Serial casting and percutaneous tenotomy first-line; posteromedial release reserved for resistant, neglected, or syndromic feet
- The deformity components are corrected in the order CAVE: Cavus first (supinate the forefoot, dorsiflex the first ray), then Adductus and Varus together by abducting the foot around the talar head, and Equinus LAST.
- Correction occurs by ABDUCTING the foot around a fixed lateral talar head in supination — NEVER pronate the foot. Pronation worsens cavus and creates a bean-shaped midfoot break.
- Counter-pressure during manipulation is applied to the LATERAL HEAD OF THE TALUS (felt just anterior to the lateral malleolus), NOT the calcaneocuboid joint — the talar head is the fulcrum.
- Approximately 90% of feet require a percutaneous Achilles tenotomy to correct residual equinus after the forefoot and midfoot are corrected to 60-70 degrees of abduction.
- Foot abduction orthosis (boots-and-bar) worn 23 hours a day for 3 months then at night to age 4-5 years is essential — bracing non-compliance is the single leading cause of relapse (odds ratio about 27).
- Posteromedial release is now reserved for resistant, neglected, or syndromic feet — extensive soft-tissue release causes stiffness, overcorrection, and a higher long-term complication burden than Ponseti.
When & Why
First-line — the Ponseti method. Idiopathic congenital talipes equinovarus in the newborn, ideally started within the first 1-2 weeks of life when the connective tissues are most plastic. It applies to all idiopathic structural clubfeet regardless of severity, and is first-line (with modification and a lower success expectation) in syndromic and neuromuscular feet — arthrogryposis, myelomeningocele, diastrophic dysplasia. Late-presenting or neglected clubfoot can still be corrected by Ponseti in walking children up to several years of age, with longer casting and a greater likelihood of adjunctive surgery. When each step is added:
Residual equinus — less than 10-15 degrees of dorsiflexion — after the forefoot and midfoot are corrected to 60-70 degrees of abduction. Required in approximately 90% of idiopathic feet.
Dynamic supination relapse in a walking child, once the lateral cuneiform has ossified (about age 2.5-3 years and over) so the transfer has a bony anchor.
Resistant deformity failing serial Ponseti casting, neglected or late rigid feet, and severe syndromic or arthrogrypotic feet with recurrent rigid deformity. NOT routine first-line for idiopathic clubfoot.
Cautions. Do not force manual dorsiflexion to correct equinus before the midfoot is corrected — it breaks through the midtarsal joint producing a rocker-bottom deformity. Do not perform a tibialis anterior transfer before the lateral cuneiform is ossified (no bony anchor). Treat skin breakdown or active infection before casting. A fully passively correctable positional foot with a normal calf and no rigid equinus or cavus needs only reassurance and stretching — it is not a true structural clubfoot. Consent. Counsel families that the great majority of idiopathic feet are corrected without major surgery, that about 90% need a minor percutaneous tenotomy, and that the foot abduction orthosis is the most important part of treatment — worn 23 hours a day for three months then at night to age four to five years. Relapse is driven far more by brace non-compliance than by initial severity. Setup. The Ponseti method is a clinic technique needing only plaster materials and, for the tenotomy, a fine blade, with a cooperative infant on a parent's lap or a firm surface. Posteromedial release is performed in theatre, supine, with a tourniquet and loupe magnification for the medial neurovascular dissection.
The Operation
The goal: correct the deformity by gentle weekly manipulation and above-knee casting in the CAVE order, abducting the foot around the lateral talar head in supination, completing most feet with a percutaneous Achilles tenotomy, and reserving formal surgical release (tibialis anterior transfer, posteromedial release) for resistant, neglected, or syndromic feet. The medial exposure for posteromedial release is laid out as the final steps of the sequence below.


Operative sequence
- Position the infant comfortably; palpate the foot and confirm the rigid CAVE deformity before starting.
- Align the forefoot with the hindfoot by supinating the forefoot and dorsiflexing the first ray. This raises the medial arch out of cavus and creates a normal forefoot-hindfoot relationship before abduction begins.
- Cavus correction is usually achieved within the first 1-2 casts. The foot is held in supination throughout — never pronate, because pronation deepens the cavus and locks the hindfoot.
- Palpate the lateral head of the talus just anterior to the lateral malleolus; place the thumb on it as a fulcrum.
- Abduct the whole foot in supination around it with gentle sustained pressure, holding each correction for about 60 seconds before casting.
- The navicular, cuboid and calcaneus rotate laterally as a unit; the calcaneus everts and abducts beneath the talus, indirectly correcting the hindfoot varus.
- Progress to about 60-70 degrees of foot abduction relative to the thigh over typically 4-6 casts.
- Apply a well-moulded plaster from toes to upper thigh with the knee flexed 90 degrees.
- The above-knee component controls rotation and prevents the cast slipping; a below-knee cast loses the correction.
- Mould around the talar head and protect the lateral malleolus from pressure sores. Change weekly.
- Once abduction reaches 60-70 degrees and the heel varus has corrected, assess ankle dorsiflexion.
- If there is less than 10-15 degrees of dorsiflexion, residual equinus remains — proceed to percutaneous Achilles tenotomy (needed in about 90% of feet).
- Perform under local anaesthetic in clinic or light sedation, with the foot held in maximal dorsiflexion to put the tendon on stretch.
- Mark a point 1-1.5 cm proximal to the calcaneal insertion; introduce a fine blade (number 11 or 15, or a tenotomy beaver blade) flat against the medial border of the tendon.
- Turn the blade and divide the tendon transversely — a palpable give and a sudden increase in dorsiflexion (about 15-20 degrees) confirms a complete tenotomy.
- Apply a final above-knee cast in maximal abduction (60-70 degrees) and dorsiflexion for 3 weeks; the tendon regenerates at length.
- For dynamic supination during the swing phase of gait in a walking child whose static correction is maintained, once the lateral cuneiform has ossified (about age 2.5-3 years and over).
- Detach the tibialis anterior from the medial cuneiform or first metatarsal base through a dorsomedial incision.
- Pass the tendon subcutaneously and re-anchor it to the lateral (third) cuneiform through a dorsolateral incision, fixing with a bone tunnel and button or a suture anchor.
- This removes the dynamic supination force without weakening dorsiflexion. Often combined with a short repeat casting cycle and a repeat tenotomy if a fixed component remains.
- Reserved for resistant, neglected or syndromic feet that casting cannot correct; attempt casting first even in neglected feet, and release only the contracted structures (à-la-carte), not a routine complete release.
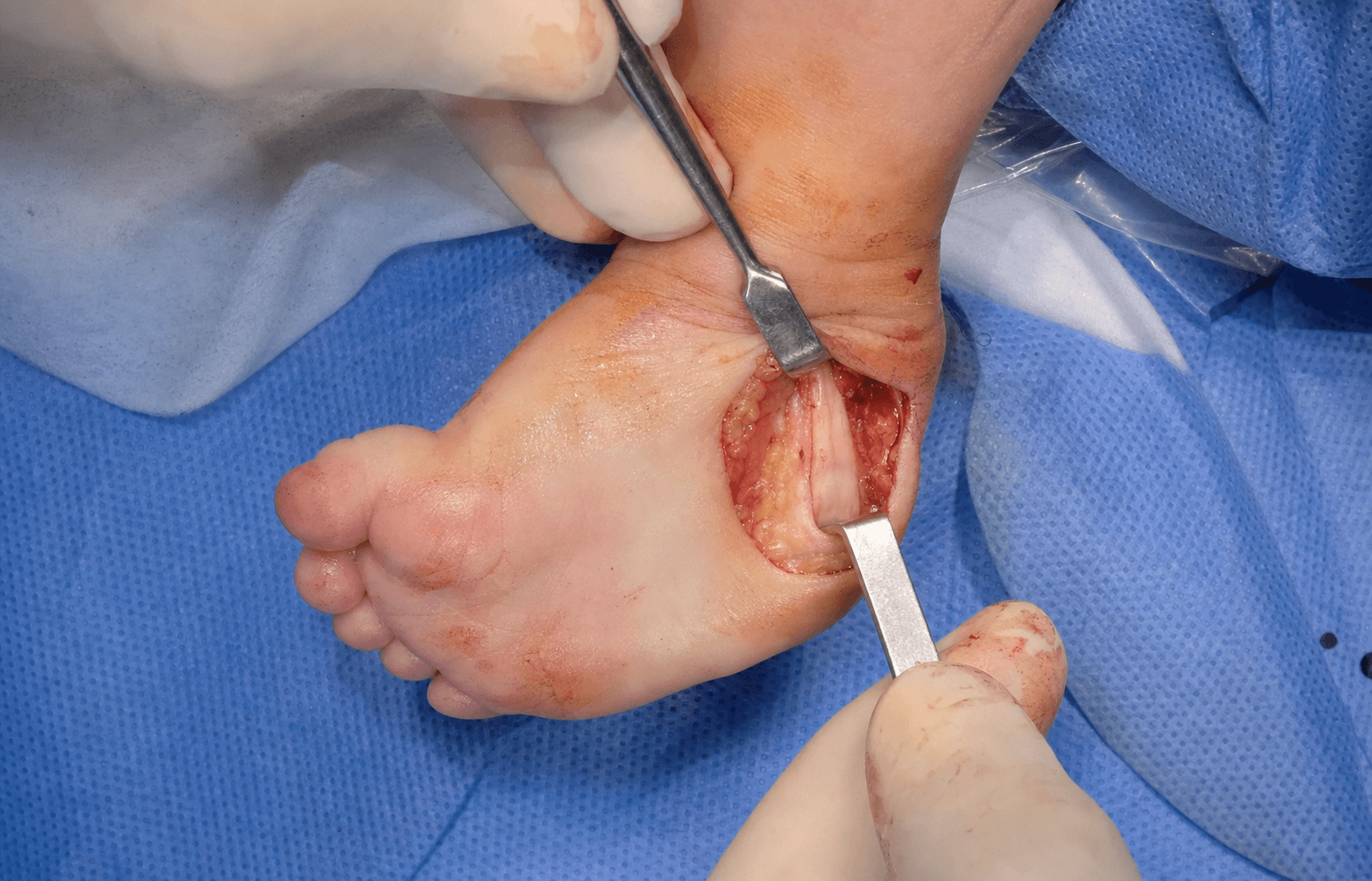
- Exposure: a medial incision (curvilinear, from the region of the medial malleolus and distal tibia along the medial border of the foot) opens the contracted posteromedial soft-tissue sleeve.
- Posterior release: a formal tendo-Achilles Z-lengthening (not just a tenotomy in the rigid older foot) and posterior ankle and subtalar capsulotomy to correct fixed equinus.
- Medial release: tibialis posterior lengthening, talonavicular joint reduction (the medially displaced navicular reduced onto the talar head), and release of the spring (calcaneonavicular) ligament, abductor hallucis, and the master knot of Henry where FHL and FDL cross.
- Plantar release: plantar fascia release for residual cavus.
- Reduce and stabilise the talonavicular (and sometimes subtalar) joint with K-wires; cast for 6-8 weeks.

Pronating the foot worsens the cavus and creates a stiff bean-shaped midfoot break. Applying counter-pressure on the calcaneocuboid joint instead of the talar head blocks subtalar derotation and prevents correction. Forcing dorsiflexion to correct equinus before the midfoot is corrected breaks through the midtarsal joint, producing a rocker-bottom (flatfoot) deformity. Correct strictly in CAVE order — equinus last.
The percutaneous tenotomy is performed 1-1.5 cm above the calcaneal insertion with the blade flat and shallow. The posterior tibial artery and tibial nerve lie anteromedial to the tendon and the sural nerve lateral — a blade plunged too deep or too medial risks neurovascular injury and posterior ankle capsule penetration. Confirm a complete cut by the palpable give and the gain in dorsiflexion; an incomplete tenotomy leaves persistent equinus.
In the medial release plane, meticulously protect the posterior tibial artery and tibial nerve — injury risks a dysvascular or insensate foot. Limit talar dissection to avoid avascular necrosis of the talus. Watch for overcorrection into planovalgus and long-term stiffness — the principal reason PMR is no longer first-line — and for wound problems closing skin over a newly corrected foot under tension.
Counter-pressure is on the lateral talar head, never the calcaneocuboid joint. The fulcrum is the talar head, palpable just anterior to the lateral malleolus. Abduct the foot in supination, holding each correction for 60 seconds before casting, and aim progressively for 60-70 degrees of foot abduction relative to the thigh.
Correction is by abduction of the whole foot in supination around the talar head; the calcaneus abducts and everts beneath the talus as a unit, indirectly correcting the hindfoot varus. Pronation deepens the cavus and locks the calcaneus under the talus — it is the classic error.
Aftercare & Complications
Foot abduction orthosis (boots-and-bar). A Denis Browne-type bar connects two open-toe boots set in external rotation — the affected foot in 60-70 degrees of external rotation (abduction), the normal foot in about 30-40 degrees, the bar shoulder-width. The brace does NOT correct deformity; it maintains the Ponseti correction and prevents relapse. Wear schedule. Full-time 23 hours a day for the first three months after the corrective cast comes off, then night-time and nap-time wear (12-14 hours a day) continued to age 4-5 years. Brace non-compliance is the single leading cause of relapse — Chen and Dobbs reported an odds ratio of about 27 for recurrence with non-compliance, making compliance the strongest modifiable predictor of success. Compliance counselling. Explain at every visit that non-compliance causes relapse far more than initial severity; address fit, skin irritation and socioeconomic barriers; document hours and check fit as the child grows. Recurrence — recognition and management
- Typical Age
- Infant or toddler
- First-Line Management
- Repeat Ponseti casting, with repeat tenotomy if equinus recurs
- Typical Age
- Walking child over 2.5-3 years
- First-Line Management
- Tibialis anterior transfer to the lateral cuneiform
- Typical Age
- Older child
- First-Line Management
- À-la-carte soft-tissue release
- Typical Age
- Adolescent or adult
- First-Line Management
- Calcaneal or midfoot osteotomy; triple arthrodesis as salvage
- Recognition
- Dorsal midfoot crease, convex sole, false correction of equinus
- Prevention and Management
- Prevention: correct CAVE in order; never dorsiflex before abduction is complete. Management: restart casting, correct cavus and abduction, then tenotomy for true equinus
- Recognition
- Skin breakdown over the lateral malleolus or heel; cast slipping distally
- Prevention and Management
- Prevention: above-knee cast, knee at 90 degrees, mould and pad the lateral malleolus. Management: change the cast; treat the skin; never over-tighten
- Recognition
- Less than 10-15 degrees of dorsiflexion persists; no give felt
- Prevention and Management
- Prevention: tendon on stretch, confirm the give and dorsiflexion gain. Management: repeat tenotomy; open lengthening if recurrent
- Recognition
- Bleeding, sensory loss, a dysvascular foot
- Prevention and Management
- Prevention: 1-1.5 cm above the insertion, blade flat and shallow, avoid a medial deep cut. Management: direct pressure; explore and repair if vascular injury
- Recognition
- Returning equinus or varus, dynamic supination at gait, lost abduction — up to 30-40% overall, far higher with brace non-compliance and in syndromic feet
- Prevention and Management
- Prevention: strict FAO compliance (23 hours then nights to age 4-5 years). Management: repeat casting with or without tenotomy; TA transfer for dynamic supination over age 2.5-3 years
- Recognition
- Flatfoot, heel valgus, weak push-off, painful midfoot — mainly after extensive PMR
- Prevention and Management
- Prevention: avoid routine full release; à-la-carte only. Management: orthoses; corrective osteotomy or arthrodesis if symptomatic and skeletally mature
- Recognition
- Reduced subtalar or ankle motion, pain, radiographic arthrosis — long-term after PMR
- Prevention and Management
- Prevention: minimise soft-tissue surgery (use Ponseti). Management: activity modification, orthoses; salvage fusion in adulthood
- Recognition
- Flattening or sclerosis of the talus on radiograph, stiffness, pain — rare, after extensive release
- Prevention and Management
- Prevention: limit talar dissection and stripping. Management: supportive; salvage procedures if collapse
Viva & Exam Focus
CAVECAVE — deformity components and order of correction
RELAPSERELAPSE — causes and management of recurrence
The trap: correcting all components at once, or correcting equinus first — forcing dorsiflexion before the midfoot is corrected breaks through the midtarsal joint, producing a rocker-bottom deformity. The fix: correct strictly in order — Cavus, Adductus, Varus, then Equinus last (often by tenotomy); cavus is corrected by supinating the forefoot, not pronating.
The trap: pronating the forefoot to correct the supination — this increases cavus, locks the calcaneus under the talus, and produces a stiff bean-shaped foot with a midfoot break. The fix: correction is by abduction of the whole foot in supination around the talar head; the calcaneus abducts and everts beneath the talus as a unit, indirectly correcting the hindfoot varus.
The fulcrum: the lateral head of the talus, palpable just anterior to the lateral malleolus as the navicular sits medially displaced against it. The risk: pressure on the calcaneocuboid joint instead blocks subtalar rotation and prevents correction; the thumb stabilises the talar head while the foot is abducted around it.
The location: the percutaneous Achilles tenotomy is performed 1-1.5 cm above the calcaneal insertion; the posterior tibial artery, tibial nerve and sural nerve lie anteromedial and lateral to the tendon. The risk: a blade plunged too deep or too medial risks neurovascular injury and posterior capsule penetration; a controlled entry with the blade flat against the tendon limits depth.
Positional: fully passively correctable, no true equinus or cavus, normal calf — reassurance or minimal stretching. Idiopathic structural: rigid CAVE, calf wasting — Ponseti. Syndromic or neuromuscular (arthrogryposis, myelomeningocele, diastrophic dysplasia): rigid, relapse-prone, higher release rate — Ponseti first but a lower threshold for surgery.
Why it matters: extensive posteromedial release historically produced overcorrected (planovalgus), weak, painful, stiff feet by adulthood — the reason Ponseti supplanted it as first-line. The implication: reserve formal release for feet that fail casting, neglected or late-presenting feet, and syndromic feet; a limited à-la-carte release is preferred over a routine complete PMR.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 2-week-old infant is referred with a bilateral rigid clubfoot. The parents ask how you will straighten the feet without an operation. Talk me through the Ponseti method and the order of correction.”
“A 3-year-old child successfully treated with Ponseti casting as an infant now walks with the foot turning inward during the swing phase of gait; the static position of the foot is well corrected. What is happening and how do you manage it?”
“You are asked to consider a posteromedial release for a neglected, rigid clubfoot in an older child. Which structures would you release, and what are the principal dangers and long-term concerns?”
Deformity and pathoanatomy
- Four components — CAVE: Cavus, Adductus, Varus, Equinus
- Talus in equinus with a medially and plantarly deviated neck; head uncovered laterally (the fulcrum)
- Navicular displaced medially and plantarward; calcaneus in varus and medially rotated under the talus
- Tight structures: Achilles, tibialis posterior, spring ligament, plantar fascia, posterior capsules
- Calf hypoplasia and a smaller foot are intrinsic and not correctable
Classification and scoring
- Pirani score 0-6: 3 hindfoot and 3 midfoot signs; a higher hindfoot score predicts tenotomy need
- Dimeglio score 0-20: four grades (I benign to IV very severe) by reducibility
- Higher initial severity means more casts, more likely tenotomy and relapse
- Differentials: positional, idiopathic structural, syndromic (arthrogryposis), neuromuscular, metatarsus adductus
Ponseti method
- Correct in CAVE order: Cavus first, then Adductus and Varus by abduction, Equinus LAST
- Abduct the foot in supination around the LATERAL TALAR HEAD — never pronate
- Counter-pressure on the talar head, NOT the calcaneocuboid joint
- Above-knee cast, knee at 90 degrees, changed weekly; usually 4-6 casts
- Target about 60-70 degrees of foot abduction with corrected heel varus
Percutaneous Achilles tenotomy
- Needed in about 90% of feet for residual equinus (less than 10-15 degrees dorsiflexion)
- Performed 1-1.5 cm proximal to the calcaneal insertion with the tendon on stretch
- Confirm a complete cut by a palpable give and a 15-20 degree gain in dorsiflexion
- Final cast in maximal dorsiflexion and abduction for 3 weeks
- Dangers: posterior tibial artery and tibial nerve (medial), sural nerve (lateral), posterior capsule
Foot abduction orthosis (bracing)
- Denis Browne boots-and-bar; affected foot in 60-70 degrees external rotation
- 23 hours a day for about 3 months, then nights and naps to age 4-5 years
- Maintains correction — does NOT actively correct
- Brace NON-COMPLIANCE is the leading cause of relapse (Dobbs)
- Reinforce compliance and check fit at every visit
Recurrence management
- Early supple relapse: repeat short Ponseti casting with or without repeat tenotomy
- Dynamic supination (walking child over 2.5-3 years): tibialis anterior transfer to the lateral cuneiform
- The transfer requires the lateral cuneiform to be ossified (bony anchor)
- Fixed or neglected rigid feet: à-la-carte soft-tissue release
- Syndromic feet relapse most — closer surveillance
Posteromedial release (reserved)
- Indications: resistant, neglected or syndromic feet failing casting
- Posterior: tendo-Achilles lengthening and posterior ankle or subtalar capsulotomy
- Medial: tibialis posterior lengthening, talonavicular reduction, spring ligament, abductor hallucis, knot of Henry
- Plantar: plantar fascia release; stabilise the talonavicular joint with K-wires
- Risks: tibial neurovascular injury, talar AVN, overcorrection, stiffness, arthritis, wound problems
Key exam traps
- Never pronate the foot — abduct in supination around the talar head
- Equinus is corrected LAST — never force early dorsiflexion (rocker-bottom)
- Counter-pressure on the talar head, not the calcaneocuboid joint
- Ponseti supplanted routine PMR because extensive release causes stiff, arthritic, overcorrected feet
- Compliance with bracing is the strongest modifiable predictor of success
Background & Evidence
Spectrum. Congenital talipes equinovarus is idiopathic in the great majority of cases; a smaller group are syndromic or neuromuscular (arthrogryposis, myelomeningocele, diastrophic dysplasia), which are rarer but more rigid and relapse-prone and often bilateral. Severity at presentation, captured by the Pirani and Dimeglio scores, predicts the treatment course. Deformity components (CAVE). Clubfoot is a three-dimensional deformity of the foot and ankle with four interrelated components.
- Description
- High medial arch, plantarflexed first ray
- Anatomical basis
- Forefoot pronated relative to the hindfoot (intrinsic tightness, tight plantar fascia)
- Description
- Forefoot adducted at the midtarsal joint
- Anatomical basis
- Medial displacement of the navicular on the talar head; tight medial structures
- Description
- Hindfoot inverted
- Anatomical basis
- Calcaneus inverted and medially rotated beneath the talus
- Description
- Hindfoot plantarflexed
- Anatomical basis
- Tight Achilles tendon, posterior ankle and subtalar capsules
Pathoanatomy. The talus is in fixed equinus with a medially and plantarly deviated neck; its head is uncovered laterally — the palpable fulcrum for correction. The navicular is displaced medially and plantarward, articulating against the medial malleolus rather than the centre of the talar head. The calcaneus is in varus, equinus and medially rotated beneath the talus (it does not simply invert — it rotates as a block with the navicular and cuboid). The cuboid is medially displaced on the calcaneus. Soft-tissue contractures involve the tibialis posterior, Achilles, FHL and FDL, the spring (calcaneonavicular) ligament, the deltoid, the plantar fascia, and the posterior ankle and subtalar capsules. Calf muscle hypoplasia and a smaller foot are intrinsic features that are not correctable. Severity scoring predicts the course. Both the Pirani and Dimeglio scores correlate with the number of casts required and the likelihood of needing a tenotomy or later surgery — a higher initial severity predicts a longer, more relapse-prone course. - Pirani score (0-6): six clinical signs each scored 0, 0.5 or 1 — hindfoot signs (posterior crease, empty heel, rigidity of equinus, 0-3) and midfoot signs (curvature of the lateral border, medial crease, position of the lateral talar head, 0-3). Tracked at each cast visit; a higher hindfoot score predicts the need for tenotomy.
- Dimeglio score (0-20): grades four reducibility parameters (equinus in the sagittal plane, varus in the frontal plane, derotation of the calcaneo-forefoot block around the talus, and forefoot adduction), each 0-4 by range of motion, plus one point each for medial crease, posterior crease, cavus and poor muscle condition. Four grades: I benign (soft-soft, 1-5), II moderate (soft greater than stiff, 5-10), III severe (stiff greater than soft, 10-15), IV very severe (stiff-stiff, 15-20).
- Key features
- Fully passively correctable, normal calf, no rigid equinus or cavus
- Implication
- Reassurance with or without stretching; excellent prognosis
- Key features
- Rigid CAVE, calf wasting, smaller foot
- Implication
- Ponseti first-line
- Key features
- Rigid, stiff, often bilateral, other joint contractures
- Implication
- Ponseti but relapse-prone; higher surgery rate
- Key features
- Insensate skin, weakness, rigid
- Implication
- Cast cautiously (skin risk); relapse common
- Key features
- Forefoot adduction only, no hindfoot equinus or varus
- Implication
- Distinct entity — not true clubfoot
Evidence base. The Ponseti method achieves initial correction in about 90-98% of idiopathic feet. The Iowa cohort (Laaveg and Ponseti, 70 patients and 104 feet at 10-27 years) showed durable, functional, supple, largely pain-free feet — the foundation of the method — and was the original basis for tibialis anterior transfer. By contrast, comprehensive posteromedial release produces stiffer, weaker, more painful feet over time with arthritic change: Dobbs et al. (45 patients, 73 feet at a mean 30 years) documented that functional impairment correlated with the extent of soft-tissue release. Non-compliance with the foot abduction orthosis is the dominant predictor of recurrence — Chen and Dobbs reported an odds ratio of about 27 for recurrence with non-compliance.
- Ponseti method
- About 90-98%
- Posteromedial release
- High, but at the cost of soft-tissue scarring
- Ponseti method
- Supple, mobile, functional
- Posteromedial release
- Stiff, prone to arthritis
- Ponseti method
- Pain-free, near-normal strength
- Posteromedial release
- More pain, calf and push-off weakness
- Ponseti method
- Brace non-compliance (modifiable)
- Posteromedial release
- Under or overcorrection, scarring
- Ponseti method
- Low (mostly repeat cast, tenotomy, TA transfer)
- Posteromedial release
- Higher — revision, salvage osteotomies
- Ponseti method
- First-line for nearly all feet
- Posteromedial release
- Resistant, neglected, syndromic only
References
Long-term results of treatment of congenital club foot (Iowa cohort)
70 patients (104 clubfeet) followed 10-27 years after manipulation-and-casting; a satisfactory functional result in 88.5% of feet and 90% of patients satisfied with appearance and function. Anterior tibial tendon transfer to the third (lateral) cuneiform appeared to prevent relapse, and most feet retained some loss of motion but remained functional and largely pain-free — the foundational evidence that the Ponseti method gives durable, supple feet and the original basis for tibialis anterior transfer.
Radical reduction in the rate of extensive corrective surgery for clubfoot using the Ponseti method
157 patients (256 idiopathic clubfeet); correction in 98% (all but 3 patients), with only 2.5% requiring extensive corrective surgery and 90% corrected with 5 or fewer casts. Relapse was 11% and related to foot-abduction brace non-compliance — not to age, prior treatment or initial severity; effective even in children up to 2 years after prior failed non-operative treatment. Confirms Ponseti as first-line with a radical reduction in extensive surgery, relapse driven by bracing non-compliance.
Long-term follow-up of patients with clubfeet treated with extensive soft-tissue release
45 patients (73 feet) treated by extensive posterior, medial and lateral release at a mean 30-year follow-up; the majority had significant limitation of foot function across three independent quality-of-life instruments. Functional impairment correlated with the extent of soft-tissue release — repeated releases gave stiffer, more arthritic, painful feet, while feet with a single, more limited procedure retained better ankle and subtalar motion. The pivotal evidence that comprehensive release produces stiff, arthritic, poorly functioning feet — the reason Ponseti supplanted routine PMR.
A new dynamic foot abduction orthosis for clubfoot treatment
Brace non-compliance was the strongest predictor of recurrence after Ponseti correction (odds ratio 27, 95% CI 2.2-326); both non-compliant patients developed recurrent deformity. An articulating dynamic foot abduction orthosis improved compliance (non-compliance 7% versus the authors' prior 41% with the standard brace) and halved skin-blistering (7% versus 23.5%). Quantifies bracing non-compliance as the dominant, modifiable driver of relapse — the basis for relentless compliance counselling.
Classification of clubfoot (Dimeglio severity score)
Defined a 0-20 scale from four reducibility parameters (sagittal equinus, frontal varus, derotation of the calcaneo-forefoot block, and forefoot adduction), adding points for medial crease, posterior crease, cavus and poor muscle condition, and stratifying feet into four grades (I benign to IV very severe or pseudo-arthrogrypotic). A validated severity score that, alongside the Pirani score, lets clinicians grade clubfoot at presentation, predict the course and objectively monitor correction across cast visits.