Spontaneous EPL rupture after distal radius fracture — the EIP transfer, step by step
- EPL rupture typically occurs 6–8 weeks after a non- or minimally displaced distal radius fracture — the timing is the classic advanced orthopaedic practice question.
- Mechanism: ischaemia at Lister's tubercle from haematoma compression in the tight 3rd extensor compartment, combined with abrasion on the irregular fracture surface.
- Direct repair FAILS — attritional rupture creates a 2–4 cm gap defect with poor tissue quality; EIP-to-EPL transfer is the gold standard.
- EIP lies ULNAR to EDC to index on the dorsum of the hand — confirmed by extending the index finger alone while the other fingers are held in a fist.
- EPL test: with the hand flat on a table the patient cannot lift the thumb off the surface (loss of retropulsion) — pathognomonic for EPL rupture.
- Tension: with the wrist at neutral the thumb must achieve full IP extension — too loose gives no extension; too tight holds the IP fixed in flexion.
When & Why
Primary indication. EPL rupture with inability to actively extend the thumb interphalangeal (IP) joint. The transfer is performed for: - Spontaneous EPL rupture after a distal radius fracture (most common — whether managed conservatively or operatively)
- EPL rupture in rheumatoid arthritis, after failed synovectomy or presenting with rupture
- Iatrogenic EPL rupture after ORIF of the distal radius (plate prominence, retractor injury, dorsal screw tip penetrating the 3rd compartment floor)
- Delayed presentation (greater than 3 weeks from rupture), where direct repair is no longer feasible
- Any EPL rupture with a gap defect or poor tendon-end quality Why EIP transfer, not a free graft. The EIP is a functioning, independently innervated motor that can be harvested in the same field and woven directly into the EPL stump in a single stage. A free tendon graft is a passive conduit that relies on the proximal EPL muscle belly and needs a junction at each end. EIP is the standard first-line choice; a graft (palmaris longus or plantaris) is reserved for when EIP is unavailable.
- EIP Transfer
- Active motor transfer — EIP is an independent extensor
- Free Tendon Graft (PL/Plantaris)
- Passive conduit — relies on the EPL proximal motor stump
- EIP Transfer
- Always available (EIP present in about 99.5%)
- Free Tendon Graft (PL/Plantaris)
- Palmaris longus absent in 10–15% bilaterally; plantaris in about 8%
- EIP Transfer
- Single-stage, same field
- Free Tendon Graft (PL/Plantaris)
- Two-incision harvest; junctions at both ends are vulnerable
- EIP Transfer
- Reliable — useful functional extension in the large majority
- Free Tendon Graft (PL/Plantaris)
- Good results in skilled hands; gap junctions can fail
- EIP Transfer
- Minimal deficit — EDC maintains index MCP extension
- Free Tendon Graft (PL/Plantaris)
- No donor deficit
- EIP Transfer
- Standard first-line procedure
- Free Tendon Graft (PL/Plantaris)
- When EIP is unavailable (absent, previously used, or injured)
Timing. Operate as soon as the diagnosis is made, ideally within 6–12 weeks of rupture. Beyond about 12 weeks the FPL intrinsic muscle begins to contract and the EPL muscle belly loses excursion, which limits the eventual result. Surgery is still worthwhile in delayed presentations — but the earlier it is done, the better the outcome.
EPL rupture after a distal radius fracture is an attritional, ischaemic rupture — not a clean laceration. Haematoma compresses the EPL in the tight 3rd compartment at Lister's tubercle, and the tendon is abraded against the irregular fracture surface. The result is tendon necrosis, fraying, and a gap defect of 2–4 cm. Approximating the ends under tension means suturing frayed, necrotic tissue that will fail. The gold standard is therefore EIP-to-EPL transfer — a functioning musculotendinous unit that bypasses the damaged EPL entirely.
Consent. Counsel the patient about the splinting and recovery (4–6 weeks protected, full activity by 12–16 weeks), the expected outcome of useful thumb IP extension in the large majority, a small risk of a transfer that is too tight or too loose needing revision, dorsal numbness or a neuroma from a superficial radial nerve branch, and a modest (usually unnoticed) reduction in independent index extension at the donor site.
The Operation
The goal is to harvest a functioning EIP, route it through the 3rd extensor compartment (the EPL's own anatomical line, redirected by Lister's tubercle), and weave it into the EPL distal stump under the correct tension so that the thumb regains active IP extension. The exposure — the three dorsal incisions and identification of the donor, the recipient stump and the routing channel — is laid out as the opening steps below.
- Contents
- APL, EPB
- Relevance to the EIP-to-EPL transfer
- Not disturbed; de Quervain's territory is radial to the field
- Contents
- ECRL, ECRB
- Relevance to the EIP-to-EPL transfer
- Wrist extensors; left undisturbed
- Contents
- EPL
- Relevance to the EIP-to-EPL transfer
- Site of rupture at Lister's tubercle — opened and used as the routing channel
- Contents
- EDC (4 slips), EIP
- Relevance to the EIP-to-EPL transfer
- EIP is harvested here; at the wrist EIP lies ulnar to EDC to index
Lister's tubercle is the dorsal radial bony prominence that acts as a pulley for the EPL, redirecting it radially toward the thumb. The 3rd compartment groove lies on the ulnar side of the tubercle. After a distal radius fracture, haematoma accumulates in this rigid compartment and compresses the EPL's blood supply, while the fracture callus or a step in the floor of the groove abrades the tendon on its deep surface.
Operative sequence
- Supine, arm on a hand table, upper-arm or proximal-forearm tourniquet, loupe magnification (recommended).
- Regional block is suitable; wide-awake local anaesthesia (WALANT) is an option that allows active tensioning before closure (Hong 2020, PMID 32097314).
- Mark the three incision sites before tourniquet inflation so landmarks are easy to identify: the index MCP (EIP harvest), the dorsum of the wrist at Lister's tubercle (the routing channel), and the dorsal thumb over the MCP and proximal phalanx (the EPL stump).
- Incision 1 (EIP harvest): a 3–4 cm longitudinal incision over the index MCP joint, centred on the extensor mechanism.
- Incision 2 (wrist/transfer tunnel): a 3–4 cm longitudinal incision over the dorsum of the wrist at the level of Lister's tubercle.
- Incision 3 (EPL distal stump): a longitudinal incision over the dorsal thumb MCP and proximal phalanx, about 3 cm, to find the EPL stump.
- In the subcutaneous plane identify and protect the superficial radial nerve branches (radial aspect) and the dorsal cutaneous branch of the ulnar nerve (at the index MCP); both are at risk in these incisions.
- Open the index MCP incision and identify the extensor mechanism. The EIP lies ulnar to the EDC slip to the index — confirm it by asking the (awake) patient to extend the index finger while the others are held in a fist before dividing anything.
- Place a locking whipstitch (Kessler or Bunnell) in the EIP tendon about 3–4 cm proximal to the MCP.
- Divide the EIP at its insertion on the ulnar side of the index extensor hood at the MCP joint — taking the correct (ulnar) slip, not the EDC.
- Mobilise the EIP proximally through the subcutaneous plane (or via the wrist incision) to gain adequate length.
- Open the dorsal thumb incision and identify the EPL distal stump, usually found at the level of the thumb MCP or proximal phalanx (it retracts only slightly).
- Place a marking suture and assess tissue quality. If the stump is very short (less than 1 cm), plan to suture the transfer directly into the extensor hood.
- Open the wrist incision over Lister's tubercle and open the 3rd extensor compartment; identify and retract the proximal EPL stump.
- In long-standing ruptures (greater than 3 months) the EPL muscle may be fibrotic with reduced excursion — document this.
- Debride the groove; this compartment becomes the routing channel for the transferred EIP.
- Pass a tendon passer (or curved haemostat) from the wrist incision subcutaneously to the index MCP incision and deliver the EIP to the wrist.
- Route the EIP through the 3rd extensor compartment (the EPL groove at Lister's tubercle) so it follows the EPL's natural line of pull.
- Pass a tendon passer from the wrist incision distally to the thumb incision and deliver the EIP to the thumb level.
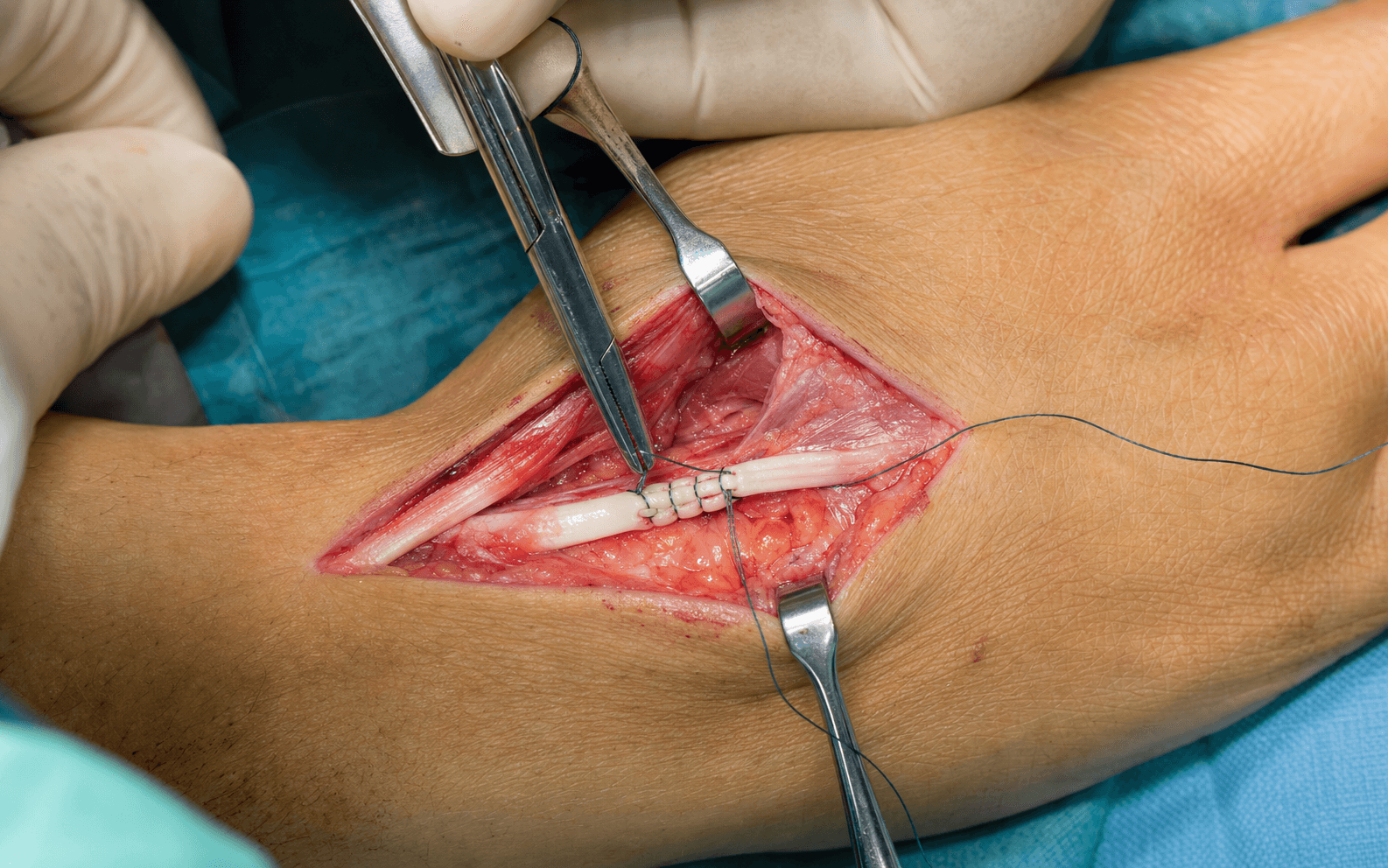
- Perform a Pulvertaft weave: pass the EIP through the EPL distal stump in 2–3 interlacing passes (or a side-to-side suture if the stump is thin).
- Set the tension before the final sutures: wrist at neutral (0°), thumb at full IP extension. At this position the EIP should be on slight tension.
- Tenodesis test: with everything held, passively flex the wrist — the thumb IP should extend further; extend the wrist and the IP should flex slightly. If this tenodesis motion is present, the tension is correct.
- Place 4/0 or 3/0 non-absorbable sutures (Ethibond/Prolene) through all weave passages. If the patient is awake, ask them to actively extend the thumb to confirm.
- Close the extensor retinaculum over the transferred tendon at the wrist.
- Layered closure at all three incisions.
- Release the tourniquet fully and check thumb vascularity.
- Apply a thumb spica splint with the IP in extension and the wrist in neutral to slight extension.
The EIP lies on the ulnar side of the EDC slip to the index. Harvesting the wrong slip (EDC) leaves both the index and the thumb without functional extension. Always confirm by (1) visualising the ulnar slip, and (2) asking the patient to extend the index with the other fingers in a fist before dividing. At the wrist the EIP lies ulnar to EDC in the 4th compartment; at the MCP, trace from the EDC attachment to find the EIP insertion more ulnarly.
Setting the tension with the wrist in extension (not neutral) is the most common mistake. If you set tension with the wrist extended, then when the patient moves the wrist to neutral or flexion the tendon becomes too tight and pulls the IP into flexion. Always use wrist neutral as the reference. A correctly tensioned thumb has: full passive IP extension available, slight IP hyperextension with the wrist at neutral, and a positive tenodesis test.
Opening the 3rd compartment at Lister's tubercle and routing the EIP through it makes the transfer follow the EPL's natural anatomical line, redirected by Lister's tubercle toward the thumb. This preserves the mechanical advantage and line of pull compared with a shallow subcutaneous route.
The operation in pictures




Aftercare & Complications
Rehabilitation | Phase | Duration | Splint | Purpose | |-------|----------|--------|---------| | 1 | 0–3 weeks | Thumb spica with IP in extension; wrist neutral | Protect the Pulvertaft weave while it heals | | 2 | 3–6 weeks | Removable thumb spica; full-time except for exercises | Controlled active range of motion begins | | 3 | 6–10 weeks | Splint for sport and heavy activities | Progressive strengthening | | 4 | 10–16 weeks | No splint | Return to full activities | Exercise protocol - Week 3–4 (protected active motion): gentle active thumb IP extension within the splint; wrist tenodesis exercises (flex and extend the wrist while observing thumb motion). Avoid resisted extension for 6 weeks.
- Week 6–10 (progressive loading): active-assisted thumb extension against gravity; gentle supervised pinch and grip; begin IP flexion while ensuring the transfer is not tethered.
- Week 10–16 (return to function): progressive strengthening; graded manual tasks; return to contact sport generally at 12–16 weeks. Expected outcomes - Active thumb IP extension: useful extension restored in the large majority — excellent-to-good in 11 of 17 (65%) by the dedicated SEEM score (Lemmen 1999, PMID 10190604); the extension lag is reliably abolished when the tendon is coapted with the thumb in full extension (Lee 2015, PMID 26418770).
- Pinch and grip strength: generally returns toward, but slightly below, the contralateral side.
- Index function (donor): independent index extension preserved; index extension strength reduced by about 38% (Lemmen 1999) — usually subclinical and seldom noticed in daily activity.
- Return to work: desk work at 6–8 weeks; manual work at 12–16 weeks.
In isolation, harvesting EIP produces minimal functional deficit for most patients. EDC to the index remains intact and provides adequate index MCP extension for daily activities. Patients who notice the deficit are those who type extensively, play keyboard instruments, or need independent index extension with the other fingers flexed. Counsel everyone, but reassure them the vast majority have no functional limitation. Lemmen 1999 (PMID 10190604) found no marked loss of independent index extension after EIP harvest, with only about a 38% reduction in index extension strength — measurable but generally subclinical, and not outweighed by the benefit of restoring thumb extension.
Complications
- Incidence
- 5–10%
- Recognition
- Cannot actively extend the thumb IP postoperatively; the IP droops into flexion
- Prevention
- Set tension at wrist neutral with the thumb fully extended; confirm the tenodesis test intra-operatively
- Management
- Early revision (within 3–6 weeks): re-tension the Pulvertaft weave. Late: revision with a new weave or free graft
- Incidence
- 5–10%
- Recognition
- Thumb IP held in fixed flexion; cannot flex despite trying; wrist extension worsens it
- Prevention
- Tenodesis test: wrist flexion should produce thumb extension, not a fixed flexed position
- Management
- Surgical revision: release one or more weave sutures to reduce tension and re-set
- Incidence
- Less than 1% if careful
- Recognition
- Intra-operative loss of active index extension; post-op weak index extension and no thumb extension
- Prevention
- Confirm EIP by active index extension in a fist; identify the ulnar slip before dividing
- Management
- If EDC harvested: replace it and proceed with a free tendon graft for the EPL
- Incidence
- 5–10%
- Recognition
- Numbness or dysaesthesia over the dorsal thumb/index; neuroma pain
- Prevention
- Loupe magnification; identify and retract the superficial radial nerve branches
- Management
- Usually resolves over 3–6 months; persistent neuroma: desensitisation, steroid injection, excision
- Incidence
- 10–20%
- Recognition
- Restricted IP motion despite adequate tension; restricted tendon glide
- Prevention
- Early protected motion from week 3–4; loupe-guided gentle dissection
- Management
- Hand therapy; tenolysis at 6 months if no further improvement
- Incidence
- Less than 3%
- Recognition
- Sudden loss of extension after a period of good function
- Prevention
- Avoid heavy use for 12 weeks; supervised rehabilitation
- Management
- Exploration and revision; free graft if the EIP stump is insufficient
- Incidence
- Less than 1%
- Recognition
- Wound erythema, discharge, fever
- Prevention
- Prophylactic antibiotics; careful skin handling
- Management
- Antibiotics; debridement if deep, with tendon protection
A patient has an EIP-to-EPL transfer and now has full thumb IP extension but a floppy index MCP that will not straighten. This suggests the EDC to the index was harvested instead of the EIP. EDC to index is the primary MCP extensor for the index; without it the patient cannot straighten the index MCP (the intrinsic muscles extend the IP joints, not the MCP). If missed at surgery it must be addressed — options include a transfer using EIP of the little finger (EIM) if available, a free graft bridging the EDC gap, or an ECRB transfer. This is exactly why confirming EIP identity before harvesting is critical: test by active index extension in a fist before dividing.
Viva & Exam Focus
EPLEPL — Aetiology of Rupture
Hook:EPL rupture arises in three settings: post-fracture (conservatively managed), post-ORIF (hardware abrasion), and rheumatoid (tenosynovitis). The classic exam question is post-fracture at 6–8 weeks after an apparently well-managed non-displaced fracture.
TRANSFERTRANSFER — the EIP-to-EPL technique in sequence
Hook:TRANSFER in order is the 8 steps of EIP-to-EPL in sequence. The two steps that decide the result are T (test the donor first) and F (set the correct tension) — tension errors are the commonest cause of a poor outcome.
Spontaneous EPL rupture classically occurs 6–8 weeks after a distal radius fracture — including non-displaced and minimally displaced fractures managed conservatively. The mechanism is ischaemia from haematoma compressing the 3rd compartment at Lister's tubercle, combined with abrasion on the irregular fracture-callus surface. Examine every distal radius fracture patient at 6 weeks for EPL integrity (the lift-off test).
EPL rupture is an attritional, ischaemic rupture — not a clean laceration. The tendon ends are frayed, necrotic and retracted, with a gap defect of 2–4 cm that cannot be bridged without unacceptable tension. Even if the ends could be approximated, the tissue quality is poor and the re-rupture rate is very high. This is why EIP-to-EPL transfer (or a free tendon graft) is the gold standard, rather than direct repair.
Test the EIP by asking the patient to make a full fist (all fingers flexed) and then independently extend the index finger. In a fist the EDC is held passively slack — only the EIP can actively extend the index MCP. Confirm the EIP is working before planning the transfer. The EIP lies ulnar to EDC to index at MCP level — essential for correct identification during harvest.
Tension is the most technically demanding step. Correct tension: with the wrist at neutral and the thumb in full extension, the transferred EIP holds the IP in slight hyperextension. Too loose gives no active IP extension. Too tight holds the IP in fixed flexion. Confirm intra-operatively by moving the wrist from flexion to extension and watching the IP (the tenodesis test).
Lister's tubercle is a bony prominence on the dorsal distal radius that acts as a pulley redirecting the EPL toward the thumb. The 3rd extensor compartment (EPL) runs in the groove on its ulnar side. In distal radius fractures, haematoma accumulates in this tight compartment and compresses the EPL. In ORIF the tubercle may be displaced or a dorsal screw may breach the compartment floor, also endangering the EPL.
EPL rupture also occurs in rheumatoid arthritis from dorsal wrist tenosynovitis at Lister's tubercle. Key differences: it may be bilateral; active synovitis must be treated (synovectomy at the time of transfer); the extensor retinaculum may need reconstruction or transposition beneath the tendons to protect the repair; and the adjacent extensors (EDC to ring and little) must be checked, as RA causes multiple simultaneous ruptures — the Vaughan-Jackson ulnar cascade.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 55-year-old woman fell on her outstretched hand 8 weeks ago and was treated conservatively for a non-displaced distal radius fracture. She now presents with inability to extend her thumb. What is the diagnosis and how do you manage it?”
“Describe how you test the EIP clinically and why this is important before an EIP-to-EPL transfer. What would you do if the EIP were absent or damaged?”
“At 6 weeks after an EIP-to-EPL transfer the patient has active wrist extension but the thumb IP drops into flexion and she cannot actively extend it. What has happened and what is your management?”
EPL rupture — diagnosis
- Classic timing: 6–8 weeks after a distal radius fracture (non-displaced or minimally displaced)
- Mechanism: ischaemia from haematoma in the tight 3rd compartment at Lister's tubercle plus abrasion on the callus
- Clinical test: EPL lift-off — cannot lift the thumb off a flat table (retropulsion lost)
- Also occurs in RA (dorsal tenosynovitis), after ORIF (hardware abrasion), and rarely spontaneously
- Direct repair FAILS — attritional gap defect with poor tissue quality; EIP transfer is the gold standard
Why EIP transfer, not direct repair
- Attritional rupture = frayed, necrotic tendon ends with a 2–4 cm gap defect
- Approximating the ends under tension sutures poor-quality tissue — re-rupture is inevitable
- EIP transfer provides a functioning motor unit that bypasses the damaged EPL
- EIP present in about 99.5% of patients; a reliable donor
- If EIP unavailable: a free tendon graft (PL or plantaris) is the alternative
EIP anatomy and test
- EIP origin: posterior ulna and interosseous membrane (distal third, distal to EDC)
- EIP lies ULNAR to EDC to index at MCP level — confirm before harvesting
- EIP test: full fist (all fingers flexed), then extend the index alone — only the EIP can do this
- Lies ulnar to EDC in the 4th compartment at the wrist
- Transferred through the 3rd compartment (the EPL route) at Lister's tubercle
Tension setting — the most critical step
- Set tension with the wrist at NEUTRAL (0°) and the thumb at FULL IP extension
- Correct tension: slight IP hyperextension with the wrist at neutral
- Tenodesis test: wrist flexion produces thumb IP extension; wrist extension produces IP flexion
- Too loose: no active IP extension; the thumb droops
- Too tight: the IP is held in fixed flexion; wrist extension worsens it
Operative steps
- Incision 1: index MCP (EIP harvest) — the ulnar slip; confirm by the fist test
- Incision 2: dorsal wrist at Lister's tubercle (route EIP through the 3rd compartment)
- Incision 3: dorsal thumb (Pulvertaft weave to the EPL distal stump)
- Route the EIP through the 3rd compartment (not subcutaneously) — it follows the EPL line
- Pulvertaft weave of 2–3 passes; 3/0 or 4/0 non-absorbable sutures
Complications
- Too loose (5–10%): no IP extension; revision — re-tension the Pulvertaft weave
- Too tight (5–10%): IP in fixed flexion; revision — release one weave suture
- EIP misidentification (less than 1%): EDC harvested instead — confirm by the fist test
- Adhesions (10–20%): restricted glide; tenolysis at 6 months if refractory
- Sensory nerve injury (5–10%): superficial radial nerve; usually resolves
Post-operative protocol
- Thumb spica with IP in extension; wrist neutral: 0–3 weeks
- Removable splint; protected active ROM from week 3–4
- Progressive strengthening from week 6; full activities from week 12–16
- Outcome: excellent-to-good IP extension in about 65% by SEEM (Lemmen 1999, PMID 10190604); lag abolished when coapted in full extension (Lee 2015, PMID 26418770)
- Index deficit: minimal — EDC maintains MCP extension; about a 38% drop in index extension strength but usually unnoticed
Key evidence and references
- Lee 2015 (PMID 26418770): coapt the thumb in FULL extension (+7.2° IP), not neutral (-5.2° lag)
- Lemmen 1999 (PMID 10190604): 17 cases; excellent-good in 65%; index extension strength down about 38%, independent extension preserved
- Hong 2020 (PMID 32097314): wide-awake (WALANT) transfer gives better early ROM than general anaesthesia
- Bonatz 1996 (PMID 8640381): post-fracture rupture at a median 7 weeks; both EIP transfer and PL graft give good results
- Saito 2025 (PMID 40449182): a fracture line distal to Lister's tubercle and a shallow/radial-peaked tubercle increase rupture risk
- RA EPL rupture: add a synovectomy to the transfer; check for the Vaughan-Jackson ulnar cascade
- Timing: operate within 4–12 weeks; delay beyond 12 weeks risks FPL contracture and reduced excursion
Background & Evidence
Epidemiology. Spontaneous EPL rupture is the classic late complication of a distal radius fracture, arising 6–8 weeks after injury — including non-displaced and minimally displaced fractures managed conservatively. The reported incidence after non-displaced fractures ranges from about 0.07 to 5 percent (Bogart 2020, PMID 30550417). Rupture also occurs in rheumatoid arthritis (from dorsal wrist tenosynovitis at Lister's tubercle), after ORIF (hardware abrasion or a dorsal screw penetrating the 3rd compartment floor), and rarely as a truly spontaneous event. Pathoanatomy and mechanism. The EPL runs in the 3rd extensor compartment, in the groove on the ulnar side of Lister's tubercle, which acts as a pulley redirecting the tendon toward the thumb. After a distal radius fracture two mechanisms combine: a haematoma accumulates in the tight, unyielding compartment and compresses the EPL's precarious blood supply (ischaemia), while the fracture callus or a step on the floor of the groove abrades the tendon on its deep surface where it hooks around the tubercle. The result is an attritional, ischaemic rupture with frayed, necrotic ends and a 2–4 cm gap — which is why direct repair fails. Saito 2025 (PMID 40449182) showed that a fracture line lying distal to Lister's tubercle and a tubercle with a shallow peak (radial peak higher than ulnar) significantly increase rupture risk, whereas the size and location of the tubercle alone do not. Key evidence. The modern tension target comes from Lee 2015 (PMID 26418770): in a prospective comparison of 24 transfers, coapting the tendon with the thumb IP in full extension achieved a mean +7.2° of extension, while coapting in neutral left a -5.2° lag — a significant difference. Lemmen 1999 (PMID 10190604), a 17-case outcome series using the dedicated SEEM score, found excellent-to-good thumb extension in 65%, with no marked loss of independent index extension and only a modest (~38%) reduction in index extension strength. Hong 2020 (PMID 32097314) showed that a wide-awake (WALANT) transfer — which allows active tensioning before closure — gives better early range of motion than general anaesthesia, with equivalent extension and strength. Bonatz 1996 (PMID 8640381) confirmed the classic post-fracture timing (median 7 weeks) and that both EIP transfer and a free palmaris longus graft give good results. Ha 2024 (PMID 38296255) reports the clinical outcomes of EIP-to-EPL transfer for EPL rupture. The consistent message — an attritional rupture that cannot be directly repaired, reconstructed reliably with an EIP transfer tensioned at wrist neutral with the thumb in full extension — is why this is a perennial viva favourite.
References
A New Method to Control Tendon Tension in EIP-to-EPL Transfer
- Prospective comparative study of 24 EIP-to-EPL transfers, all coapted with the wrist in neutral
- Group sutured with the thumb IP in FULL extension achieved +7.2° IP extension; group sutured in NEUTRAL achieved -5.2° (an extension lag) — statistically significant
- No significant difference in grip, pinch or DASH between groups
- Slight intentional over-tensioning (EIP elongation ~0.7 cm vs ~0.2 cm) reliably abolished the extension lag
Evaluation of Restoration of Extensor Pollicis Function by Transfer of the Extensor Indicis
- Long-term outcome series of 17 EIP-to-EPL transfers assessed with a dedicated SEEM scoring tool
- Excellent-to-good thumb extension in 11 of 17 patients (65%)
- No marked loss of independent index extension at the donor site
- Index extension strength reduced by ~38% — donor morbidity is measurable but functionally well tolerated
Wide-Awake vs Conventional EIP-to-EPL Transfer for Chronic EPL Rupture
- Comparative study of 29 transfers: WALANT (wide-awake) n=11 vs general anaesthesia n=18
- Wide-awake group had significantly better IP and MCP flexion and total arc of motion, especially in the early post-operative period
- IP/MCP EXTENSION did not differ between groups — both restored extension well
- No difference in grip/pinch strength, complication rate or time to return to work
Rupture of the Extensor Pollicis Longus Tendon
- Retrospective series of 7 EPL ruptures; 5 followed non-displaced distal radius fracture
- Median time from fracture to rupture was 7 weeks (range 2 weeks to 11 months)
- 3 treated with EIP transfer, 4 with free palmaris longus graft
- 6 of 7 finished with an IP extensor lag under 10° or normal IP motion
Risk Factors for EPL Rupture Following Non-Displaced Distal Radius Fractures
- Multicentre case-control study: 20 EPL ruptures vs 52 controls after non-displaced distal radius fracture
- A fracture line DISTAL to Lister's tubercle significantly increased rupture risk
- A Lister's tubercle with a shallow peak and a radial peak higher than the ulnar peak increased risk
- Size and location of Lister's tubercle alone did not predict rupture
Ruptured EPL Tendon After a Nondisplaced Distal Radius Fracture in a Young Adult Soccer Player
- Case report of spontaneous EPL rupture after a nondisplaced distal radius fracture in a young adult
- Illustrates that rupture occurs even in young, active patients after apparently minor, nondisplaced injuries
- Cited for the reported incidence of EPL rupture after nondisplaced distal radius fractures (~0.07–5%)
Clinical Outcomes of Extensor Indicis Proprius Tendon Transfer for Extensor Pollicis Longus Tendon Rupture
- Contemporary clinical outcomes series of EIP-to-EPL tendon transfer for EPL rupture
- Reports the functional results of the standard transfer in a modern cohort
- Adds to the body of evidence that EIP transfer reliably restores thumb extension