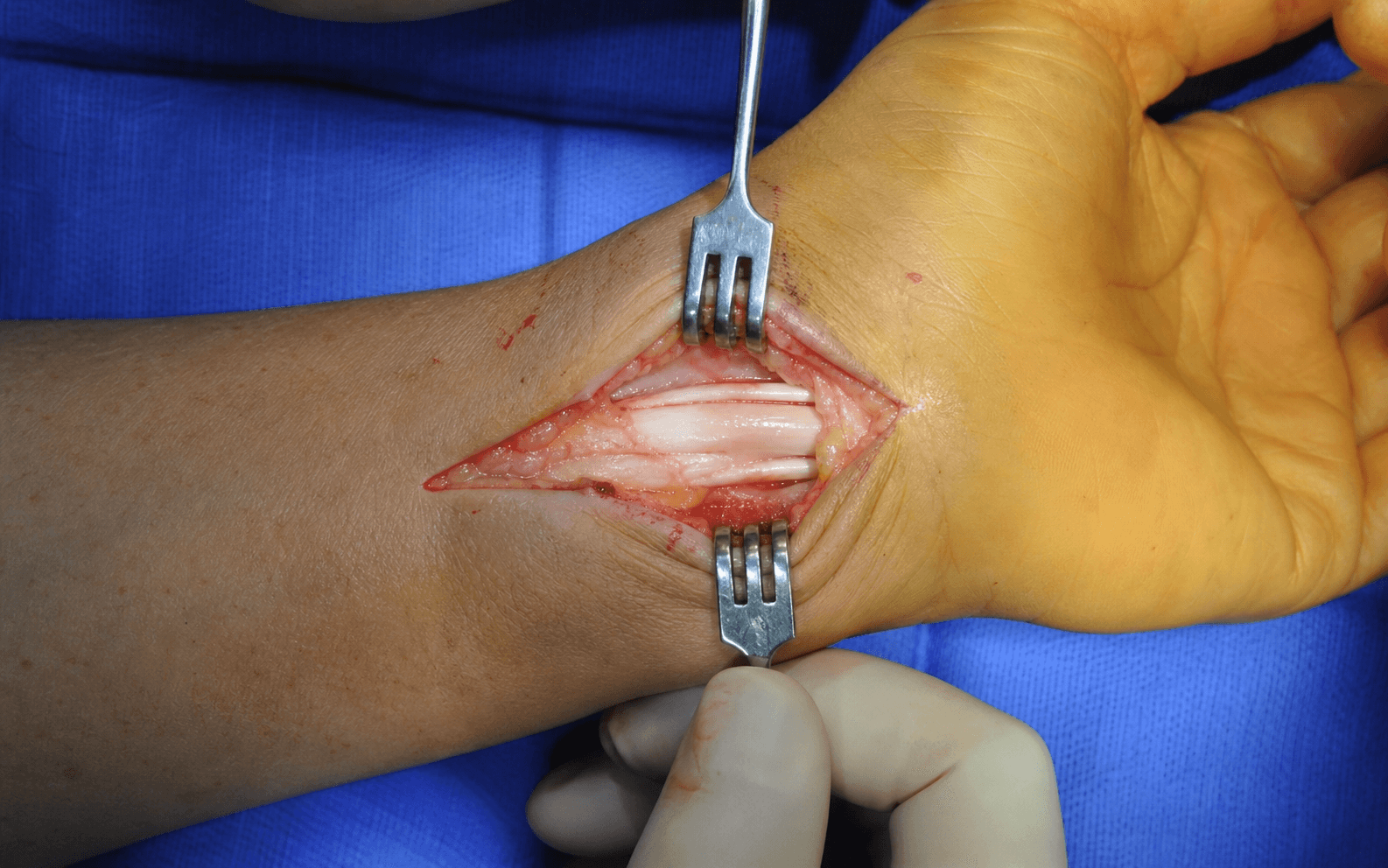
Open release of the stenosed first dorsal compartment (APL and EPB) at the radial styloid
- The first dorsal compartment contains APL (multiple slips in 50 to 80 percent, mean 2.2) and EPB; APL is the more volar/radial tendon and EPB the more dorsal/ulnar one.
- A septum is present in 20 to 30 percent and creates a SEPARATE EPB sub-compartment. A MISSED SEPTUM is the commonest cause of a failed release (60 to 80 percent of failures).
- The superficial radial nerve has 2 to 5 branches crossing the operative field; nerve injury is the commonest complication (5 to 10 percent).
- Release the radial/dorsal half (the roof) only and PRESERVE the volar floor to prevent volar tendon subluxation. Do NOT repair the retinaculum — dorsal tendon subluxation after release is normal and expected.
When & Why
Indication. Symptomatic De Quervain's stenosing tenosynovitis that has failed conservative management — pain over the radial styloid that is worse with thumb and wrist movement, a positive Finkelstein test, and significant functional impairment (gripping, lifting, ADLs) — typically after at least 3 to 6 months of symptoms. The Finkelstein test is the diagnostic hallmark (about 90 percent sensitive, 80 percent specific). The examiner passively flexes the patient's thumb fully into the palm (opposition), then ulnar-deviates the wrist while holding the thumb flexed; a positive test reproduces sharp pain over the radial styloid. The Eichoff modification has the patient make a fist over the tucked thumb and actively ulnar-deviate the wrist — the same principle. Always exclude the other causes of radial-sided wrist pain before operating:
- Where it hurts / what you find
- Pain at the thumb base, not the radial styloid
- How you tell it from De Quervain's
- Positive grind test; radiographs show trapeziometacarpal joint-space narrowing, osteophytes and sclerosis. Finkelstein usually negative
- Where it hurts / what you find
- Pain 4 to 6 cm PROXIMAL to the radial styloid, with prominent crepitus and swelling
- How you tell it from De Quervain's
- Where the second compartment (ECRL, ECRB) crosses the first (APL, EPB); Finkelstein may be weakly positive but the pain is proximal
- Where it hurts / what you find
- Point tenderness over the radial styloid bone, usually after trauma
- How you tell it from De Quervain's
- Radiographs show the fracture line; Finkelstein negative, or painful from the fracture rather than the tendons
- Where it hurts / what you find
- Burning, tingling and paraesthesiae rather than mechanical tendon pain
- How you tell it from De Quervain's
- Positive Tinel over the nerve course; sensory changes in the radial nerve distribution; Finkelstein negative
- Where it hurts / what you find
- Pain more volar, at the wrist crease
- How you tell it from De Quervain's
- Tenderness over FCR at the trapezium; pain on resisted wrist flexion and radial deviation; Finkelstein negative
Document failure of conservative care before offering surgery: - Thumb spica splint for 4 to 6 weeks (continuous, wrist neutral, thumb IP free), with NSAIDs and activity modification (avoid repetitive thumb and wrist motion).
- Corticosteroid injection (0.5 to 1 mL of steroid with local anaesthetic into the compartment — never intratendinous; stop if the tendon whitens). Initial success is 50 to 80 percent, but 30 to 50 percent recur within a year; usually 1 to 2 attempts are offered before surgery. Consent specifically for radial-sided numbness or a tender neuroma, scar tenderness, some temporary loss of pinch strength, a small risk of incomplete pain relief (and the possible need for revision), and — importantly — the expected dorsal prominence of the tendons afterwards. Setup. Supine, arm on a hand table, upper-arm tourniquet (250 mmHg), forearm supinated with the thumb in slight extension and abduction. Loupe magnification (2.5 to 3.5x) is mandatory — identifying the radial sensory nerve branches is the whole game. WALANT is an increasingly used alternative (see Background).
The Operation
The goal: open the stenosed first dorsal compartment, release every APL slip and the EPB sub-compartment (including the septum if present), while protecting the superficial radial nerve and the radial artery — then leave the retinaculum open. The exposure is laid out in full as the first steps below.
Operative sequence
- Supine, affected arm on a radial hand table, upper-arm tourniquet (250 mmHg). Exsanguinate (Esmarch or elevation) and inflate after prep and draping.
- Forearm SUPINATED, thumb in slight extension and abduction over a towel or hand block.
- Mark the first dorsal compartment over the radial styloid (passive thumb extension and abduction make the tendons prominent), the radial styloid tip, and the EPL tendon (third compartment) dorsally as a reference landmark.
- A TRANSVERSE incision (preferred), 1.5 to 2 cm, directly over the first compartment at radial styloid level, following the natural skin crease. It runs parallel to the superficial radial nerve branches (lower neuroma risk, better cosmesis), though it is less extensile.
- A LONGITUDINAL incision along the radial border (2 to 3 cm) is the alternative — more extensile, but perpendicular to the nerve branches and a worse scar.
- Incise skin and subcutaneous fat carefully; the nerve branches lie immediately deep.
- Loupes on (2.5 to 3.5x). Use fine tenotomy or Stevens scissors with a spreading technique parallel to the nerve course — never blind sharp dissection.
- Identify the 2 to 5 superficial radial nerve branches (mean 3) crossing the field; they appear as white cords with small accompanying vessels and follow no predictable pattern.
- Place a vessel loop around EACH branch and retract gently. Avoid cautery in the subcutaneous plane (bipolar only, and only after the nerves are protected).
- Retract the nerves and expose the thickened, white, glistening extensor retinaculum overlying the tendons (markedly thickened in chronic disease).
- Define the full extent — 2 to 3 cm proximal and about 1 cm distal to the styloid — and mark the release line along the RADIAL (dorsal) border, keeping the ulnar (volar) rim intact.
- With a 15 blade or tenotomy scissors, incise the retinaculum LONGITUDINALLY along the radial/dorsal border, from 2 cm proximal to 1 cm distal to the styloid.
- Incise the ROOF (dorsal half) only and PRESERVE the FLOOR (volar half) — the volar rim acts as a pulley and prevents volar tendon subluxation.
- Spread beneath the retinaculum to complete the release; the tendons should BULGE out dorsally, the sign of an adequate release.
- Inspect the compartment contents. The APL is the more VOLAR and RADIAL tendon; 50 to 80 percent of patients have MULTIPLE slips (mean 2.2, range 1 to 4). Use a probe to separate and count every slip and ensure each glides freely.
- If the tenosynovium is markedly thickened, perform a partial tenosynovectomy, but leave some paratenon — do not strip the tendons bare.
- Identify the EPB — more DORSAL and ULNAR, usually a single tendon inserting on the proximal phalanx base.
- ACTIVELY inspect for a SEPTUM: a white fibrous band between APL and EPB, present in 20 to 30 percent, that creates a SEPARATE dorsal/ulnar sub-compartment for EPB. Probe between the tendons; if EPB is tethered despite the main release, a septum is likely.
- If found, incise the septum COMPLETELY from proximal to distal and verify that EPB glides independently. A missed septum is the commonest cause of a failed release (60 to 80 percent of failures).
- Passively extend and abduct the thumb: the APL and EPB should glide smoothly and subluxate DORSALLY out of the compartment, each APL slip and the EPB moving independently.
- Passively flex and adduct the thumb: the tendons glide back easily.
- If they catch or stay in the tunnel, the release is INCOMPLETE — extend it further and re-check for a missed septum or APL slip.
- Release the tourniquet and achieve haemostasis with bipolar electrocautery (no monopolar near the nerves). Irrigate the wound.
- DO NOT REPAIR the retinaculum (it would recreate the stenosis); leave the tendons uncovered dorsally so they can subluxate — this is the intended result.
- Close the subcutaneous layer with 4-0 absorbable suture and the skin with 5-0 nylon or a subcuticular suture. Apply a sterile dressing and a short thumb spica splint (wrist neutral, thumb included, IP free) for comfort only.
The superficial radial nerve is injured in 5 to 10 percent of releases (the commonest complication). It lies immediately beneath the skin, with 2 to 5 branches crossing the field at unpredictable angles. Loupe magnification, a spreading technique, identification and vessel-loop retraction of every branch, a transverse incision, and avoidance of cautery in the subcutaneous plane are the preventive measures. Most injuries are neuropraxias that resolve over 6 to 12 weeks; a persistent painful neuroma (1 to 2 percent) may need excision and burial into pronator quadratus or bone.
The radial artery passes volar to the compartment, about 5 to 8 mm deep to its floor, beneath the APL tendons as it enters the anatomical snuffbox. Stay dorsal, preserve the volar floor, and avoid dissecting into the snuffbox. Injury is rare (less than 0.1 percent) but serious: direct pressure, identify the vessel, primary repair or controlled ligation (the ulnar artery usually suffices), and vascular help if needed.
A transverse incision runs parallel to the superficial radial nerve branches, lowering the neuroma risk and hiding the scar in a wrist crease. Reserve the longitudinal incision for when you genuinely need more extensile exposure.
After the main release, actively look for the septum — a pale fibrous band between APL and EPB, present in 20 to 30 percent. Probe between the tendons, divide it completely, and confirm EPB glides on its own. A missed septum is the commonest cause of a failed operation (60 to 80 percent of failures).
Leave the retinaculum open and the tendons uncovered dorsally. Dorsal prominence and subluxation of the tendons with thumb motion after release are NORMAL and expected — counsel the patient before the operation, not after.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Activity | |-------|--------|----------------|----------| | 1 | 0 to 2 weeks | Bulky dressing and short thumb spica splint (wrist neutral, thumb in, IP free) | Elevation, ice, finger ROM; splint for comfort only, removable | | 2 | 2 to 4 weeks | Splint off; sutures out at 10 to 14 days | Active thumb and wrist ROM; light ADLs; scar massage once healed | | 3 | 4 to 6 weeks | No splint | Progressive strengthening; return to sedentary work | | 4 | 6 to 8 weeks | None | Full activities, including heavy manual work and racquet or contact sports | Immediate pain relief occurs in about 95 percent of patients, with 85 to 95 percent excellent or good long-term results, recurrence in less than 5 percent, and satisfaction of 90 to 95 percent. Full ROM is typically achieved by 2 to 4 weeks and full strength by 6 to 8 weeks. Most patients do NOT need formal hand therapy — self-directed ROM is enough; refer only for persistent stiffness, weak grip, scar adhesions or CRPS concerns. Counsel patients that dorsal tendon prominence and a palpable 'popping' with thumb motion are normal post-operative findings, not complications. Complications
- Recognition
- Numbness over the dorsoradial hand; a tender Tinel at the scar, burning and hypersensitivity
- Prevention
- Loupes, spreading dissection, identify every branch, vessel loops, transverse incision, no cautery near nerves
- Management
- Neuropraxia: observe and desensitise, resolves 6 to 12 weeks. Persistent neuroma: excision and burial, or repair or graft if transected
- Recognition
- Pain and a positive Finkelstein that never settled, identical to pre-op
- Prevention
- Inspect for and divide the septum; release every APL slip; extend the release adequately; run the excursion test
- Management
- Confirm diagnosis, exclude CMC arthritis, intersection syndrome and neuroma; ultrasound or MRI for a septum; revision release with septum division (70 to 85 percent success)
- Recognition
- The tendons subluxate VOLARLY with thumb motion — a clunk, pain, functional limitation
- Prevention
- Preserve the volar floor; release the roof only; no circumferential release
- Management
- If symptomatic, reconstruct a volar pulley (retinacular graft); if asymptomatic, observe
- Recognition
- Tendons bulge dorsally and 'pop' with thumb motion, usually painless
- Prevention
- Expected after an adequate release; counsel the patient pre-operatively
- Management
- Reassurance; no treatment needed
- Recognition
- Increasing pain, redness, warmth, purulent drainage, fever
- Prevention
- Sterile technique, haemostasis, careful wound care
- Management
- Oral antibiotics and local wound care; deep infection needs debridement, IV antibiotics and cultures
- Recognition
- A sensitive, raised scar; pain with wrist and thumb motion
- Prevention
- Gentle skin handling, meticulous haemostasis, transverse incision, tension-free closure
- Management
- Massage, silicone, desensitisation; steroid injection or rare revision
- Recognition
- Pulsatile bleeding from the wound floor; expanding haematoma
- Prevention
- Stay dorsal, preserve the floor, avoid the snuffbox
- Management
- Direct pressure, primary repair or ligation, vascular help; confirm ulnar inflow first
Viva & Exam Focus
SEPTUMSEPTUM — inspect after the main release
RADIALRADIAL — protect the superficial radial nerve
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“Describe the anatomy of the first dorsal compartment. What is the significance of a septum?”
“Explain the Finkelstein test and the differential diagnosis for radial-sided wrist pain. How do you distinguish these conditions clinically?”
“A patient returns 3 months after first dorsal compartment release with persistent pain and a positive Finkelstein test. What is your differential diagnosis and management?”
Indications
- Symptomatic De Quervain's failing conservative care (splint 4 to 6 weeks plus NSAIDs plus 1 to 2 steroid injections)
- Positive Finkelstein test (about 90 percent sensitive, 80 percent specific)
- Exclude CMC arthritis (grind test), intersection syndrome (4 to 6 cm proximal), radial styloid fracture and Wartenberg syndrome
Key anatomy
- First dorsal compartment: roof = retinaculum, floor = periosteum; ulnar border = second compartment (ECRL, ECRB)
- APL volar/radial, multiple slips in 50 to 80 percent, to metacarpal base; EPB dorsal/ulnar, usually single, to proximal phalanx
- Septum in 20 to 30 percent creates a separate EPB sub-compartment — a missed septum is the commonest cause of failure (60 to 80 percent)
- Superficial radial nerve 2 to 5 branches cross the field — the commonest complication (5 to 10 percent)
Critical steps
- Transverse incision; loupes; identify and loop every nerve branch
- Release the roof (radial/dorsal) only, preserve the volar floor
- Release every APL slip; actively find and divide the septum; verify EPB glides
- Excursion test: tendons subluxate dorsally with thumb extension
- Do NOT repair the retinaculum
Complications
- Radial sensory nerve injury or neuroma 5 to 10 percent (commonest)
- Persistent pain from incomplete release 2 to 5 percent (missed septum in 60 to 80 percent)
- Volar subluxation less than 1 percent; radial artery injury less than 0.1 percent
- Dorsal tendon prominence is NORMAL, not a complication
Post-op
- Thumb spica for comfort 1 to 2 weeks, then active ROM
- Immediate pain relief in about 95 percent; 85 to 95 percent excellent results
- Sedentary work 2 to 3 weeks; heavy work 6 to 8 weeks; recurrence less than 5 percent
Background & Evidence
First dorsal compartment anatomy. A fibro-osseous tunnel at the radial styloid level: the roof is the extensor retinaculum (thickened in De Quervain's), the floor is the periosteum over the radial styloid and radius, the radial border is subcutaneous tissue and the ulnar border is the second dorsal compartment (ECRL, ECRB). It contains two tendons:
- APL
- Volar and radial within the compartment
- EPB
- Dorsal and ulnar within the compartment
- APL
- 1 to 4 slips (multiple in 50 to 80 percent, mean 2.2)
- EPB
- Usually a single tendon
- APL
- Posterior radius, ulna and interosseous membrane (mid-forearm)
- EPB
- Posterior radius and interosseous membrane (distal to APL)
- APL
- Base of the first metacarpal (radial side)
- EPB
- Base of the proximal phalanx (dorsal)
- APL
- Thumb abduction (radial plane), CMC extension, radial deviation
- EPB
- Thumb MCP and IP extension
Through a transverse incision; allows full inspection for the septum and every APL slip. The evidence-based default.
Smaller portals and potentially lower nerve risk, but you cannot assess the septum adequately and the failure rate is higher. Not recommended when a septum is suspected.
1 percent lidocaine with epinephrine 1:100,000, no tourniquet; the awake patient can move the thumb for a dynamic check of the release. Increasingly used in the procedure room.
For a failed primary release the commonest finding at revision is a missed septum (60 to 80 percent); re-explore, divide the septum, extend any inadequate release and free missed APL slips. Revision succeeds in 70 to 85 percent when a cause is found and corrected. If both De Quervain's and CMC arthritis are present they can be addressed at one sitting (release the first compartment first, then the CMC arthroplasty). Guidelines, registries & global practice. | Domain | Global consensus (AAOS, BSSH/BOA, ASSH, FESSH) | |--------|------------------------------------------------| | First-line | Corticosteroid injection into the compartment plus a thumb spica; injection has the strongest evidence base | | Surgery threshold | Failure of conservative care, typically after 1 to 2 injections; no registry tracks tendon-sheath releases | | Operative principle | Release both APL and EPB sub-compartments, protect the radial sensory nerve, do NOT routinely repair the retinaculum | | Practice variation | WALANT and procedure-room release increasingly favoured worldwide for cost and dynamic intra-operative assessment; endoscopic release used selectively but risks a missed septum | There is no implant or arthroplasty registry relevant to this soft-tissue procedure; regional differences relate mainly to setting (theatre versus procedure room) and anaesthetic technique (tourniquet or regional versus WALANT) rather than the operative steps, which are globally consistent.
References
Incidence of a septum within the first dorsal compartment of the wrist
Dissection of 100 cadaver wrists found a septum in 34 percent, consistently separating APL from EPB to create a discrete EPB sub-compartment; when present on one side it was usually bilateral. This is the anatomical basis for the single most important intra-operative step: after the main release the surgeon must actively inspect for a septum and release the separate EPB sub-compartment, otherwise EPB remains stenosed.
De Quervain tenosynovitis of the wrist
An authoritative review confirming stenosing tenosynovitis of APL and EPB in the first dorsal compartment, more common in women, with corticosteroid injection plus a thumb spica splint usually successful as first-line treatment. At surgery, protect the radial sensory nerve and identify every accessory compartment; retinacular repair is rarely needed.
Patient satisfaction and outcomes of surgery for de Quervain's tenosynovitis
In 43 consecutive wrists at a mean 3-year follow-up the cure rate was 91 percent with 88 percent fully satisfied; recurrence occurred in 2 (5 percent), radial sensory nerve injury in 1 (2 percent) and severe scar tenderness in 1 (2 percent). Open release is reliable definitive treatment, and avoiding complications — especially radial sensory nerve injury — is the dominant determinant of satisfaction.
Long-term results of surgical release of de Quervain's stenosing tenosynovitis
In 94 consecutive patients under a single surgeon a successful outcome (negative Finkelstein) was achieved in all cases, with six peri-operative complications: four transient radial nerve lesions, one superficial infection and one delayed healing. Decompression of both tendons with limited retinacular resection (a maximum of 3 mm) gives excellent long-term cure; transient radial nerve dysfunction is the commonest morbidity and usually resolves.
Effectiveness of corticosteroid injection and splint in diabetic de Quervain's tenosynovitis patients
A randomised trial of 168 patients (84 diabetic, 84 non-diabetic) comparing injection alone with injection plus splint found QuickDASH and VAS improved in all groups at 12 months, but outcomes were worse in diabetics; adding a forearm-based thumb splint helped non-diabetics but not diabetics. Corticosteroid injection is effective first-line, but diabetic patients respond less well and should be counselled about a higher likelihood of needing surgery.