The common peroneal nerve at the fibular neck · intermediate
- The peroneus longus fascial edge (the fibrous arch where the nerve enters the muscle) is the MOST COMMON compression site - the common peroneal nerve equivalent of the arcade of Frohse for the posterior interosseous nerve, or Osborne's ligament for the ulnar nerve.
- The common peroneal nerve is most superficial and vulnerable where it wraps around the fibular neck 1-2 cm below the head, subcutaneous for about 4 cm - the site of external compression from casts, habitual leg crossing and operative positioning.
- Always find the nerve PROXIMAL first, in the interval between biceps femoris and the lateral head of gastrocnemius, then trace it distally around the fibular neck.
- Decompress BOTH terminal branches - the deep peroneal nerve (motor to dorsiflexion) and the superficial peroneal nerve (eversion and dorsum-of-foot sensation).
- Do NOT close the fascia tightly on closure - it recreates the compression you just released. Leave the fascia open or close it very loosely.
- Recovery is predicted by the duration of symptoms, the completeness of the lesion and the presence of a Tinel sign.
When & Why
Indication. Surgical decompression is offered for a common peroneal nerve palsy at the fibular neck that is compressive in origin, has failed an adequate trial of non-operative care, or is caused by a space-occupying lesion. The patient typically presents with a foot drop (weak or absent ankle dorsiflexion and eversion) with sensory loss over the lateral leg and dorsum of the foot, a positive Tinel sign at the fibular neck, and an intact ankle jerk and gastrocnemius-soleus function (which exclude a sciatic or tibial lesion). Absolute indications are progressive motor weakness (foot drop) with a compressive lesion, failure of conservative management after 3-6 months of observation, a space-occupying lesion (ganglion cyst, schwannoma), and an open injury with the nerve in continuity requiring exploration. Relative indications are persistent symptoms with documented compression on imaging, an iatrogenic injury after total knee arthroplasty or proximal tibial surgery, and a positive Tinel sign at the fibular neck with EMG confirming compression. Timing drives the decision to operate, and depends on the mechanism:
Observe for 3-4 months before exploring - most recover without surgery.
Operate earlier when symptoms are progressive, or when a space-occupying lesion such as a ganglion is present.
Explore early if there is no recovery by 6 weeks, particularly with a complete motor lesion.
Contraindications. Absolute: a complete nerve transection requiring grafting (a different procedure), active infection at the surgical site, and irreversible nerve damage with chronic denervation (greater than 18 months). Relative: a central cause of the foot drop (stroke, multiple sclerosis, spinal pathology), an L5 radiculopathy mimicking a CPN palsy, and an underlying polyneuropathy such as Charcot-Marie-Tooth disease, in which decompression is less effective. The differential of a foot drop must be excluded before operating - decompressing the peroneal nerve will not help an L5 radiculopathy:
- Differentiating features
- Weak hip abduction (gluteus medius), back pain, dermatomal sensory loss; ankle jerk usually preserved
- Differentiating features
- Hip abduction and hamstrings intact; sensory loss confined to the lateral leg and dorsum; positive Tinel at the fibular neck
- Differentiating features
- Weak hamstrings and an absent ankle jerk
- Differentiating features
- Upper motor neuron signs; no peripheral sensory pattern matching the CPN
- Differentiating features
- Upper and lower motor neuron signs together; no sensory loss
Pre-operative assessment. Document motor function (tibialis anterior power, resisted ankle dorsiflexion), a Tinel sign at the fibular neck (positive in a regenerating or compressed nerve), and the sensory examination over the lateral leg, dorsum of the foot and first web space. Palpate for a mass - a ganglion is palpable about 60 percent of the time - and confirm gastrocnemius-soleus function is intact (excludes a sciatic or tibial lesion). EMG and nerve conduction studies are essential: a conduction block at the fibular neck implies a good prognosis, while fibrillation potentials in tibialis anterior indicate denervation. MRI excludes a mass lesion and assesses nerve signal change; ultrasound allows dynamic assessment and identifies ganglion cysts and nerve calibre change. Consent. Counsel that 60-80 percent improve when the aetiology is compressive and preoperative function is good, that a complete foot drop present for greater than 12 months carries a poor prognosis, and that there is a 2-5 percent risk of worsening, plus incomplete recovery and residual numbness. Setup. Lateral decubitus (affected side up) is preferred, or supine with a bump under the ipsilateral hip, with the knee flexed 15-20 degrees to relax peroneus longus. A standard soft-tissue tray with bipolar cautery (essential for haemostasis near the nerve), loupe magnification (2.5-3.5x), a headlight, fine dissecting scissors (Metzenbaum, tenotomy), Penfield dissectors, vessel loops for nerve retraction and a self-retainer (Weitlaner or Gelpi). General or regional anaesthesia; full leg prep; a thigh tourniquet is optional and, if used, should be deflated before closure to check haemostasis.
The Operation
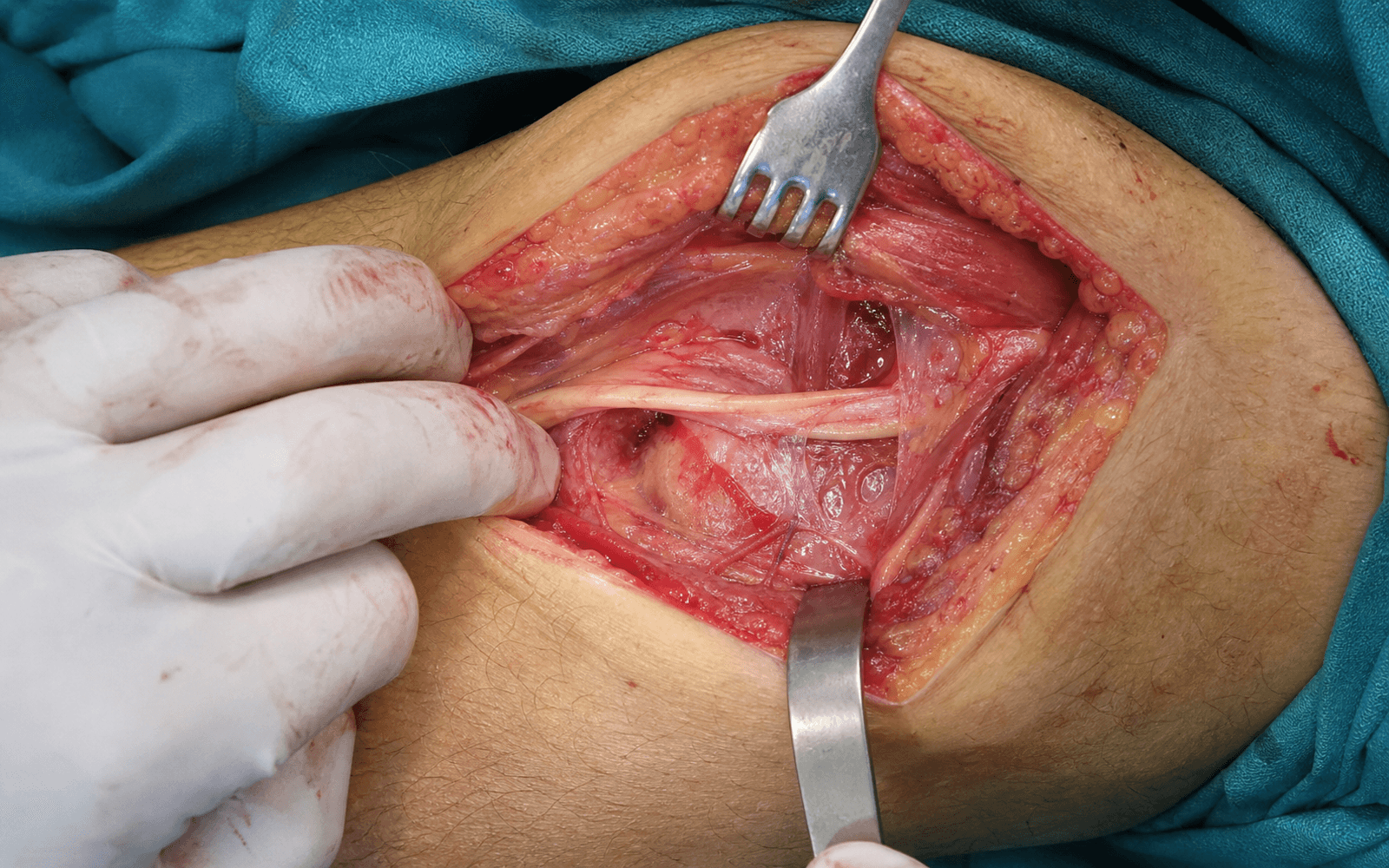
The goal is to expose the common peroneal nerve through a curvilinear incision centred on the fibular neck, find it safely in the proximal interval, trace it distally, and release every point of compression - above all the peroneus longus fascial arch - while protecting its branches and the lateral sural cutaneous nerve.
Operative sequence
- Lateral decubitus with the affected side up (preferred), or supine with a bump under the ipsilateral hip; flex the knee 15-20 degrees to relax peroneus longus.
- Mark the fibular head (the prominent landmark), the fibular neck, and the anticipated course of the CPN 1-2 cm below the head as it curves anteriorly.
- Palpate the fibular head - the nerve lies 1-2 cm distal and wraps the neck in the subcutaneous plane, where it can sometimes be felt as a cord.
- Make a 6-8 cm curvilinear incision centred on the fibular neck. Begin posteriorly (following the nerve's course from the popliteal fossa) and curve distally and anteriorly.
- The curve mirrors the nerve: the CPN comes from posteriorly, wraps around the neck, then dives anteriorly into peroneus longus. An incision too anterior misses the proximal compression sites; too posterior risks the sural nerve.
- Incise the subcutaneous tissue carefully. Identify and protect the lateral sural cutaneous nerve, which branches from the CPN proximal to the fibular head - injury causes numbness over the posterolateral calf.
- Loop it with a vessel loop for gentle retraction throughout the case.
- Incise the deep fascia longitudinally. Identify the CPN proximal to the fibular head, where it emerges in the interval between biceps femoris (anterior) and the lateral head of gastrocnemius (posterior).
- Always find the nerve proximally first, where it is easier and safer. Confirm identity with a nerve stimulator if uncertain.
- Pass a vessel loop around the nerve and trace it distally as it wraps around the fibular neck.
- This subcutaneous segment is the site of maximum vulnerability - the point where external compression (casts, positioning) acts - so handle it with atraumatic technique.
- Identify the fibrous arch at the entry to peroneus longus. Divide this fascial edge completely - this is the MOST COMMON compression site, the CPN equivalent of the arcade of Frohse.
- Visualise the nerve passing freely beneath the arch before moving on; an incomplete release is the commonest cause of persistent symptoms.
- Dissect the nerve free of all fibrous bands, scar and tight fascia around the fibular neck, including a tight intermuscular septum.
- Release constrictive tissue 360 degrees around the nerve so that it is freely mobile.
- Follow the nerve to its bifurcation into the deep and superficial peroneal nerves within peroneus longus, and decompress both at their respective compression points.
- Deep peroneal nerve: enters the anterior compartment through the anterior intermuscular septum - motor to dorsiflexion (tibialis anterior, EHL, EDL, EDB).
- Superficial peroneal nerve: continues in the lateral compartment - eversion (peroneus longus and brevis) and sensation over the dorsum of the foot.
- Examine the nerve for neuroma, hourglass constriction, intrinsic damage or a mass. If a ganglion is present (the most common mass lesion), excise it completely with its stalk, usually from the superior tibiofibular joint.
- Internal neurolysis (opening the epineurium) is controversial, with no proven benefit and a risk of worsening scarring - reserve it for obvious intraneural pathology.
- If the nerve is healthy externally but function is poor, external neurolysis is sufficient.
- If a complete transection is found, mark it for grafting (a separate procedure). A nerve in continuity that conducts an intraoperative nerve action potential should be left alone, not resected.
- Achieve meticulous haemostasis with bipolar cautery; deflate the tourniquet before closure to check.
- Do NOT close the fascia tightly - it recreates the compression. Leave the fascia open or close very loosely. Close the subcutaneous tissue and skin.
The fibrous arch where the nerve enters peroneus longus is the most common compression site and the key to the whole operation. Divide it completely and watch the nerve pass freely beneath it before you close. An incomplete release is the commonest cause of persistent symptoms after surgery.
Identify the common peroneal nerve proximal to the fibular head, in the clean interval between biceps femoris and the lateral head of gastrocnemius, before tracing it distally around the neck. A nerve stimulator confirms identity if you are unsure.
Tight fascial closure recreates the compression you just released. Leave the fascia open or close it very loosely - many surgeons do not close it at all.
Aftercare & Complications
Immediate post-operative care. No splinting is required unless a combined procedure has been performed. Elevate the leg for 24-48 hours to minimise swelling, allow weight-bearing as tolerated from the outset, and review the wound at 2 weeks. Ankle-foot orthosis. Continue an AFO for the foot drop until motor recovery is documented, using a custom-moulded AFO if prolonged use is anticipated. The priority is to prevent an equinus contracture while the nerve recovers. Rehabilitation and follow-up. Begin early ankle range-of-motion exercises, with physiotherapy strengthening as power returns and gait training with the AFO. Review clinically at 6 weeks, 3 months and 6 months, with a repeat EMG at 3-6 months to assess reinnervation. The first signs of recovery appear at 3-4 months and recovery may continue for 18-24 months. Expected recovery. Good-prognosis factors are a compressive aetiology, a short duration of symptoms, a partial lesion and a positive Tinel sign. Poor-prognosis factors are a traumatic transection, a duration greater than 12 months, an absent Tinel sign and no improvement on EMG. Overall, 60-80 percent of well-selected patients achieve meaningful improvement. Complications. Most are preventable with atraumatic handling, complete decompression of every site, and a loose closure.
- Recognition
- Increased weakness or numbness postoperatively
- Prevention
- Atraumatic handling; avoid excessive retraction
- Management
- EMG at 3 months; observe if the nerve is in continuity
- Recognition
- Persistent symptoms with no improvement at 6 weeks
- Prevention
- Decompress ALL sites including both branches
- Management
- Revision surgery if confirmed on EMG
- Recognition
- Numbness over the posterolateral calf
- Prevention
- Identify and protect it early with a vessel loop
- Management
- Usually permanent; no specific treatment
- Recognition
- Pain, swelling, an expanding mass
- Prevention
- Meticulous haemostasis; deflate the tourniquet before closure
- Management
- Evacuate if compressive; drain if required
- Recognition
- Erythema, drainage, fever
- Prevention
- Aseptic technique; prophylactic antibiotics
- Management
- Antibiotics; debridement if deep
- Recognition
- Wound separation over the fibular prominence
- Prevention
- Careful skin handling; avoid tension
- Management
- Secondary healing or revision closure
- Recognition
- Painful snapping of the nerve over the fibular head
- Prevention
- Avoid excessive proximal release
- Management
- Rarely symptomatic; fascial sling if problematic
- Recognition
- Burning pain, allodynia, colour and temperature change
- Prevention
- Atraumatic technique; early mobilisation
- Management
- Pain management, physiotherapy, specialist referral
Viva & Exam Focus
WRAPWRAP - causes of common peroneal nerve palsy
Hook:Weight-loss palsy is under-recognised - seen in ICU patients, after bariatric surgery and in anorexia.
FIBULARFIBULAR - compression sites, proximal to distal
Hook:The peroneus longus fascial edge is the fibular-tunnel equivalent - like the arcade of Frohse or Osborne's ligament.
- Course and function
- Wraps the fibular neck 1-2 cm below the head, subcutaneous for about 4 cm; the surgical target
- Where it is endangered
- Subcutaneous segment at the fibular neck - the site of external compression and direct injury
- Course and function
- Enters the anterior compartment; motor to tibialis anterior, EHL, EDL and EDB (dorsiflexion)
- Where it is endangered
- Anterior intermuscular septum and the peroneus longus fascia - must be decompressed
- Course and function
- Continues in the lateral compartment; motor to peroneus longus and brevis (eversion), sensory to the dorsum
- Where it is endangered
- Peroneus longus fascia and the lateral-compartment septa
- Course and function
- Branches from the CPN proximal to the fibular head; sensory to the posterolateral calf
- Where it is endangered
- Subcutaneous plane of the proximal incision - protect it with a vessel loop
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 45-year-old man presents with a right foot drop three weeks after a total knee arthroplasty. He cannot dorsiflex his ankle (MRC 0/5) and has numbness over the lateral leg and dorsum of the foot. The ankle jerk is intact. How would you investigate and manage this patient?”
“During a common peroneal nerve decompression you identify what appears to be a ganglion cyst arising from the superior tibiofibular joint. What is the significance of this finding and how would you manage it?”
“A thin 28-year-old woman presents with a gradual onset of bilateral foot drop over six months. She works as a seamstress and sits cross-legged while working. EMG shows a bilateral CPN palsy at the fibular neck. What is your management approach?”
Indications
- Compressive CPN palsy at the fibular neck with a foot drop
- Failed conservative management over 3 to 6 months
- A mass lesion (ganglion) requiring excision
- Progressive weakness, or a post-TKA palsy with no recovery
Critical anatomy
- The CPN wraps the fibular neck 1 to 2 cm below the head, subcutaneous for about 4 cm
- The peroneus longus fascial edge is the MOST COMMON compression site
- It divides into a deep branch (dorsiflexion) and a superficial branch (eversion, dorsum sensation)
- The lateral sural cutaneous nerve branches proximally - protect it to avoid calf numbness
Critical steps
- Find the nerve PROXIMAL first - in the biceps/gastrocnemius interval
- Release the peroneus longus fascia completely (the key decompression)
- Decompress BOTH the deep and superficial branches
- Do NOT close the fascia tightly - leave it open or loose
Danger zones
- The CPN itself - most superficial at the fibular neck
- Deep peroneal nerve - motor to dorsiflexion
- Superficial peroneal nerve - sensation to the dorsum
- Lateral sural cutaneous nerve - sensation to the posterolateral calf
Post-operative
- Weight-bear as tolerated; AFO until motor recovery is documented
- EMG at 3 to 6 months to assess reinnervation
- 60 to 80 percent achieve meaningful improvement with good selection
- Recovery may continue for 18 to 24 months
Exam tips
- The peroneus longus fascia is the arcade-of-Frohse equivalent for the CPN
- A ganglion is the most common mass lesion - excise the stalk
- Post-TKA palsy is usually neurapraxia - observe 3 to 4 months
- Internal neurolysis is not proven to help - avoid it unless there is intraneural pathology
Background & Evidence
Anatomical course - the basis of the operation. The common peroneal nerve arises from nerve roots L4-S2. It separates from the tibial nerve in the distal thigh at the sciatic bifurcation, runs along the medial border of biceps femoris, and emerges between biceps and the lateral head of gastrocnemius. At the fibular neck it wraps around 1-2 cm distal to the fibular head and is subcutaneous for about 4 cm - its most superficial and vulnerable point. It gives off the lateral sural cutaneous nerve proximally, then enters peroneus longus through a fibrous tunnel where it divides into the deep peroneal nerve (which enters the anterior compartment through the anterior intermuscular septum and supplies the dorsiflexors) and the superficial peroneal nerve (which continues in the lateral compartment to supply the evertors and the dorsum of the foot). Why the peroneus longus fascia matters. The fibrous arch at the entry to peroneus longus is the most common compression site - the common peroneal nerve equivalent of the arcade of Frohse for the posterior interosseous nerve or Osborne's ligament for the ulnar nerve. This single anatomical fact is the most commonly tested point on the operation. Epidemiology and aetiology. Causes include external compression (lateral decubitus positioning or a leg holder, plaster casts, habitual leg crossing), rapid weight loss (loss of the protective fat pad), a ganglion cyst arising from the superior tibiofibular joint, and a fibular neck fracture. Iatrogenic palsy complicates about 0.3 to 1.8 percent of total knee arthroplasties, and is more likely with a preoperative valgus deformity, prior lumbar laminectomy and epidural analgesia. Nerve-injury classification and surgical decision-making. Seddon's classification underpins the decision to observe, decompress or graft:
- Pathology
- Conduction block with an intact axon
- Prognosis and surgical relevance
- Full recovery; no surgery - the basis for observing a post-TKA or compressive palsy
- Pathology
- Axon disrupted, connective-tissue framework intact
- Prognosis and surgical relevance
- Wallerian degeneration then slow regeneration (about 1 mm per day); explore if there is no recovery
- Pathology
- Complete transection of the nerve
- Prognosis and surgical relevance
- No spontaneous recovery; needs repair or grafting - a different procedure
References
Management and outcomes in 318 operative common peroneal nerve lesions (LSU series)
- Largest single-centre operative series (318 knee-level CPN lesions, 1967-1999); stretch/contusion the commonest mechanism (44%)
- After external neurolysis, 107 of 121 lesions (88%) with a recordable intraoperative nerve action potential recovered useful function
- Graft length predicts outcome: 75% good function with grafts under 6 cm versus only 16% with grafts of 13-24 cm
The operative treatment of peroneal nerve palsy
- 31 patients decompressed after failed non-operative management; constricting fibrous bands consistently found at the fibular head AND at the proximal origin of peroneus longus
- 30 of 31 operated patients (97%) improved and discontinued their AFO, versus only 3 of 9 (33%) managed non-operatively (p less than 0.01)
- Authors recommend operative decompression if non-operative measures fail to improve symptoms
Peroneal nerve entrapment
- 60 patients (62 limbs) decompressed by dividing BOTH edges of the fibular fibrous arch; mean follow-up 42 months
- Good motor recovery (MRC grading) in 33 of 38 patients (87%) who had combined sensory and motor deficits
- Delay to surgery predicted failure: non-recovered patients had a mean 30-month delay versus 9 months in those who fully recovered
Patient outcome after common peroneal nerve decompression
- 51 decompressions reviewed for motor, sensory and pain outcomes
- Motor function improved in 40 of 48 (83%); pain improved in 26 of 31 (84%)
- Sensory recovery was less reliable - improvement in only 23 of 47 (49%)
Peroneal intraneural ganglia: the importance of the articular branch (unifying theory)
- Intraneural ganglia arise from the superior tibiofibular joint and track proximally along the articular branch within the epineurium of the deep peroneal nerve
- Explains the characteristic preferential deep peroneal (deep branch) deficit and the absence of pure superficial-only involvement
- Recurrence is 10-20% if the articular branch and joint connection are not addressed
Peroneal nerve palsy after total knee arthroplasty: predisposing and prognostic factors
- 32 palsies in 10,361 consecutive TKAs (about 0.3%); frequently delayed in presentation
- Significant risk factors: preoperative valgus deformity (p less than 0.0001), prior lumbar laminectomy (p less than 0.04) and epidural analgesia (p less than 0.03)
- Double-crush phenomenon proposed to explain palsy in patients with prior laminectomy or subclinical neuropathy
Complete reference list 1. Kim DH, Murovic JA, Tiel RL, Kline DG. Management and outcomes in 318 operative common peroneal nerve lesions at the Louisiana State University Health Sciences Center. Neurosurgery. 2004;54(6):1421-1428. 2. Mont MA, Dellon AL, Chen F, Hungerford MW, Krackow KA, Hungerford DS. The operative treatment of peroneal nerve palsy. J Bone Joint Surg Am. 1996;78(6):863-869. 3. Fabre T, Piton C, Andre D, Lasseur E, Durandeau A. Peroneal nerve entrapment. J Bone Joint Surg Am. 1998;80(1):47-53. 4. Maalla R, Youssef M, Ben Lassoued N, Sebai MA, Essadam H. Peroneal nerve entrapment at the fibular head: outcomes of neurolysis. Orthop Traumatol Surg Res. 2013;99(6):719-722. 5. Spinner RJ, Atkinson JL, Tiel RL. Peroneal intraneural ganglia: the importance of the articular branch. A unifying theory. J Neurosurg. 2003;99(2):330-343. 6. Schmalzried TP, Amstutz HC, Dorey FJ. Nerve palsy associated with total hip replacement. J Bone Joint Surg Am. 1991;73(7):1074-1080. 7. Idusuyi OB, Morrey BF. Peroneal nerve palsy after total knee arthroplasty: assessment of predisposing and prognostic factors. J Bone Joint Surg Am. 1996;78(2):177-184. 8. Kang HJ, Choi YR, Kang ES. Outcomes of arthroscopic excision of proximal tibiofibular joint ganglion cysts. J Bone Joint Surg Am. 2012;94(18):1678-1683. 9. Humphreys DB, Novak CB, Mackinnon SE. Patient outcome after common peroneal nerve decompression. J Neurosurg. 2007;107(2):314-318. 10. George SC, Boyce DE. An evidence-based structured review to assess the results of common peroneal nerve repair. Plast Reconstr Surg. 2014;134(2):302e-311e.