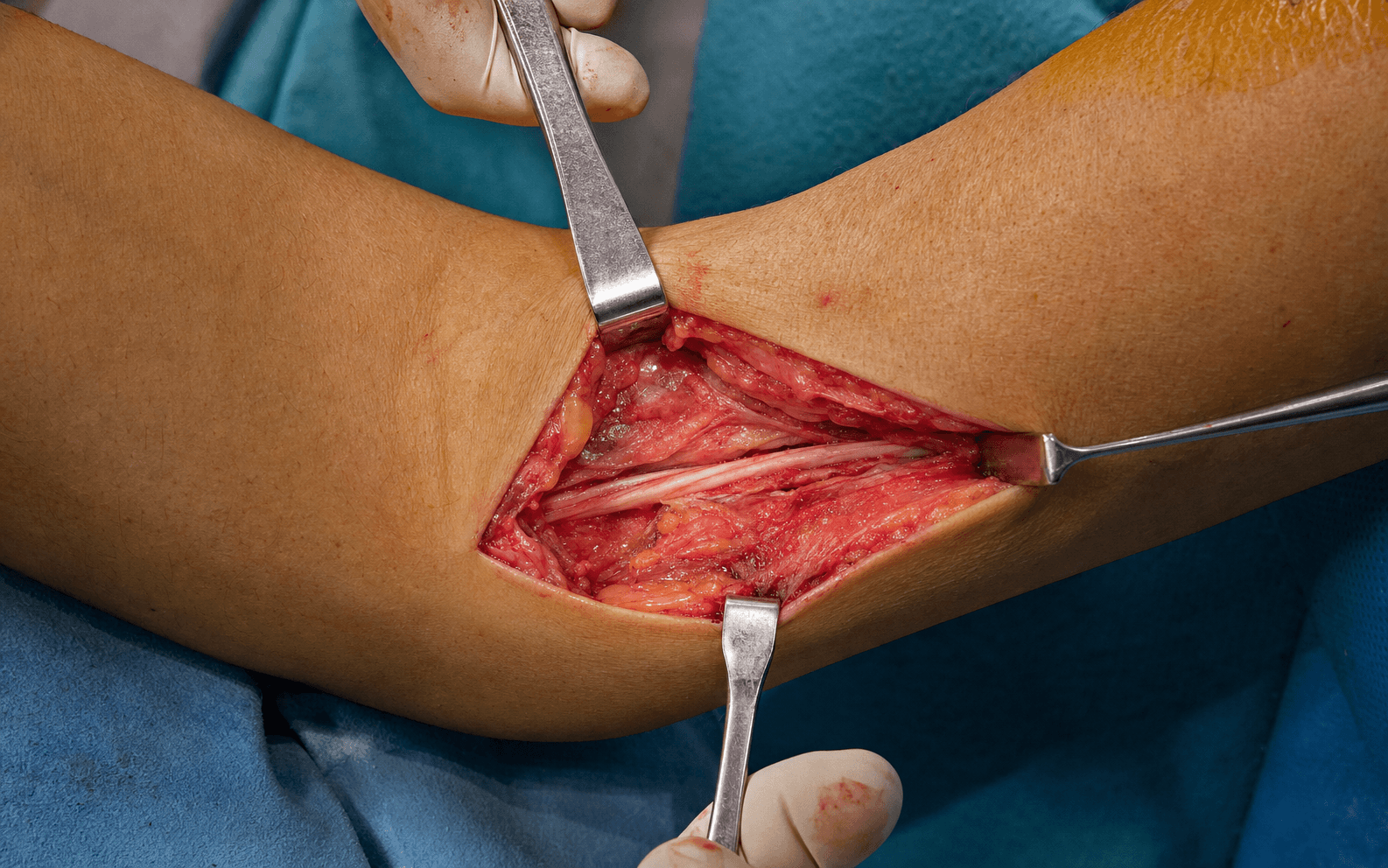
Medial elbow, lazy-S incision centred over the cubital tunnel · the second most common upper-limb compression neuropathy
- Cubital tunnel syndrome is the second most common upper-extremity compression neuropathy after carpal tunnel; failure of 3 or more months of conservative treatment is the primary surgical indication.
- Four critical compression sites must be released: the Arcade of Struthers (present in about 70 percent of patients), the medial intermuscular septum, Osborne's ligament (the primary site) and the FCU aponeurosis.
- The McGowan grade predicts outcome: Grade 1 (sensory only) 85–95 percent good results, Grade 2 (motor weakness) 70–80 percent, Grade 3 (severe atrophy) only 50–60 percent — counsel patients on this before operating.
- Simple decompression equals transposition for outcome but with less morbidity; reserve transposition for nerve subluxation, revision surgery, structural deformity or extensive scarring.
When & Why
Indication. Symptomatic ulnar neuropathy at the elbow — medial elbow pain radiating into the ring and small fingers, numbness in the ulnar distribution, a positive Tinel sign over the cubital tunnel and a positive elbow flexion test — with objective involvement on examination or nerve conduction studies, that has failed conservative management (activity and positioning advice, night extension splinting and NSAIDs) for at least 3–6 months. Absolute indications
- Progressive motor weakness (McGowan Grade 2–3) despite conservative treatment
- Severe symptoms affecting activities of daily living or occupation
- Documented ulnar nerve compression on electrodiagnostic studies (motor latency greater than 3.5 ms across the elbow, or conduction velocity less than 50 m/s across the elbow)
- Failed conservative management for 3–6 months Relative indications
- McGowan Grade 1 symptoms (sensory only) significantly interfering with work or function
- A subluxating ulnar nerve causing recurrent symptoms
- A space-occupying lesion compressing the nerve (ganglion, osteophyte)
- Post-traumatic cubital tunnel syndrome with structural deformity Contraindications
- Active infection overlying the surgical site
- Medical comorbidities precluding elective surgery
- An inadequate trial of conservative management (less than 3 months)
- Motor neuropathy from an alternative diagnosis (motor neuron disease, cervical radiculopathy) — exclude these before attributing symptoms to the elbow The one decision that matters. Whatever you add, every technique begins with the same step — complete release of every compression point along the ulnar nerve at the elbow. The only real choice is whether the nerve then stays in situ or is moved anteriorly:
The evidence-based default — equal efficacy to transposition with roughly one-third the complication rate. Release the four sites and leave the nerve on the floor of the tunnel.
Moves the nerve into subcutaneous fat anterior to the epicondyle, held by a fascial sling. Faster recovery, but the nerve is more vulnerable to direct trauma.
Passes the nerve beneath the elevated flexor-pronator origin — best protection and a vascularised bed, at the cost of temporary flexor-pronator weakness for 3–6 months.
Reserve transposition for documented nerve subluxation (pre-operative dynamic ultrasound or intra-operative flexion-extension testing), revision surgery, extensive perineural scarring preventing adequate in-situ release, post-traumatic or valgus structural deformity, or when medial epicondylectomy is performed. Consent specifically for medial antebrachial cutaneous nerve (MABCN) injury with a painful scar or neuroma (the most common complication, 15–30 percent), persistent or recurrent symptoms (10–25 percent, usually incomplete release), nerve subluxation after simple decompression (5–15 percent), elbow stiffness, haematoma and the small risk of nerve devascularisation. Setup. Supine with the arm on a hand table, shoulder abducted 90 degrees, elbow supported on a folded towel. Ensure the elbow can flex and extend freely through its full arc — you will test nerve excursion during the operation. Pad all bony prominences. Tourniquet is optional (a bloodless field, but it may worsen post-operative stiffness). Anaesthesia is general or regional (axillary/supraclavicular); avoid local infiltration around the nerve. Loupe magnification is mandatory — identifying the MABCN and the ulnar nerve is the whole game.
The Operation
The goal: expose the ulnar nerve through a medial lazy-S incision, protect the medial antebrachial cutaneous nerve throughout, identify the ulnar nerve in healthy tissue proximal to the compression zone, and systematically release all four compression sites — the Arcade of Struthers, the medial intermuscular septum, Osborne's ligament and the FCU aponeurosis — then decide, from a flexion-extension test, whether the nerve stays in situ or is transposed anteriorly. The exposure is laid out in full below (and in depth on the Hotchkiss medial approach to the elbow page).
Operative sequence
- Supine, hand table, shoulder abducted 90 degrees, elbow free to flex and extend, loupes on.
- Mark the landmarks: the medial epicondyle, the course of the ulnar nerve behind it, and the olecranon. Mark the planned lazy-S incision before tourniquet inflation if you use one.
- A curvilinear lazy-S incision centred over the cubital tunnel, from about 2 cm proximal to 6 cm distal to the medial epicondyle, crossing the epicondyle obliquely.
- It runs proximal-posterior to distal-anterior, avoiding direct pressure over the epicondyle and allowing extension either way if transposition is needed.
- A straight longitudinal incision 1–2 cm posterior to the epicondyle is simpler and adequate for a pure simple decompression, but limits extension.
- Use skin hooks, not forceps, for retraction — the MABCN is the structure most often injured.
- Identify the medial antebrachial cutaneous nerve early: it pierces the deep fascia about 10 cm proximal to the epicondyle and crosses the field about 10 mm anterior to it as a white, glistening structure.
- Trace it and protect it throughout — injury occurs in 15–30 percent of cases and causes a painful scar or neuroma. A posterior branch may cross more posteriorly and is at risk in deeper dissection.
- Palpate the nerve through the fascia 5–8 cm proximal to the epicondyle, where it is easily felt and lies in healthy tissue.
- Incise the deep fascia longitudinally directly over the nerve and elevate it gently with a nerve hook or vessel loop.
- Confirm the yellow-white colour, visible fascicles and longitudinal vessels. Always identify the nerve in normal tissue first — it is far safer and easier than starting in the scarred, compressed zone.
- Located 8–10 cm proximal to the medial epicondyle: a fibrous band passing from the medial intermuscular septum to the medial head of triceps.
- Present in about 70 percent of patients; if identified, pass a nerve hook beneath it and divide it under direct vision.
- Missing this proximal point is a classic cause of persistent symptoms after an otherwise "adequate" distal release.
- A thick fascial septum from the medial epicondyle separating the anterior (flexor) and posterior (extensor) compartments; it forms the posterior boundary of the nerve's course.
- For simple decompression, release it for 2–3 cm proximally if the nerve is stable.
- If you plan to transpose, you must excise a 5 cm segment completely — a retained septum creates a new anterior compression point and kinks the transposed nerve.
- The dense fibrous band forming the roof of the cubital tunnel, spanning from the medial epicondyle to the olecranon (the cubital tunnel retinaculum).
- Pass a nerve hook beneath it to define its extent, then divide it completely under direct vision — this is the tightest compression point in most patients.
- Confirm the release by feel: no remaining constricting bands. The nerve should expand visibly and any hourglass deformity should resolve.
- Located 3–4 cm distal to the joint line: the fascial band between the humeral head (medial epicondyle origin) and ulnar head of flexor carpi ulnaris.
- Split the aponeurosis longitudinally for 4–5 cm distal to the joint, staying midline.
- Protect the motor branches to FCU — they arise from the medial aspect of the nerve 20–40 mm distal to the epicondyle (1–3 branches). Follow the nerve distally into the forearm to ensure complete release.
- Inspect the decompressed segment for hourglass constriction, colour (pale suggests ischaemia), thickening or scarring, and any space-occupying lesion.
- Flex and extend the elbow while observing the nerve. Normal: the nerve glides smoothly with 4.7–8 mm of excursion and does not subluxate.
- If the nerve subluxates anteriorly over the medial epicondyle with flexion, anterior transposition is indicated to prevent recurrent compression.
- If the nerve is stable with smooth excursion and no subluxation, simple in-situ decompression is complete — proceed to closure.
- Mobilise the nerve with its vascular leash (surrounding fat and small vessels) for 6–8 cm proximal and distal to the epicondyle; avoid circumferential stripping to preserve the intrinsic blood supply.
- Completely excise the medial intermuscular septum for 5 cm proximally (prevents anterior kinking), and protect the FCU motor branches.
- Create the anterior bed — subcutaneous (lay the nerve in subcutaneous fat and fashion a fascial sling from flexor-pronator fascia to stop it falling back) or submuscular (elevate the flexor-pronator origin, create a muscular trough, pass the nerve beneath it and reattach the origin with non-absorbable sutures).
- Transpose the nerve in a smooth gentle anterior curve with no kinking at the proximal or distal transition; confirm it glides 5–10 mm through the full arc without tethering before securing it.
- Copious irrigation; bipolar cautery for bleeding points, kept away from the nerve.
- Achieve meticulous hemostasis — a haematoma compresses the nerve. Consider a small drain if dissection was extensive.
- Approximate the deep fascia loosely with absorbable suture; leave it open if closure would constrict the nerve.
- Close the subcutaneous layer (ensure the MABCN is not caught) and skin with monofilament or staples without tension.
- Apply soft padding and a posterior splint at 90 degrees of flexion for comfort only (longer, 2 weeks, after transposition).
The medial antebrachial cutaneous nerve is the most commonly injured structure in cubital tunnel surgery (15–30 percent of cases). It pierces the deep fascia about 10 cm proximal to the epicondyle and crosses the field around 10 mm anterior to it, only millimetres beneath the skin. Use skin hooks rather than forceps for retraction, identify the nerve early in the superficial dissection, trace and protect it throughout, and handle all tissues atraumatically. If it is transected, recognise it intra-operatively and repair it primarily with 8-0 nylon under loupe magnification.
After the four-site release, passively flex and extend the elbow while watching the nerve. A stable nerve gliding smoothly with 4.7–8 mm of excursion confirms an adequate simple decompression; an anterior subluxation over the medial epicondyle is your indication to transpose. This single dynamic test is the decision point examiners expect you to describe.
The Arcade of Struthers sits 8–10 cm proximal to the medial epicondyle and is present in about 70 percent of patients. A release that ends at Osborne's ligament leaves a proximal compression point behind — a classic cause of persistent symptoms after an apparently "adequate" distal release. Always carry the proximal dissection far enough to divide it when present.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 | 0–2 weeks | Posterior splint at 90 degrees for comfort only (2 weeks if transposed) | Gentle active elbow, wrist and finger range from day 1–2; remove splint for exercises | | 2 | 2–6 weeks | Discontinue splint at 2 weeks; avoid direct pressure on the elbow | Full active range of motion; light activities of daily living; begin strengthening at 4 weeks | | 3 | 6–12 weeks | Splint for heavy tasks only | Progressive strengthening (putty, therapy bands); avoid heavy lifting greater than 5 kg until 6 weeks | | 4 | 3–12 months | None | Graded return to full function; sensory and intrinsic motor recovery continue | Return to work is roughly 2–3 weeks for sedentary duties, 4–6 weeks for light duties and 8–12 weeks for heavy manual labour. Sensory symptoms (paraesthesiae) often improve within weeks; intrinsic motor strength recovers slowly over 6–12 months at the rate of axonal regeneration (about 1 mm per day). Outcome tracks the McGowan grade: Grade 1 reaches 85–95 percent good-to-excellent results, Grade 2 70–80 percent, and Grade 3 only 50–60 percent, rarely with full recovery. Complications
- Recognition
- Painful scar with a positive Tinel sign anterior to the incision; altered sensation over the medial forearm
- Prevention
- Skin hooks not forceps; identify the MABCN early ~10 mm anterior to the epicondyle; atraumatic handling
- Management
- Neuropraxia observes and recovers 6–12 weeks; neuroma — desensitisation, scar massage; persistent — excise and bury in muscle
- Recognition
- No improvement or early recurrence; paraesthesiae persist; repeat NCS shows persistent slowing at the elbow
- Prevention
- Complete release of ALL four sites (SAFE); adequate proximal (8 cm) and distal (6 cm) extent; confirm free gliding through full range
- Management
- Repeat EMG/NCS and MRI to localise; revision surgery if a specific compression point is found; consider transposition
- Recognition
- Recurrent symptoms with elbow flexion; palpable or visible snapping of the nerve over the epicondyle
- Prevention
- Intra-operative flexion-extension test before closure; low threshold to transpose if the nerve subluxates
- Management
- Asymptomatic — observe; symptomatic — revision with anterior transposition
- Recognition
- Reduced flexion and pronation strength immediately post-op; difficulty gripping
- Prevention
- Limit flexor-pronator elevation; anatomic reattachment with strong non-absorbable sutures; early mobilisation
- Management
- Usually resolves by 3–6 months with progressive strengthening; investigate detachment if persistent
- Recognition
- Worsening deficit immediately post-op; nerve pale intra-operatively; severe neuropathic pain
- Prevention
- Preserve the vascular leash during mobilisation; avoid circumferential stripping; minimise traction
- Management
- Supportive care, hand therapy, neuropathic pain agents; neurolysis if dense scar forms; prognosis guarded if severe
- Recognition
- Excessive swelling and pain early; tense wound, ecchymosis, worsening neurology
- Prevention
- Meticulous hemostasis with bipolar away from the nerve; consider a drain; soft dressing without excess compression
- Management
- Small — observe, elevate, ice; large or expanding — urgent evacuation in theatre
- Recognition
- Limited flexion-extension; pain at terminal motion
- Prevention
- Splint for comfort only 1–2 weeks; early range of motion from day 1–2
- Management
- Hand therapy and static progressive splinting; serial casting; rarely contracture release
Viva & Exam Focus
SAFESAFE Release — the four compression sites
Crosses the field about 10 mm anterior to the medial epicondyle. Use skin hooks not forceps, identify it early. Injury in 15–30 percent causes a painful neuroma.
Arise from the medial aspect of the ulnar nerve 20–40 mm distal to the epicondyle. Stay midline when splitting the FCU aponeurosis; division causes flexor carpi ulnaris weakness.
The anterior bundle lies deep to the nerve, from medial epicondyle to the sublime tubercle. Stay superficial during tunnel release; aggressive medial retraction causes valgus instability.
The posterior boundary of the medial compartment. Excise a 5 cm segment under direct vision if transposing; a retained septum kinks the transposed nerve anteriorly.
Segmental vessels enter the nerve throughout its course. Mobilise with the vascular leash (surrounding fat and vessels); avoid circumferential stripping, which devascularises the nerve.
Find the nerve in healthy tissue 5–8 cm proximal to the epicondyle before entering the compressed zone. Starting in scarred tissue risks iatrogenic injury.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 52-year-old carpenter presents with 8 months of medial elbow pain and numbness in the ring and small fingers. Examination reveals a positive Tinel sign at the cubital tunnel, a positive elbow flexion test, and weakness of the first dorsal interosseous but no visible atrophy. NCS shows an ulnar motor latency of 8.2 ms across the elbow (normal less than 3.5 ms) and a conduction velocity of 42 m/s. What is your management?”
“What are the main complications of cubital tunnel decompression and how do you prevent them? If a patient develops a painful scar anteriorly three months post-operatively with a positive Tinel sign, what has happened and how do you manage it?”
“Walk me through your technique for cubital tunnel decompression. After you release Osborne's ligament and inspect the nerve, how do you decide whether to perform simple decompression or anterior transposition?”
Indication
- Failed conservative care for 3–6 months with NSAIDs, activity modification and night extension splinting
- Progressive motor weakness (McGowan Grade 2–3)
- Electrodiagnostic confirmation: motor latency greater than 3.5 ms or conduction velocity less than 50 m/s across the elbow
The four compression sites (SAFE)
- Arcade of Struthers — 8–10 cm proximal, band from MIS to medial triceps head, present in ~70%
- Medial intermuscular septum — posterior boundary; excise 5 cm if transposing to prevent kinking
- Osborne's ligament — roof of the cubital tunnel, the PRIMARY compression site
- FCU aponeurosis — 3–4 cm distal, between the humeral and ulnar heads of FCU
Exposure & critical steps
- Lazy-S incision 2 cm proximal to 6 cm distal to the medial epicondyle
- Skin hooks (not forceps); identify and protect the MABCN ~10 mm anterior to the epicondyle
- Identify the ulnar nerve proximally in healthy tissue, not in the compressed zone
- Systematic four-site release, then the flexion-extension test before closure
Danger zones
- MABCN — injured in 15–30%, causes a painful neuroma
- FCU motor branches — medial aspect, 20–40 mm distal; division causes FCU weakness
- Ulnar collateral ligament — deep to the nerve; aggressive retraction causes valgus instability
- Intrinsic vascularity — preserve the vascular leash; circumferential stripping devascularises the nerve
Simple decompression vs transposition
- Cochrane: equivalent outcomes; transposition has a higher wound-infection rate
- Default is simple in-situ decompression — least morbidity
- Transpose for subluxation, revision, extensive scarring or structural/valgus deformity
- Submuscular gives best protection with temporary weakness; subcutaneous recovers faster
Complications
- MABCN injury 15–30% — skin hooks, early identification; neuroma → desensitisation then burial
- Persistent symptoms 10–25% — complete four-site release; revise if a compression point is found
- Subluxation 5–15% — flexion test; revise with transposition if symptomatic
- Elbow stiffness 5–10% — splint for comfort only 1–2 weeks, early motion
Post-op & prognosis
- Splint at 90 degrees for comfort only; active range from day 1–2
- Sensory recovery over weeks–months; motor recovery 6–12 months (~1 mm/day)
- Return to work: sedentary 2–3 weeks, light 4–6 weeks, heavy 8–12 weeks
- Outcome by McGowan grade: 1 → 85–95%, 2 → 70–80%, 3 → 50–60%
Background & Evidence
Epidemiology. Cubital tunnel syndrome is the second most common compression neuropathy of the upper extremity after carpal tunnel. It is slightly more common in men, peaks in the fifth and sixth decades, and is associated with repetitive or prolonged elbow flexion, pressure over the elbow, and conditions that alter nerve mobility or the local anatomy (prior elbow trauma, osteoarthritis, ulnar nerve subluxation). Pathoanatomy. The ulnar nerve lengthens by 4.7–8 mm and the tunnel pressure rises sharply with elbow flexion, so sustained flexion and nerve translation increase friction and compression. The nerve is segmentally supplied, with a zone of relative hypovascularity at the tunnel level, which is why mobilisation must preserve the surrounding vascular leash. Compression is rarely at a single point — it is the sum of four potential sites along the nerve's course at the elbow, which is why a complete release addresses all of them. McGowan classification (and its associated prognosis) is the standard pre-operative grading and the basis for counselling:
- Clinical features
- Subjective sensory symptoms only; no measurable motor weakness; no atrophy
- Prognosis (good to excellent)
- 85–95%
- Clinical features
- Sensory symptoms plus measurable weakness (first dorsal interosseous or pinch); no visible atrophy
- Prognosis (good to excellent)
- 70–80%
- Clinical features
- Profound intrinsic weakness with visible atrophy (first dorsal interosseous, hypothenar) and severe sensory deficit
- Prognosis (good to excellent)
- 50–60%, rarely full recovery
Key evidence — simple decompression versus transposition. The Cochrane review (Caliandro 2016) pooled 9 RCTs (587 participants); the comparison of simple decompression versus transposition across 3 clinical trials (261 participants) found no difference in clinical improvement (RR 0.93, 95 percent CI 0.80 to 1.08, moderate-certainty evidence), no difference in motor conduction velocity, and equivalence that held even when nerve impairment was severe. Transposition carried a higher wound-infection rate (RR 0.32, 95 percent CI 0.12 to 0.85). The 2025 Cochrane update (15 RCTs, 970 participants) reaffirmed little-to-no difference between simple decompression and either subcutaneous or submuscular transposition, and no difference between endoscopic and open decompression. The landmark RCTs agree. Bartels (2005) randomised 152 patients to simple decompression versus anterior subcutaneous transposition and found equivalent outcomes (good/excellent in 49 of 75 versus 54 of 77, not significant) with a far lower complication rate for decompression (9.6 percent versus 31.1 percent; RR 0.32, 95 percent CI 0.14 to 0.69) — the authors advised simple decompression even in the presence of nerve subluxation. Gervasio (2005) randomised 70 patients with severe (Dellon Grade 3) disease to decompression versus anterior submuscular transposition and again found equivalence (80 percent versus 82.9 percent good-to-excellent on the Bishop score, no recurrences in either group). Meta-analyses reach the same conclusion: Zlowodzki (2007) across 4 RCTs found no difference in nerve-conduction velocity or clinical scores, and Macadam (2008) across 10 studies (906 nerves) found no significant difference (odds ratio for improvement with decompression 0.75, 95 percent CI 0.54 to 1.04), with only a non-significant trend favouring transposition. Current recommendation. Simple in-situ decompression is first-line for idiopathic cubital tunnel syndrome — equal efficacy, lower morbidity. Transposition is reserved for documented subluxation, post-traumatic or valgus structural deformity, a space-occupying lesion, or revision after failed decompression. Where transposition is indicated, no high-quality evidence shows submuscular to be superior to subcutaneous; the choice turns on surgeon preference and patient factors (a slim or exposed elbow favours submuscular protection; the need for faster recovery favours subcutaneous).
References
Treatment for ulnar neuropathy at the elbow (Cochrane systematic review)
- 9 RCTs (587 participants); simple decompression versus transposition analysed in 3 clinical trials (261 participants)
- No difference in clinical improvement: RR 0.93 (95% CI 0.80 to 1.08), moderate-certainty evidence
- No difference in motor nerve-conduction velocity; equivalence held even when nerve impairment was severe
- Transposition carried a higher wound-infection rate (RR 0.32, 95% CI 0.12 to 0.85)
Treatment for ulnar neuropathy at the elbow (2025 Cochrane update)
- 15 RCTs (970 participants), 6 new trials added since the 2016 update
- Little to no difference in functional improvement for decompression versus subcutaneous (RR 0.92) or submuscular (RR 0.95) transposition
- No difference between endoscopic and open decompression on the Bishop score (RR 0.98, 2 trials, 99 participants)
- Insufficient evidence to define when to choose conservative versus surgical treatment, or to select a best technique by clinical, neurophysiological or imaging features
Simple decompression versus anterior subcutaneous transposition for idiopathic ulnar neuropathy at the elbow (RCT)
- 152 patients randomised: 75 simple decompression versus 77 anterior subcutaneous transposition, 1-year follow-up
- Good/excellent outcome 49 of 75 versus 54 of 77 — not statistically significant
- Complication rate significantly lower with decompression: 9.6% versus 31.1% (RR 0.32, 95% CI 0.14 to 0.69)
- Duration of symptoms, nerve (sub)luxation and severity did not influence outcome
Simple decompression versus anterior submuscular transposition in severe cubital tunnel syndrome (RCT)
- 70 patients with severe (Dellon Grade 3) disease randomised to decompression versus anterior submuscular transposition
- Good-to-excellent (Bishop score) in 80% (decompression) versus 82.9% (submuscular) — no significant difference
- No severe complications and no recurrences in either group at mean 47-month follow-up
- No difference in clinical or electrophysiological outcome
Simple decompression versus anterior subcutaneous and submuscular transposition of the ulnar nerve: a meta-analysis
- 10 comparative studies: 449 simple decompressions, 342 subcutaneous and 115 submuscular transpositions
- Odds of improvement with decompression versus transposition 0.75 (95% CI 0.54 to 1.04) — not significant
- Subgroup analyses by technique (subcutaneous versus submuscular) and by study quality were also non-significant
- A non-significant trend favouring transposition, with little publication bias or heterogeneity
Named-society practice — global synthesis (AAOS, BSSH/BOA, AANEM, EFSN)
- Diagnosis is clinical, supported by electrodiagnostics; motor conduction velocity across the elbow under 50 m/s and focal slowing or conduction block localise the lesion
- Trial conservative management (activity and positioning advice, night extension splinting, nerve gliding) for mild-to-moderate idiopathic disease before surgery
- In-situ decompression (open or endoscopic) is first-line surgery; outcomes equal transposition with lower wound morbidity
- Reserve transposition for documented subluxation, post-traumatic or valgus deformity, a space-occupying lesion, or revision after failed decompression
Further references 1. Zlowodzki M, Chan S, Bhandari M, Kalliainen L, Schubert W. Anterior transposition compared with simple decompression for treatment of cubital tunnel syndrome: a meta-analysis of randomized, controlled trials. J Bone Joint Surg Am. 2007;89(12):2591–2598. PMID 18056489. Level I meta-analysis (4 RCTs) showing equivalent clinical and electrophysiological outcomes. 2. Dellon AL. Review of treatment results for ulnar nerve entrapment at the elbow. J Hand Surg Am. 1989;14(4):688–700. PMID 2666496. Classic review establishing the sensory-plus-motor staging system and treatment algorithm by compression severity. 3. Assmus H, Antoniadis G, Bischoff C. Carpal and cubital tunnel and other, rarer nerve compression syndromes. Dtsch Arztebl Int. 2015;112(1–2):14–26. Comprehensive review of compression neuropathies including diagnostic and treatment algorithms.