Varus-valgus constrained revision TKA for collateral ligament incompetence or an irreducible flexion-extension gap mismatch — the intermediate articulation between posterior-stabilised and a rotating hinge.
- CCK sits on the constraint ladder between posterior-stabilised (PS) and rotating-hinge designs — indicated when the collateral ligaments are incompetent or the flexion-extension gaps cannot be balanced with a PS implant, but a full hinge is not yet required.
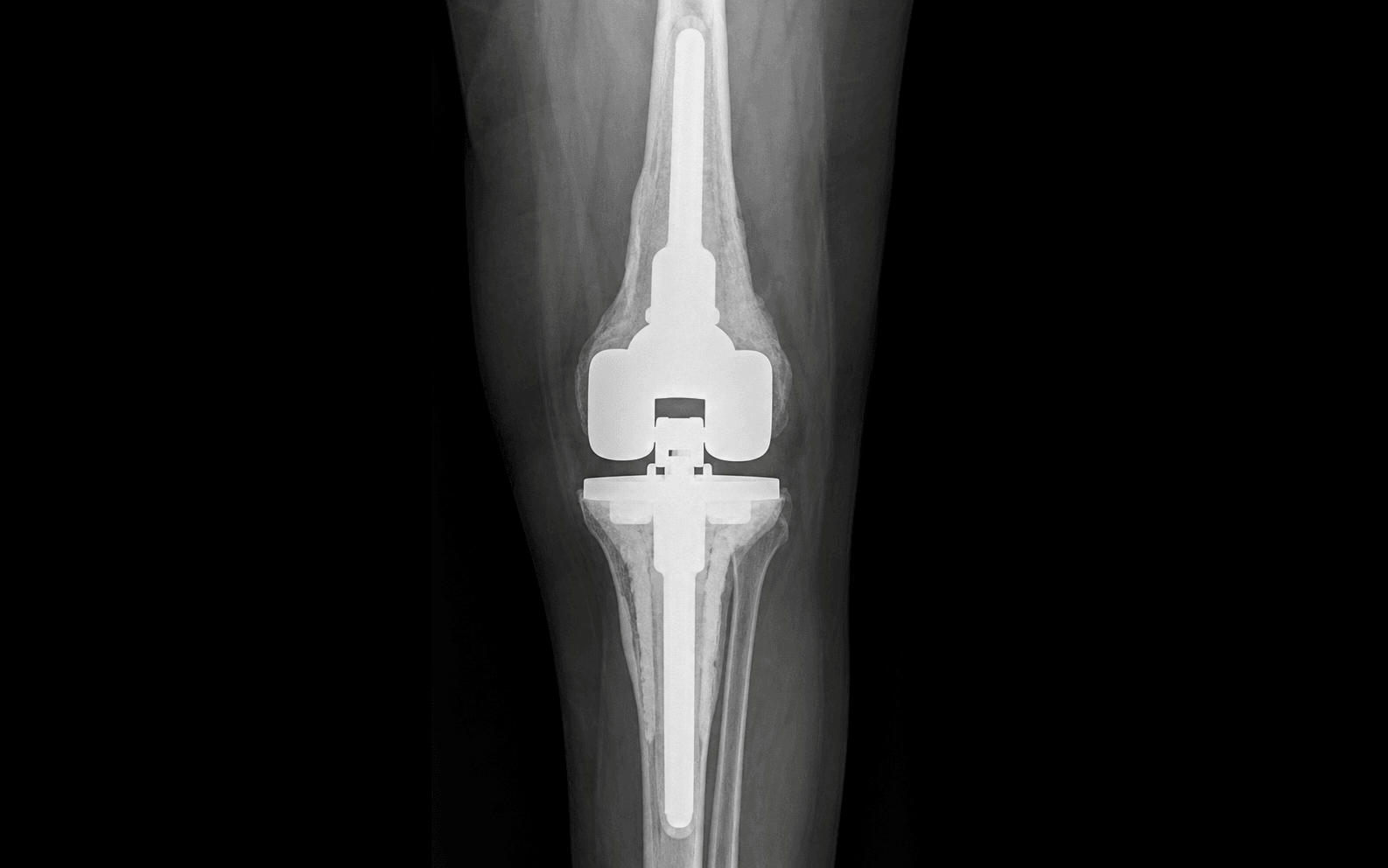
- The tall tibial post engages a deepened femoral box to resist varus-valgus angulation (approximately 2–4 degrees) and limit rotation (approximately 5–8 degrees) — constraint forces are transmitted directly to the implant-bone interface, so stems and metaphyseal cones or sleeves are mandatory.
- A deep medial parapatellar approach with an extensile option (quadriceps snip or tibial tubercle osteotomy) is required for safe component removal and gap assessment in the revision setting.
- Rehabilitation emphasises protected weight-bearing for 6 weeks when stems and cones are used, with gradual progression to full weight-bearing once metaphyseal integration is confirmed radiographically.
When & Why
A constrained condylar knee (CCK) — also called a varus-valgus constrained (VVC) implant — is the intermediate articulation on the revision constraint ladder. It is chosen when the collateral ligaments cannot provide coronal stability and a posterior-stabilised (PS) implant will not balance the gaps, but the deficiency is not severe enough to justify a rotating hinge. Move up the ladder one rung at a time — cruciate-retaining, then posterior-stabilised, then CCK, then rotating hinge, then fixed hinge — selecting the lowest constraint that solves the instability pattern.
Incompetent medial or lateral collateral ligament on stress testing (greater than 5–7 mm opening or asymmetric laxity); flexion-extension gap mismatch greater than 4 mm persisting after maximal soft-tissue release and component positioning; severe coronal deformity (greater than 15–20 degrees varus or valgus) not correctable with a PS implant; revision for instability with documented failure of a PS or cruciate-retaining design.
Complex primary TKA in inflammatory arthritis or neuromuscular disease where soft-tissue balancing is unreliable; conversion of a unicompartmental knee arthroplasty with collateral ligament damage; post-traumatic arthritis with collateral ligament disruption.
Absolute: active periprosthetic joint infection (eradicate first), extensor mechanism disruption (reconstruct staged or simultaneously), severe comorbidities precluding major revision. Relative: young high-demand patient (a rotating hinge may be more durable), massive bone loss needing a custom or megaprosthesis, likely non-compliance with protected weight-bearing.
- Indication
- Intact collaterals, balanced gaps
- Constraint mechanism
- Cam-post for AP stability only
- Fixation requirement
- Standard or short stems optional
- Durability concerns
- Instability if collaterals fail
- Indication
- Collateral incompetence or gap mismatch greater than 4 mm
- Constraint mechanism
- Tall post in deepened box limits VV and rotation
- Fixation requirement
- Mandatory stems plus cones or sleeves
- Durability concerns
- Post wear, post fracture, aseptic loosening
- Indication
- Complete collateral absence, massive bone loss
- Constraint mechanism
- Hinge gives VV stability, rotation unconstrained
- Fixation requirement
- Long stems and megaprosthesis options
- Durability concerns
- Bushing wear, aseptic loosening, infection
- Indication
- Neuromuscular disease, resection for tumour
- Constraint mechanism
- Rigid hinge, no rotation
- Fixation requirement
- Megaprosthesis with extracortical fixation
- Durability concerns
- High mechanical failure rate
A posterior-stabilised cam-post provides only anteroposterior stability — it cannot substitute for incompetent collaterals. Confirm the indication under anaesthesia with varus-valgus stress testing in full extension and at 30 degrees of flexion. Greater than 5 mm of asymmetric opening, or a flexion-extension gap mismatch greater than 4 mm that persists after soft-tissue release, mandates a constrained articulation. Never force further ligament division to make a PS implant fit — over-release creates iatrogenic instability you cannot salvage.
Setup. Supine on a radiolucent table with a bump under the ipsilateral hip, the leg draped free and a tourniquet high on the thigh. A sterile bump or triangle holds the knee at 90 degrees of flexion for most of the procedure, with the ability to extend for gap measurement. Plan the exposure and fixation beforehand on full-length standing radiographs and a CT for bone loss assessment.
The Operation
The goal is to remove the failed components without harming the extensor mechanism, reconstruct the metaphyseal bone loss, confirm that the instability or gap mismatch genuinely requires a constrained articulation, and implant a stemmed CCK with metaphyseal cones. The exposure — a deep medial parapatellar arthrotomy with an extensile option — is the foundation of a safe revision and is laid out as the first steps below.
Operative sequence
- Use the prior midline scar, extending proximally and distally as needed, and perform a medial parapatellar arthrotomy that preserves any remaining MCL fibres.
- Develop the plane along the medial side of the patella and quadriceps tendon, mobilising the patella without forcing eversion.
- If the patella will not evert safely or the components cannot be exposed, extend proximally and laterally through the quadriceps tendon at 45 degrees — a quadriceps snip — rather than struggling and avulsing the extensor mechanism.
- For more extensile access, perform a tibial tubercle osteotomy preserving a lateral soft-tissue hinge, fixed later with wires or screws.
- Remove all components with dedicated extraction devices, osteotomes and Gigli saws, preserving as much bone stock as possible.
- Pin the tibial tubercle with two 2.0 mm K-wires before tibial component extraction to prevent avulsion, and protect the patellar tendon insertion with a wire or pin.
- Use controlled osteotomes to avoid iatrogenic fracture of the femoral condyles or tibial plateau; excise scar tissue and irrigate thoroughly.
- Classify the metaphyseal bone loss with the AORI system (see Background & Evidence); CCK revisions almost always show AORI type 2 or 3 defects.
- Ream the tibial and femoral canals sequentially for stem trials so the stems engage the diaphysis for at least 100–150 mm.
- Trial metaphyseal cones or sleeves to achieve a circumferential press-fit in viable bone that gives rotational stability independent of the stem.
- Measure the extension and flexion gaps with spacer blocks or trial components (stems and cones in place) in full extension and at 90 degrees of flexion, releasing any residual soft-tissue contracture.
- Confirm the indication: if varus-valgus laxity exceeds 5 mm or the flexion-extension mismatch persists greater than 4 mm, select the CCK trial rather than over-releasing the posterior capsule or collaterals.
- Engage the tall tibial post in the femoral box and confirm stability with varus-valgus and anteroposterior stress testing.
- Impact the metaphyseal cones into the prepared bone, then mix cement and insert the stemmed definitive components, removing excess cement.
- Reference the tibial tubercle and the posterior tibial cortex to avoid tibial malrotation, and ensure at least 100–150 mm of diaphyseal stem engagement.
- Assess patellar tracking with the trial insert in place; correct component rotation or perform a lateral retinacular release if it maltracks before final cementation.
- Close the arthrotomy in layers over a drain, repair the quadriceps snip or tubercle osteotomy as appropriate, and place the knee in a hinged brace locked in extension.
- Obtain intra-operative radiographs to confirm component position, stem alignment and cone seating.
- Iatrogenic tibial tubercle avulsion — pin the tubercle before extraction.
- Patellar tendon rupture — protect the insertion with a wire or pin.
- Femoral condyle fracture during component removal — use controlled osteotomes and extraction devices; never leverage against the condyles.
- Tibial component malrotation — reference the tibial tubercle and the posterior tibial cortex.
- Patellar maltracking — assess tracking before final cementation and perform a lateral release if needed.
- Inadequate stem engagement — ensure at least 100–150 mm of diaphyseal fit.
Before any tibial component removal, pin the tibial tubercle with two 2.0 mm K-wires to prevent avulsion, and keep a low threshold for a quadriceps snip if the patella cannot be everted safely — extending the approach early is always better than struggling and damaging the extensor mechanism.
Measure the gaps in full extension and at 90 degrees flexion with the trial stems and cones in place. If the extension gap is tight and the flexion gap is loose by greater than 4 mm, accept the CCK construct rather than over-releasing the posterior capsule or collateral ligaments — the post-box will mechanically compensate for the mismatch.
Aftercare & Complications
Rehabilitation | Phase | Timing | Weight-bearing | Therapy goals | |-------|--------|----------------|---------------| | 1 | 0–6 weeks | Protected 20–50 percent with crutches or walker; hinged brace locked in extension for ambulation, unlocked for ROM | Passive and active-assisted ROM from day 1, aiming for 0–90 degrees by week 2; quadriceps sets and straight-leg raises | | 2 | 6–12 weeks | Progressive as tolerated once radiographic metaphyseal integration; brace weaning | Stationary cycling, pool therapy, progressive strengthening; independent ambulation by 12 weeks | | 3 | 3–6 months | Full weight-bearing | Advanced strengthening and proprioception; return to low-impact activities (walking, swimming, cycling); high-impact activities discouraged permanently | Radiographic surveillance at 6 weeks, 3 months, 1 year, 2 years, 5 years and 10 years monitors for component migration, osteolysis and post wear. Complications
- Rate and timing
- 2–5 percent; early (less than 90 days), higher with prolonged operative time
- Prevention
- Meticulous handling, prophylactic antibiotics
- Management
- Wound care; debridement and irrigation if deep
- Rate and timing
- Less than 2 percent; early
- Prevention
- Tubercle protection and extensile exposure planning
- Management
- Repair or reconstruction
- Rate and timing
- 1–3 percent; early
- Prevention
- Controlled osteotomes and extractors, careful stem insertion
- Management
- Fixation or revision as indicated
- Rate and timing
- 5–10 percent at 5 years; intermediate
- Prevention
- Mandatory stems plus cones or sleeves in every case
- Management
- Revision with adequate diaphyseal and metaphyseal fixation
- Rate and timing
- 3–8 percent at 5 years; intermediate
- Prevention
- Highly cross-linked polyethylene, radiographic surveillance
- Management
- Revise the articulation; reassess stems and cones
- Rate and timing
- Less than 5 percent; intermediate
- Prevention
- Correct component rotation, address progressive ligament attenuation
- Management
- Revision as indicated
- Rate and timing
- Cumulative 10–15 percent at 10 years; late
- Prevention
- Long-term radiographic surveillance
- Management
- Revision of the constrained articulation
- Rate and timing
- Late
- Prevention
- Surveillance radiographs
- Management
- Grafting and revision when symptomatic or progressive
Viva & Exam Focus
CCKCCK — constraint ladder and indications
GAPGAP — balancing before you commit to CCK
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 68-year-old woman presents with a painful, unstable total knee arthroplasty 7 years after primary surgery. She has 8 mm of medial laxity in extension and 12 mm in 30 degrees of flexion, and stress radiographs confirm collateral ligament incompetence. What implant do you select and why?”
“During a revision total knee arthroplasty you have removed the components and found a 6 mm flexion-extension gap mismatch that persists after posterior capsular release and collateral balancing, with moderate medial bone loss (AORI type 2). Which implant do you choose and what fixation strategy do you employ?”
“A 72-year-old man with a CCK revision performed 4 years ago presents with new-onset instability and a palpable clunk during flexion. Radiographs show no component migration but reveal asymmetric wear of the tibial post. What is the diagnosis and what are your management options?”
Indications
- Collateral incompetence: greater than 5 to 7 mm asymmetric varus-valgus laxity in extension or 30 degrees flexion
- Flexion-extension gap mismatch greater than 4 mm persisting after maximal soft-tissue release
- Severe coronal deformity (greater than 15 to 20 degrees) not correctable with a PS implant
- Documented failure of PS or CR design with instability; complex primary in inflammatory or neuromuscular disease
Constraint ladder
- CR less than PS less than CCK less than rotating hinge less than fixed hinge
- CCK gives 2 to 4 degrees varus-valgus constraint via a tall tibial post in a deepened femoral box
- CCK permits limited rotation (5 to 8 degrees) to reduce torsional transmission versus a fixed hinge
- Move up the ladder only when lower constraint fails the instability pattern
Mandatory fixation
- Every CCK requires diaphyseal stems (minimum 100 to 150 mm) in both tibia and femur
- Metaphyseal cones or sleeves are mandatory with AORI type 2 or 3 bone loss
- Constraint forces transmit to the implant-bone interface — without stems and cones, early loosening follows
- Cemented stems give immediate stability; cementless stems rely on diaphyseal fit and metaphyseal ingrowth
Surgical approach
- Deep medial parapatellar arthrotomy with quadriceps snip or tibial tubercle osteotomy for extensile exposure
- Pin the tibial tubercle before component removal to prevent avulsion
- AORI classification guides metaphyseal reconstruction (type 1 contained, type 2 moderate, type 3 severe)
- Gap assessment in extension and 90 degrees flexion after component removal
Complications
- Aseptic loosening (5 to 10 percent at 5 years) — almost always inadequate metaphyseal or diaphyseal fixation
- Polyethylene post wear or fracture (3 to 8 percent at 5 years) — presents with new instability or a clunk
- Wound infection or dehiscence (2 to 5 percent) — higher in revision with prolonged operative time
- Extensor mechanism disruption (less than 2 percent) — prevented by tubercle protection
- Recurrent instability (less than 5 percent) — usually component malrotation or progressive ligament attenuation
Post-operative protocol
- Protected weight-bearing 20 to 50 percent for 6 weeks with a hinged brace locked in extension
- Active and passive ROM from day 1, aiming for 0 to 90 degrees by week 2
- Advance to full weight-bearing once radiographic metaphyseal integration is confirmed
- Radiographic surveillance at 6 weeks, 3 months, 1, 2, 5 and 10 years for migration and post wear
Key evidence
- CCK survivorship free of revision for instability approximately 90 to 95 percent at 5 years when stems and cones are used
- Post wear remains the main mechanical concern at mid-term follow-up
- Rotating hinge reserved for more severe ligamentous deficiency or massive bone loss
- CCK is the appropriate intermediate constraint when PS balancing fails but a hinge is not required
Background & Evidence
The CCK articulation. The constrained condylar knee features a tall, rectangular tibial post that engages a deepened femoral box. Post height and box geometry limit varus-valgus angulation to approximately 2 to 4 degrees and restrict rotation to approximately 5 to 8 degrees. This provides coronal stability when the collaterals are incompetent while still allowing some rotation, which reduces torsional stress at the fixation interfaces compared with a fixed hinge. Why stems and metaphyseal fixation are mandatory. The constrained post-box articulation transmits coronal shear and torsional moments to the implant-bone interface. Without stems and metaphyseal cones or sleeves these forces cause early aseptic loosening. Every CCK revision therefore includes cemented or cementless diaphyseal stems (minimum 100 to 150 mm), porous metaphyseal cones or sleeves in both tibia and femur when AORI type 2 or 3 bone loss is present, and highly cross-linked polyethylene inserts when available to reduce post wear. Bone loss — the AORI classification. The Anderson Orthopaedic Research Institute (AORI) classification guides metaphyseal reconstruction, and CCK revisions almost always involve type 2 or 3 defects that necessitate cones or sleeves.
- Defect
- Minor contained defects
- Reconstruction
- Cement or particulate graft
- Defect
- Moderate metaphyseal bone loss
- Reconstruction
- Cones, sleeves or structural graft
- Defect
- Severe segmental or cavitary loss
- Reconstruction
- Megaprosthesis or custom components
Relevant anatomy in the revision setting. The MCL originates from the medial epicondyle and inserts on the proximal tibia approximately 5 to 7 cm distal to the joint line; in revision it is often attenuated, avulsed or scarred from prior surgery or instability. The LCL runs from the lateral epicondyle to the fibular head and is frequently incompetent in valgus deformity or after multiple revisions. The extensor mechanism — the patellar tendon insertion on the tibial tubercle — is the structure most at risk during tibial component extraction. Key evidence. Long-term single-centre series and registry data show solid survivorship for CCK revision TKA when stems and cones are used, with polyethylene post wear the dominant mid-term concern. Posterior-stabilised articulations show superior survivorship when the ligaments can be balanced, which reinforces reserving CCK for genuine collateral incompetence or irreducible gap mismatch. The full references are listed below.
References
Survivorship and complications in revision TKA with a constrained condylar knee implant: a minimum 10-year follow-up
- Minimum 10-year follow-up of CCK revision TKA demonstrated solid survivorship with stems and cones
Superior survivorship for posterior stabilised versus constrained condylar articulations after revision TKA: a retrospective comparative analysis at short-term follow-up
- CCK in revision showed acceptable short-term survivorship, though PS had superior rates when ligament balance was possible
Is hybrid fixation in revision TKA using LCCK prostheses reliable?
- Hybrid fixation with LCCK (Legacy Constrained Condylar Knee) in revision TKA is reliable with good outcomes
Incidence of constrained condylar and hinged knee implants and mid- to long-term survivorship: a register-based study from the Nordic Arthroplasty Register Association (NARA)
- Nordic registry data confirm mid- to long-term survivorship of constrained condylar implants in revision TKA