthesis use, and a 20 to 40 percent chance of revision to a higher level within five years. Setup. Supine with an ipsilateral hip bump (30 degrees internal rotation), thigh tourniquet (inflate to 250 to 300mmHg for the lower extremity), the foot off the end of the table or on a radiolucent support. Prep from tourniquet to toes. Fluoroscopy is helpful to mark the talonavicular and calcaneocuboid joints.
The Operation
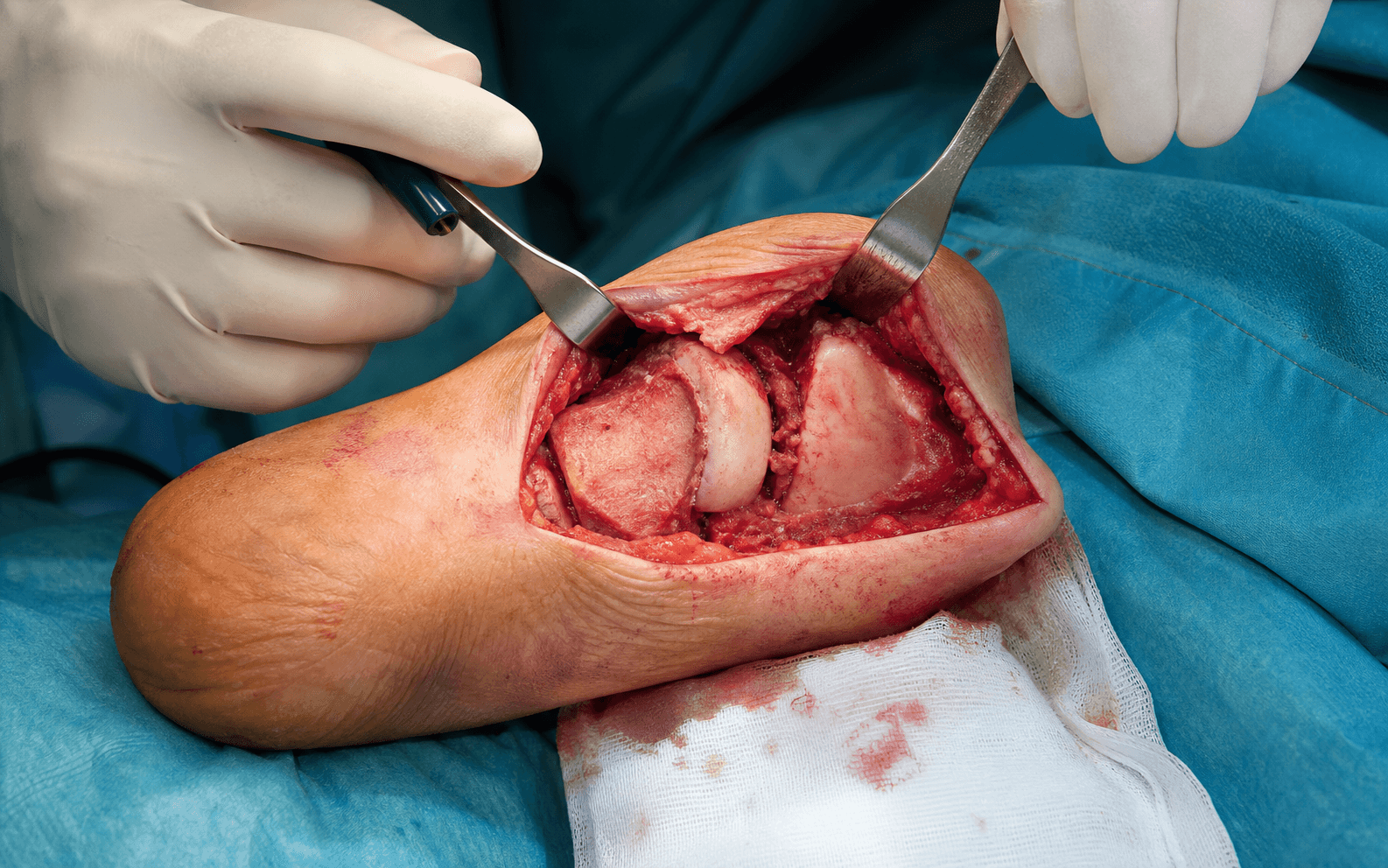
The goal: confirm perfusion, design a long plantar racquet flap, disarticulate cleanly through the talonavicular and calcaneocuboid joints while protecting the dorsalis pedis and the medial and lateral plantar neurovascular bundles, balance the tendons to prevent equinoVARUS, and close a tension-free, sensate flap over smooth bone with the foot splinted in neutral. The exposure - the racquet incision and the step-by-step protection of the plantar bundle - is laid out in full below; it is the heart of the operation.
Operative sequence
- Supine, hip bump, thigh tourniquet, foot off the end of the table; fluoroscopy available.
- Confirm feasibility before cutting: palpate dorsalis pedis and posterior tibial pulses, check TcPO2 greater than 30mmHg and ABI greater than 0.5 at the proposed level, and assess skin quality, temperature and capillary refill. If perfusion is marginal, stop and arrange revascularisation or a higher level.
- Palpate and mark the talonavicular joint medially and the calcaneocuboid joint laterally (fluoroscopy confirms); mark the plantar flap to the metatarsal-head level so it will reach the dorsum without tension.
- Transverse dorsal limb across the talonavicular and calcaneocuboid joints.
- Medial and lateral extensions curve distally along the midfoot borders onto the plantar surface.
- Plantar limb at the distal forefoot (metatarsal-head level): the plantar flap is LONG (6 to 8cm from the transverse tarsal joint) and the dorsal flap is SHORT (1 to 2cm) and largely discarded.
- The long plantar flap will rotate dorsally to cover talus and calcaneus; it must reach without any tension - a short flap is the commonest cause of failure.
- Incise the dorsal skin and deepen through subcutaneous fat to the extensor retinaculum.
- Identify the dorsalis pedis artery running between EHL (medial) and EDL (lateral) with the deep peroneal nerve; protect it meticulously - it supplies the dorsal skin and its injury causes dorsal necrosis.
- Identify and tag the extensor tendons - tibialis anterior (most medial), EHL, EDL and peroneus tertius if present - then divide them sharply under direct vision and retract proximally to expose the talonavicular and calcaneocuboid capsules. The tagged TA will be re-routed to the talar neck later.
- Extend the medial limb distally along the medial border of the foot and deepen through skin and subcutaneous tissue.
- Identify the tibialis posterior tendon on the navicular tuberosity (the medial midfoot prominence) and divide it sharply, but do not avulse it (bleeding).
- The critical structure of the whole operation - the medial plantar neurovascular bundle: it branches from the posterior tibial artery and nerve about 1cm distal to the medial malleolus and runs 15 to 20mm from the medial plantar border, deep to skin and fat but superficial to the flexor tendons. It is the primary blood supply and the primary sensation of the plantar flap. Dissect superficial to it and preserve it within the full thickness of the flap.
- Extend the lateral limb distally along the lateral border of the foot.
- Identify and divide the peroneal tendons: peroneus brevis on the fifth metatarsal base (the key everter) and peroneus longus crossing plantarward to the first cuneiform.
- Protect or sharply divide the sural nerve along the lateral border (lateral foot sensation).
- Identify and preserve the lateral plantar neurovascular bundle lateral to FDL and deep to the plantar aponeurosis; it gives calcaneal branches for heel sensation and must stay within the flap.
- Identify the talonavicular joint capsule medially and the calcaneocuboid joint capsule laterally - together the transverse tarsal (Chopart) joint.
- Incise both capsules circumferentially and plantarflex the foot to open the joints.
- Disarticulate the navicular from the talar head and the cuboid from the calcaneus, and remove the navicular, cuboid and entire forefoot en bloc.
- Preserve the articular cartilage of the talar head and calcaneus (avoid gouging) if the joint is to be kept for motion; these same surfaces can later be prepared for arthrodesis.
- Incise the plantar skin at the marked distal level and raise the flap as a composite of skin, subcutaneous fat, plantar aponeurosis and the medial and lateral plantar neurovascular bundles.
- Divide FHL and FDL tendons distally, preserving their proximal stumps.
- Release the tourniquet briefly to confirm brisk flap bleeding and capillary refill; Doppler the plantar arteries.
- Trim excess fat so the flap lies flat, but do NOT thin it excessively - the vascular plexus and the nerves must be preserved for padding and protective sensation.
- Equinus occurs in 30 to 50 percent from Achilles overpull after loss of the dorsiflexors; address it at the index operation, do not wait and see.
- Z-plasty (open): 3cm posteromedial incision, proximal medial and distal lateral hemisections 3 to 4cm apart; dorsiflex the foot to neutral with the knee flexed and repair the tendon.
- Percutaneous triple hemisection: three 1cm stab incisions (proximal medial, middle lateral, distal medial); dorsiflex to neutral and allow healing with lengthening.
- Lengthen until the foot rests at neutral (90 degrees) with the knee extended - typically 2 to 3cm. Over-lengthening causes calcaneus gait; under-lengthening fails to prevent equinus.
- This corrects the VARUS that Achilles lengthening alone leaves behind, by centralising the dorsiflexion pull over the talus and abolishing the unopposed inversion.
- Use the tagged tibialis anterior tendon (EDL/EHL may be co-tenodesed to it); drill a tunnel in the talar neck dorsal to the articular surface, or use a suture anchor or interference screw.
- Tension the transfer with the foot in neutral dorsiflexion and slight eversion; add a peroneal balancing transfer laterally (to calcaneus or talus) where the varus pull is strong.
- Systematic-review data show that modified (balanced) Chopart stumps heal far more reliably than conventional ones.
- The most definitive equinus prevention - fusing the subtalar joint creates a stable platform and is increasingly used, especially for a rigid or recurrent deformity.
- Debride the talar and calcaneal subtalar cartilage to bleeding subchondral bone, position the hindfoot in 5 degrees of valgus and neutral dorsiflexion, and fix with one or two cannulated screws (6.5 to 7.3mm) from calcaneus into talus, bone-grafting from the resected navicular or cuboid.
- Costs: 30 to 45 minutes extra operative time, a 10 to 15 percent nonunion risk, and 10 to 12 weeks of protected weight-bearing.
- Use a rongeur to smooth the talar head and the calcaneal cuboid surface, removing any sharp edge or prominence that would ulcerate through the flap.
- If the joint is preserved, smooth the edges without violating subchondral cartilage; if arthrodesis was performed, ensure adequate bleeding-bone apposition.
- Bring the plantar flap dorsally and confirm it lies flat over smooth bone with no bony prominence palpable.
- Release the tourniquet completely, allow about 10 minutes for pressure to re-establish, and achieve bone-dry hemostasis - bipolar for small vessels, suture ligation for larger ones, avoiding electrocautery near the plantar nerves. A haematoma is a major cause of flap failure.
- Place a deep drain beneath the flap, exiting lateral or medial to the incision (never through the flap or the neurovascular bundle); remove at 24 to 48 hours.
- Anchor the plantar aponeurosis to dorsal periosteum and tendon stumps with 2-0 absorbable sutures to prevent distal flap migration and keep sensate skin over the weight-bearing talus and calcaneus. The flap must lie flat without any tension.
- Close in layers: 3-0 absorbable subcutaneous sutures to reduce dead space with no tension, then interrupted nylon or staples approximating the plantar flap edge to the dorsal skin (leave 1 to 2mm gaps if oedematous).
- Dress with non-adherent gauze, fluffed padding and a soft wrap - loose, no circumferential constriction.
- Apply a posterior splint from toes to knee with the foot at neutral (90 degrees), never plantarflexed, and the knee at 30 degrees flexion to reduce Achilles tension. Splinting in plantarflexion encourages equinus contracture.
The medial plantar artery and nerve are the primary blood supply and the primary sensation of the weight-bearing flap; the lateral bundle carries heel sensation via its calcaneal branches. Identify them early in the medial and lateral dissection, dissect superficial to them, and carry them within the full thickness of the flap. Do not thin the flap, do not place electrocautery near the nerves, and do not pass a drain through the bundle. Injury makes the stump ischaemic or insensate - an insensate weight-bearing surface ulcerates repeatedly and usually ends in revision to a higher level.
Lengthen until the foot rests at neutral (90 degrees) with the knee extended and there is no resistance to passive dorsiflexion - typically 2 to 3cm. The examiner will ask exactly this. Over-lengthening produces a calcaneus gait with weak push-off; under-lengthening fails to prevent equinus and you will be back.
The residual deformity is equinoVARUS, not pure equinus. Lengthening the Achilles fixes the equinus but leaves the varus - unopposed tibialis posterior against the lost peroneus brevis. Unless you also transfer the tibialis anterior to the talar neck (and add a peroneal transfer if the varus pull is strong), the stump inverts, weight shifts onto the old cuboid region, and the lateral or plantar skin breaks down. Balancing roughly halves the wound-failure rate (46 percent conventional versus 28 percent modified Chopart).
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation and wound | Milestone | |-------|--------|--------------------------|-----------| | Immediate | 0 to 2 weeks | Bulky padded dressing and posterior splint, foot at neutral, knee at 30 degrees flexion | Hospital 3 to 5 days, strict non-weight-bearing, drain out at 24 to 48 hours, PCA or epidural then oral analgesia, enoxaparin 40mg SC daily, glucose 6 to 10 mmol/L in diabetics | | Early | 2 to 6 weeks | Posterior splint in neutral, changed weekly to watch for equinus | Non-weight-bearing, sutures out at 3 to 4 weeks, serial casting if equinus develops, upper-body and transfer training | | Intermediate | 6 to 12 weeks | Custom AFO | Gradual weight-bearing from 6 to 8 weeks if healed, union check at 10 to 12 weeks if arthrodesis, prosthetic consultation, gait training | | Long-term | 3 months onward | AFO long-term in about 80 percent, plus prosthesis or shoe filler | Review 3-monthly then 6-monthly; monitor for equinus, skin breakdown and ulceration | Most patients return to household ambulation over several months; about 80 percent need a long-term AFO and 20 to 40 percent require revision to a higher level within five years. Red flags requiring urgent review: flap discoloration (dusky, blue or black), wound dehiscence with bone exposure, fever or systemic sepsis, progressive equinus deformity, new pressure ulceration, or uncontrolled pain. Complications
- Recognition
- Progressive plantarflexion and inversion contracture over weeks to months; weight shifts onto the lateral or distal stump; inability to reach neutral
- Prevention
- Tendon balancing at the index operation - Achilles lengthening plus tibialis anterior transfer to the talar neck, plus a peroneal transfer if varus is strong; splint in neutral, serial casting, early AFO
- Management
- Mild and flexible: serial casting, AFO, stretching. Moderate or recurrent: revise the tendon balancing. Rigid or severe: subtalar or tibiotalocalcaneal arthrodesis, or revision to Syme or transtibial
- Recognition
- Skin-edge separation, exposed bone or tendon, dusky flap, absent capillary refill; usually within 7 to 14 days
- Prevention
- Confirm perfusion preoperatively (TcPO2 greater than 30mmHg); long plantar flap without tension; meticulous hemostasis; protect the plantar arteries; non-weight-bearing healing
- Management
- Partial: local wound care, debridement, secondary healing or delayed closure. Complete: revision to a higher level (Syme or transtibial), with negative-pressure therapy as a bridge
- Recognition
- Absent protective sensation on the plantar surface on monofilament testing; patient reports numbness; high ulceration risk
- Prevention
- Meticulous medial and lateral dissection preserving the plantar neurovascular bundles; maintain full flap thickness; avoid electrocautery near nerves
- Management
- No surgical correction; daily foot inspection education, protective footwear and custom insoles, frequent podiatry; consider transtibial revision for recurrent ulceration
- Recognition
- Wound erythema, purulent drainage, fever, raised WCC and CRP; probe-to-bone positive; marrow oedema on MRI
- Prevention
- Preoperative antibiotic prophylaxis (cefazolin 2g IV); meticulous hemostasis; drain placement; non-weight-bearing healing; glycaemic control; smoking cessation
- Management
- Superficial: oral antibiotics and local wound care. Deep or osteomyelitis: culture-directed IV antibiotics for about 6 weeks, debridement, and revision to a higher level if talus or calcaneus is infected
- Recognition
- Sensation of the forefoot still present, often painful - burning, shooting or cramping, worse at night; distinguish from stump pain
- Prevention
- Pre-emptive analgesia (epidural or nerve blocks); early mobilisation; mirror therapy; psychological preparation
- Management
- Gabapentin 300 to 900mg three times daily, amitriptyline 25 to 75mg nocte or duloxetine 60mg daily; mirror therapy, TENS, desensitisation; refractory cases to a pain clinic
- Recognition
- Skin breakdown over bony prominences (talar head, calcaneus); painful, may expose bone; usually with prosthetic or AFO use
- Prevention
- Smooth bone contouring at surgery; sensate flap; proper prosthetic fitting; pressure-relieving insoles; daily inspection
- Management
- Non-weight-bearing, local wound care and pressure relief; debride necrotic tissue; if bone is exposed, revise the contour or revise to a higher level if recurrent
- Recognition
- Unable to achieve a comfortable fit; equinus prevents a neutral foot position; short lever arm limits push-off; pain with use
- Prevention
- Prevent equinus (the primary factor); adequate stump length; sensate weight-bearing surface; early prosthetic consultation and realistic expectations
- Management
- Custom AFO; prosthetic shoe filler with a carbon-fibre plate; address any equinus; consider revision to Syme or transtibial if non-functional
Complication rates from verified series: - Wound complications: failed wound healing about 46 percent after conventional (un-balanced) Chopart versus 28 percent after modified (balanced) Chopart in systematic review; up to 94 percent with any wound complication in a dysvascular diabetic case series.
- Revision to a higher level: about 28 percent in a large diabetic series (annual incidence 13 percent); up to 56 percent in high-risk diabetic cohorts.
- Successful prosthetic ambulation: about 44 percent in a dysvascular diabetic series; higher in selected ambulatory, balanced, well-perfused patients.
- Background mortality is high in the diabetic-dysvascular population (about 46 percent over about 3 years in one series) and is driven by comorbidity, not by the operation itself. Why a conventional Chopart has fallen out of favour. Many surgeons now prefer a balanced (modified) Chopart, a Pirogoff or Syme stump, or a primary transtibial amputation over an un-balanced Chopart because of the high equinoVARUS rate, the high wound-failure rate (up to about 46 percent conventional, halved by balancing), difficulty with prosthetic fitting and a short lever arm, frequent revision to a higher level, and patient-reported function that does not improve and stays below population norms. A Chopart is still indicated when the patient specifically refuses a higher amputation, when there are religious or cultural requirements for tissue preservation, or when the surgeon is highly experienced with the technique and its deformity-prevention strategies.
Viva & Exam Focus
CHOPARTCHOPART - the hazards of a plantar-based amputation at the transverse tarsal joint
EQUINUSEQUINUS - preventing the equinoVARUS deformity
Five danger structures - know the location and the protection strategy for each:
- Location
- Between EHL and EDL, 2 to 3cm distal to the talonavicular joint on the dorsal midfoot; supplies the dorsal skin
- Protection strategy
- Identify early after the dorsal incision, gentle retraction during tendon division, preserve the adventitia, avoid electrocautery within 5mm
- Location
- Branches from the posterior tibial artery and nerve 1cm distal to the medial malleolus; runs 15 to 20mm from the medial plantar border; primary supply and sensation to the flap
- Protection strategy
- Dissect superficial to the bundle during the medial approach, preserve all plantar soft-tissue thickness, identify it before dividing the tibialis posterior tendon
- Location
- Accompanies the lateral plantar nerve lateral to FDL and deep to the plantar aponeurosis; gives calcaneal branches for heel sensation
- Protection strategy
- Keep the lateral dissection superficial to the deep fascia, protect it during peroneal tendon division, preserve the calcaneal branches
- Location
- Talar head (talonavicular joint) and the anterior and middle facets; becomes the weight-bearing surface if the joint is preserved
- Protection strategy
- Capsular dissection only; smooth the bone edges without violating subchondral bone if preserving the joint; consider arthrodesis to prevent arthrosis
- Location
- Runs with the dorsalis pedis artery between EHL and EDL; sensation to the first web space, motor to EDB
- Protection strategy
- Identify it with the dorsalis pedis, gentle retraction only, divide sharply if necessary - motor loss is acceptable, sensory loss is problematic
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old diabetic man has forefoot gangrene extending to the midfoot. You are considering a Chopart amputation. What is your preoperative assessment, and what would make you choose a higher level instead?”
“What is the major complication of a Chopart amputation and how do you prevent it at the index operation?”
“During the plantar flap dissection, what critical neurovascular structures must you preserve and why? Describe their anatomy.”
Indications
- Severe forefoot trauma or ischaemia with a viable hindfoot
- Diabetic forefoot gangrene or osteomyelitis with TcPO2 greater than 30mmHg
- Tumour requiring forefoot resection with negative margins
- Multiple failed ray amputations leaving a non-functional forefoot
- Contraindications: TcPO2 less than 30mmHg, ABI less than 0.5, hindfoot infection, a non-ambulatory patient
Key anatomy
- Transverse tarsal joint = talonavicular (medial) plus calcaneocuboid (lateral)
- Dorsalis pedis artery: between EHL and EDL, supplies the dorsal skin
- Medial plantar bundle: 15 to 20mm from the medial border - primary flap supply and sensation
- Lateral plantar bundle: with FDL, calcaneal branches to the heel
- Muscle imbalance = equinoVARUS: lost dorsiflexors versus retained Achilles (equinus); lost peroneus brevis versus retained tibialis posterior (varus)
Critical steps
- Confirm perfusion: TcPO2 greater than 30mmHg and ABI greater than 0.5 are mandatory
- Racquet incision: long plantar flap to the metatarsal heads, short dorsal flap
- Protect the dorsalis pedis during the dorsal dissection (between EHL and EDL)
- Preserve the medial and lateral plantar bundles in a full-thickness flap
- Disarticulate at the transverse tarsal joint and preserve the talus and calcaneus cartilage
- Balance: Achilles lengthening (equinus) plus tibialis anterior transfer to the talar neck (varus); arthrodesis for a rigid or recurrent deformity
- Inset the flap without tension and anchor it to prevent migration
Danger zones
- Dorsalis pedis: between EHL and EDL - protect during the dorsal dissection
- Medial plantar bundle: 15 to 20mm from the medial border - injury means an insensate stump
- Lateral plantar bundle: with FDL - calcaneal branches for heel sensation
- Talar cartilage: avoid gouging if preserving the joint for motion
- Deep peroneal nerve: with the dorsalis pedis - traction injury is possible
Technique pearls
- The plantar flap must be long enough (to the metatarsal heads) - tension equals failure
- Preserve full flap thickness (skin, fat, aponeurosis, neurovascular bundles) - padding is critical
- Balance the tendons at the index operation - balancing roughly halves wound failure (46 percent to 28 percent)
- Achieve meticulous hemostasis before closure - a haematoma compromises the flap
- Splint in neutral (90 degrees), never plantarflexion
- Hindfoot arthrodesis is an option for a rigid or recurrent equinovarus deformity
Major complications
- EquinoVARUS deformity (most common): Achilles and tibialis posterior overpull; prevented by tendon balancing
- Wound dehiscence or flap necrosis: about 46 percent conventional, 28 percent modified; up to 94 percent any wound complication in dysvascular diabetics
- Insensate stump: plantar nerve injury - catastrophic functional loss
- Infection: higher in diabetics, may require revision
- Pressure ulceration: bony prominences (especially lateral with varus), insensate skin, prosthetic issues
- Prosthetic difficulty: short lever arm, equinovarus; only about 44 percent ambulate with a prosthesis in dysvascular series
- Revision to a higher level: about 28 percent in a diabetic series, up to 56 percent in high-risk cohorts
Post-operative protocol
- Non-weight-bearing for 6 to 8 weeks, drain out at 24 to 48 hours, sutures at 3 to 4 weeks
- Posterior splint in neutral with the knee at 30 degrees flexion
- Serial casting if equinovarus develops; maintain neutral
- AFO fitting at 6 to 8 weeks, required long-term in about 80 percent
- Prosthetic consultation at 6 to 8 weeks - custom filler or prosthesis
- Monitor: flap viability, equinus development, skin breakdown, ulceration
Exam tips
- Know: Chopart = transverse tarsal joint (talonavicular plus calcaneocuboid)
- Emphasise: equinoVARUS is the major deformity - balance the tendons (Achilles lengthening plus tibialis anterior transfer) at the index operation
- State: TcPO2 greater than 30mmHg and ABI greater than 0.5 are the minimum perfusion requirements; revascularise first if marginal
- Mention: medial plantar bundle preservation is critical for a sensate weight-bearing surface
- Acknowledge: high wound-failure and revision rates; balancing roughly halves wound failure; many prefer a balanced Chopart, Pirogoff or Syme, or transtibial
- Explain: the racquet incision = long plantar (sensate, durable) plus short dorsal flap
Background & Evidence
Surgical anatomy. The transverse tarsal (Chopart) joint is formed by the talonavicular joint medially - a ball-and-socket joint that allows inversion and eversion - and the calcaneocuboid joint laterally - a modified saddle joint with more restricted motion. The two function together as the midtarsal joint complex; a Chopart amputation disarticulates through both while preserving an intact talus and calcaneus. The vascular supply to the flap comes from the medial and lateral plantar arteries (terminal branches of the posterior tibial), with the dorsalis pedis (the continuation of the anterior tibial, running between EHL and EDL) supplying the dorsal skin. The nerves that matter are the medial plantar nerve (sensation to the medial plantar weight-bearing skin - critical to preserve), the lateral plantar nerve (lateral plantar sensation and motor to the intrinsics, with calcaneal branches to the heel), the deep peroneal nerve (first web space sensation, motor to EDB) and the sural nerve (lateral border sensation). The central problem is muscle imbalance. With the forefoot gone, the insertions of the dorsiflexors and evertors are lost while the plantarflexors and invertors remain:
- Normal balance
- TA, EHL and EDL balance the Achilles
- After Chopart
- Dorsiflexors lost; Achilles unopposed
- Resulting deformity
- Equinus
- Normal balance
- Peroneus brevis balances tibialis posterior
- After Chopart
- Peroneus brevis lost; tibialis posterior unopposed
- Resulting deformity
- Varus
- Weight-bearing skin
- Sensate, thick, durable plantar skin
- Vascularity
- Medial and lateral plantar arteries - robust
- When used
- The standard primary technique
- Weight-bearing skin
- Non-plantar skin on the stump - less durable
- Vascularity
- Variable; sagittal vessels
- When used
- When dorsal or plantar tissue loss precludes a racquet flap
Key evidence. The systematic review by van der Wal (2023) showed that failed wound healing runs at about 46 percent after a conventional (un-balanced) Chopart but falls to about 28 percent after a modified (balanced) Chopart, with re-amputation to a higher level most frequent after the conventional procedure - and that modified Chopart allowed unprosthetised short-distance ambulation in 74 percent versus only 26 percent household ambulation after a conventional one. This is the quantitative basis for treating tendon balancing as integral to the operation, not optional. Brodell (2020), in a single-centre diabetic series, found that even with tendon transfers 94 percent developed a wound complication and 56 percent required revision, with only 44 percent ever ambulating with a prosthesis - a sobering reminder that in the dysvascular diabetic foot a primary transtibial amputation is often the better answer. The original rationale for balancing (Reyzelman and Armstrong, 1999) emphasised that the residual deformity is equinoVARUS, not pure equinus, and that eliminating the cuboid can paradoxically reduce varus. Faglia (2015) and Schade (2010) underline that in the dysvascular diabetic population the operation is a last-chance limb-salvage step with a high revision rate and very high background mortality, and that no single balancing or arthrodesis technique is proven superior - so the choice is individualised to soft-tissue quality and surgeon experience.
References
Lisfranc and Chopart amputation: a systematic review
- Systematic review of 16 studies. Failed wound healing was 20 percent after Lisfranc, 28 percent after MODIFIED Chopart (with tendon balancing), and 46 percent after CONVENTIONAL Chopart.
- Re-amputation to a higher level was most frequent after a conventional (un-balanced) Chopart.
- Modified Chopart allowed unprosthetised short-distance ambulation in 74 percent versus only 26 percent household ambulation after conventional Chopart.
Chopart Amputation: Questioning the Clinical Efficacy of a Long-standing Surgical Option for Diabetic Foot Infection
- Single-centre case series of 18 diabetic patients (Chopart with tendon transfers), mean follow-up 22.8 months.
- 17 of 18 patients (94 percent) developed a postoperative wound complication; 10 of 18 (56 percent) required revision (2 Syme, 8 transtibial).
- Only 44 percent ever ambulated with a prosthesis; PROMIS physical-function scores did not improve and stayed well below the US average.
Limb salvage with Chopart's amputation and tendon balancing
- Describes the rationale for tendon balancing - anterior tibial tendon transfer plus tendo-Achilles lengthening - to counter the deforming equinoVARUS pull.
- The SHORTER the midfoot amputation, the greater the equinovarus tendency, exposing the cuboid and fifth metatarsal base to ulcerating pressure.
- By eliminating the cuboid, the Chopart level can paradoxically reduce varus and out-perform a short transmetatarsal or Lisfranc stump when balanced.
Outcomes of Chopart Amputation in a Tertiary Referral Diabetic Foot Clinic: 83 Hospitalized Patients
- Consecutive series of 83 diabetic patients (gangrene 46 percent, abscess 37 percent, osteomyelitis 17 percent); 77 percent required revascularisation, mean follow-up 2.8 years.
- Major (proximal) amputation was needed in 23 patients (27.7 percent; annual incidence 13 percent); ulcer recurrence in 31.9 percent of healed feet.
- 45.8 percent mortality over follow-up - age, prior stroke and urgent surgery were independent predictors of death.
Factors associated with successful Chopart amputation in patients with diabetes: a systematic review
- Systematic review of 4 studies, 74 ambulatory diabetic feet, weighted mean follow-up 21.1 months.
- A functional weight-bearing limb was maintained for at least 12 months when supported by a properly fitted high-profile prosthesis or AFO.
- Available data were too heterogeneous to prove the superiority of any single tendon-balancing or osseous (arthrodesis) technique.
Further reading: 1. Berger LE, Spoer DL, Huffman SS, et al. A comparative analysis of functional and patient-reported outcomes following Lisfranc and Chopart amputations in high-risk limb salvage patients. J Foot Ankle Surg. 2023;62(6):933-938. doi:10.1053/j.jfas.2023.04.014 (PMID 37160203) 2. Chiu YC, Chung TC, Wu CH, et al. Chopart amputation with tibiotalocalcaneal arthrodesis and free flap reconstruction for severe foot crush injury. Bone Joint J. 2018;100-B(10):1359-1363. doi:10.1302/0301-620X.100B10.BJJ-2018-0118.R1 (PMID 30295529) 3. DeGere MW, Grady JF. A modification of Chopart's amputation with ankle and subtalar arthrodesis by using an intramedullary nail. J Foot Ankle Surg. 2005;44(4):281-286. doi:10.1053/j.jfas.2005.04.014 (PMID 16012435) 4. Pinzur MS, Stuck RM, Sage R, Hunt N, Rabinovich Z. Syme ankle disarticulation in patients with diabetes. J Bone Joint Surg Am. 2003;85(9):1667-1672. doi:10.2106/00004623-200309000-00002 5. Sanders LJ, Dunlap G. Transmetatarsal amputation. A successful approach to limb salvage. J Am Podiatr Med Assoc. 1992;82(3):129-135. doi:10.7547/87507315-82-3-129 6. Dillon MP, Fatone S. Deliberations about the functional benefits and complications of partial foot amputation: do we know the full story? Med Hypotheses. 2013;81(4):754-761. doi:10.1016/j.mehy.2013.07.037 7. Early JS, Hansen ST. Surgical reconstruction of the diabetic foot: a salvage approach for midfoot collapse. Foot Ankle Int. 1996;17(6):325-330. doi:10.1177/107110079601700604 8. Harris WR. The classic: Syme's amputation: the technical details essential for success by Austen Harris. Clin Orthop Relat Res. 2012;470(4):947-950. doi:10.1007/s11999-011-2195-6