Basal thumb (first carpometacarpal) osteoarthritis · Eaton-Littler II–IV
- The operation is excision of the arthritic trapezium. Adding a ligament reconstruction and tendon interposition (LRTI) or a suture-button suspension is OPTIONAL — high-level RCT evidence shows no outcome benefit over trapeziectomy alone, and LRTI adds donor morbidity and complications.
- Identify and protect the radial artery in the field BEFORE removing the trapezium, and take the trapezium piecemeal — en-bloc removal risks the artery.
- Protect the superficial radial nerve branches (2–3 mm deep, crossing the incision) and the FCR tendon in its groove on the volar trapezium.
- Release a tight adductor pollicis in advanced disease, otherwise the thumb will not regain its span.
- Splint the thumb in palmar abduction (the functional position), not flat in the palm.
When & Why
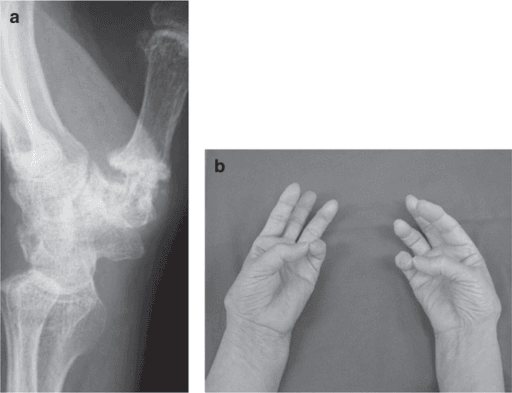
Indication. Symptomatic basal thumb (first CMC) osteoarthritis — pain at the thumb base on pinch and grip, tenderness over the CMC joint, and a positive grind test (axial load plus rotation reproduces pain) — with Eaton-Littler Stage II–IV disease on radiographs, that has failed conservative treatment (activity modification, a thumb spica splint, NSAIDs and at least one intra-articular corticosteroid injection). Stage I disease, and disease that has not had a fair trial of non-operative care, is managed without surgery. Assess the whole thumb ray, not just the CMC joint. Before committing, exclude or plan for:
- Scaphotrapeziotrapezoid (STT) involvement (pantrapezial / Stage IV disease) — it changes nothing about the trapeziectomy itself but must be recognised and the patient counselled.
- MCP hyperextension (the compensatory Z-deformity) — if the MCP hyperextends more than about 30 degrees it should be addressed at the same sitting (volar capsulodesis, sesamoid arthrodesis, K-wire or even MCP fusion), or the correction at the CMC will be lost.
- A fixed adductor contracture, which you will need to release to restore span. The one decision that matters. Whatever you add, every technique begins with the same step — complete excision of the trapezium. The only real choice is what (if anything) you do afterwards:
Simplest, shortest, no donor morbidity. The benchmark — RCT-equivalent to LRTI at 1 and 5 years and the evidence-based default.
Adds a ligament-reconstruction tendon-interposition (an FCR suspensory sling plus an interposition "anchovy"). No proven outcome benefit and a higher complication rate.
A suture-button (e.g. TightRope) suspends the thumb metacarpal off the index metacarpal — no tendon harvest and faster recovery, but limited long-term data and hardware-specific complications (button migration, prominence).
Consent specifically for radial-sided numbness or a tender neuroma, scar tenderness/pillar pain, some loss of pinch strength, a small risk of incomplete pain relief, and (if LRTI) FCR donor-site symptoms. Setup. Supine, arm on a hand table, upper-arm tourniquet, regional (axillary/supraclavicular) block. Position the thumb in abduction and opposition to relax the thenar muscles. Loupe magnification (×2.5–×3.5) is mandatory — nerve and vessel identification is the whole game.
The Operation
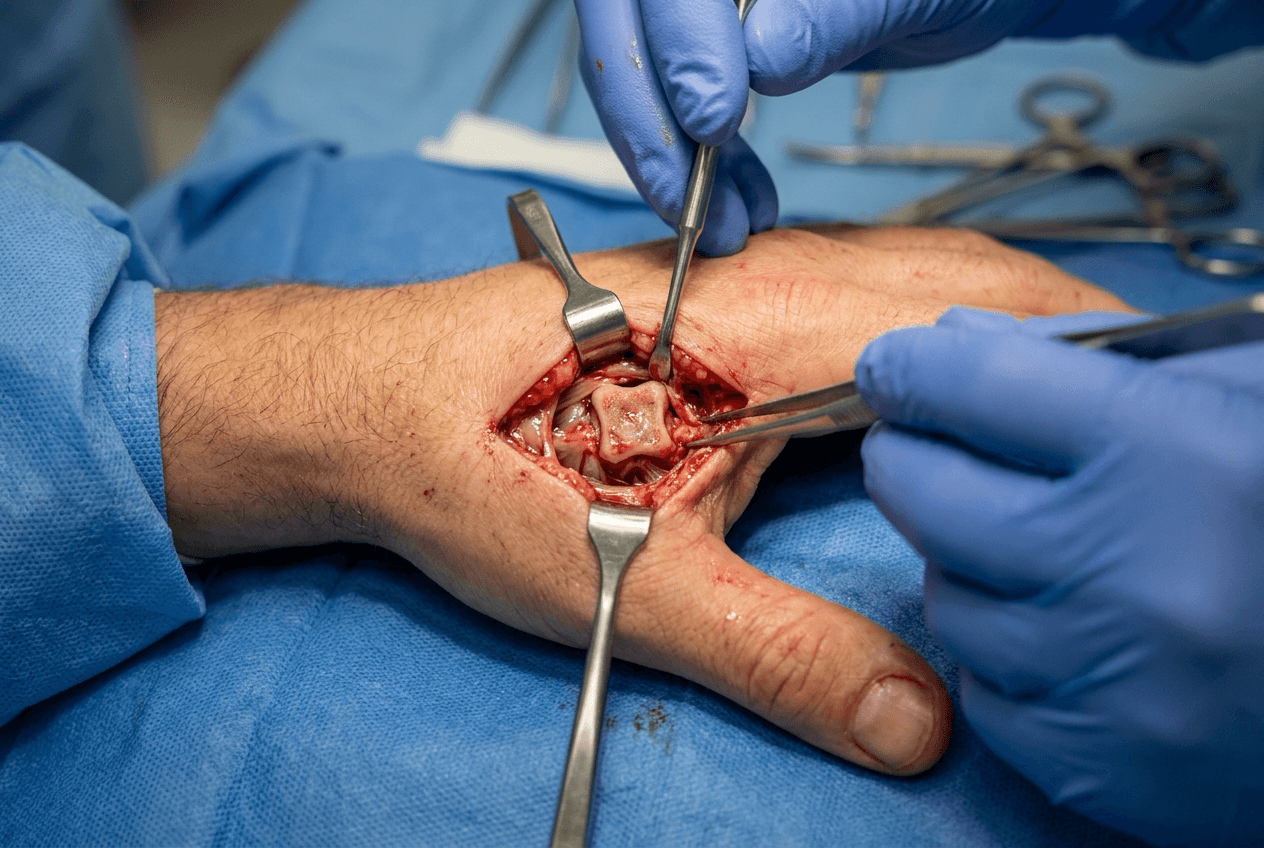
The goal: expose the joint through the Wagner volar approach, remove the arthritic trapezium completely while protecting the radial artery, the FCR and the superficial radial nerve, restore thumb span, and stabilise the thumb in palmar abduction. The exposure is laid out in full below (and in depth on the Wagner approach to the first CMC joint page).
Operative sequence
- Supine, hand table, upper-arm tourniquet, thumb in abduction/opposition, loupes on.
- Mark the landmarks: the trapezium (palpable in the snuffbox and volarly at the thenar eminence), the first metacarpal base, the scaphoid tubercle (proximal limit), and the glabrous–non-glabrous skin junction along the thenar eminence, which defines the incision line.
- A curved incision beginning about 1 cm proximal to the scaphoid tubercle along the radial border of FCR, curving distally along the thenar crease at the glabrous–non-glabrous junction to the midshaft of the first metacarpal (typically 5–7 cm).
- The curve allows proximal extension (along the radial artery) and distal extension as needed.
- In the subcutaneous plane, identify and retract the superficial radial nerve branches — they cross the field only 2–3 mm deep and are the structure most often injured (numbness or a painful neuroma).
- Identify the radial artery; it courses dorsally toward the first web but branches cross the field. Control or ligate branches as needed and protect the main vessel. This is done before any bone work.
- Elevate the thenar muscle origins (abductor pollicis brevis, opponens pollicis, flexor pollicis brevis superficial head — all median-innervated) subperiosteally off the trapezium and metacarpal base.
- The exposure works the internervous plane between the thenar muscles (median nerve) and adductor pollicis (ulnar nerve); the adductor, on the ulnar side of the metacarpal base, is not elevated.
- This avoids the first dorsal compartment tendons (APL, EPB) that a dorsal approach would risk.
- Open the capsule in a T-fashion (longitudinal limb over the CMC joint, transverse limb at the metacarpal base) and tag the flaps for later repair.
- Inspect the surfaces and confirm the Eaton stage. In Stage IV the STT joint is arthritic but is not separately replaced.
- Dissect subperiosteally around the trapezium.
- Remove it in pieces with an osteotome and rongeur — splitting it first (a central trough) and delivering fragments is far safer for the radial artery than levering it out en-bloc.
- Protect the FCR tendon running in its groove on the volar surface of the trapezium — it forms the floor of the excision.
- Clear every fragment, including dorsal and volar osteophytes; confirm a clean trapezial void and palpate the scaphoid proximally (its articular surface should be intact and smooth).
- Test passive thumb abduction from the palmar plane.
- If the adductor pollicis is contracted (common in Stage III–IV), release its fascia/origin until full abduction is achieved — otherwise the thumb stays adducted and pinch is weak.
- Trapeziectomy alone — pack the void with absorbable haemostatic material or leave it empty; this is the evidence-based default. Proceed to closure.
- Otherwise continue to LRTI or a suture-button suspension (Step 9).
LRTI (ligament reconstruction + tendon interposition):
- Harvest the radial half of FCR through a second short proximal wrist incision, dividing it proximally with a tendon stripper and leaving its distal insertion intact.
- Drill a dorsal-to-volar tunnel in the thumb metacarpal base, about 1 cm from the articular surface.
- Pass the FCR slip through the tunnel, loop it on itself to create a suspensory sling, and suture it under tension (see the safety note below).
- Fold the remaining tendon into a ball — the "anchovy" — and pack it into the trapezial void as an interposition spacer.
- Repair the capsule over the anchovy. Suspensionplasty (suture button): after trapeziectomy a suture-button device suspends the thumb metacarpal off the index metacarpal — no tendon harvest and earlier mobilisation, at the cost of hardware-specific complications.
- Repair the capsule and re-approximate the thenar origin (and the released adductor) to restore the soft-tissue sleeve.
- Layered closure; release the tourniquet and confirm thumb perfusion.
- A temporary K-wire may hold the metacarpal in abduction (surgeon preference, especially with suspension).
- Apply a thumb spica with the thumb in palmar abduction.
Before any trapezium removal, identify the radial artery and its branches in the field. The artery passes between APL/EPB and EPL in the snuffbox and crosses toward the first web to enter the deep palm. Protect the main vessel, control branches deliberately, and remove the trapezium piecemeal rather than en-bloc. If the artery is injured: direct pressure, call for vascular help, and repair primarily where possible — confirm the ulnar artery and a complete palmar arch before sacrificing it.
After threading FCR through the metacarpal tunnel and before the final suture, hold the wrist neutral and the thumb in maximum abduction/opposition, tension the sling until the metacarpal base lifts off the scaphoid (feel the gap open), then secure it. Under axial load the metacarpal should not migrate proximally more than 3–4 mm.
The Wagner volar approach keeps you away from the first dorsal compartment tendons (APL, EPB) and works the internervous plane between the thenar muscles (median) and adductor pollicis (ulnar). A dorsal approach risks those tendons and the dorsal radial artery branches — reserve it for specific indications such as Bennett-fracture work.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 | 0–2 weeks | Thumb spica cast (K-wire removed at ~4 weeks if used) | Finger active range of motion only | | 2 | 2–6 weeks | Removable thumb spica splint | Gentle thumb IP and wrist motion; scar care from 6 weeks | | 3 | 6–10 weeks | Splint for heavy tasks | Progressive CMC motion, light pinch | | 4 | 10–16 weeks | Night splint only | Strengthening, graded return to function | Most patients return to desk work by about 6 weeks and heavy manual work by 12–16 weeks. Around 85–90 percent report significant pain relief, with grip and pinch recovering to roughly 85–90 percent of the other side by a year, and high satisfaction at 5 years. Radiographic proximal migration of the metacarpal (subsidence into the void) is expected and usually asymptomatic. Complications
- Recognition
- Numbness or dysaesthesia over the thumb/dorsum; a tender Tinel sign at the scar
- Prevention
- Subcutaneous dissection under loupe; identify and retract branches
- Management
- Usually settles; persistent neuroma — desensitisation, injection, excision
- Recognition
- Arterial bleeding in the field; expanding haematoma
- Prevention
- Identify and protect the artery first; remove the trapezium piecemeal
- Management
- Direct pressure, primary repair, vascular help; confirm ulnar inflow first
- Recognition
- Proximal metacarpal migration on radiograph with pain on pinch
- Prevention
- Splint in abduction; suspension may reduce migration (no proven outcome benefit)
- Management
- Conservative first; revision suspension only if genuinely refractory
- Recognition
- A sensitive scar and restricted motion in early recovery
- Prevention
- Meticulous closure; scar massage and silicone from 6 weeks
- Management
- Massage, silicone, desensitisation therapy
- Recognition
- Wrist flexion weakness, tendon adhesion, wrist pain
- Prevention
- Careful radial half-width harvest
- Management
- Therapy; rarely re-exploration
- Recognition
- Recurrent Z-collapse, weak pinch
- Prevention
- Address MCP hyperextension greater than 30 degrees at the index operation
- Management
- Volar capsulodesis, sesamoid arthrodesis or MCP fusion
- Recognition
- Allodynia, swelling, disproportionate pain
- Prevention
- Minimise tourniquet time; gentle handling; early motion
- Management
- Pain team, hand therapy, sympathetic blockade
Viva & Exam Focus
TRAPEZIUMTRAPEZIUM — order of the operation
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 62-year-old woman has basal thumb pain failing splints and an injection. How do you decide between trapeziectomy alone and LRTI?”
“At 6 months a patient has proximal metacarpal migration on radiograph and pain on pinch. How do you manage this?”
Indication
- Eaton-Littler II–IV basal thumb OA failing conservative care
- Positive grind test; assess the STT and MCP joints
Exposure
- Wagner VOLAR approach along the thenar crease
- Internervous plane: thenar (median) versus adductor (ulnar)
- At risk: superficial radial nerve, radial artery
Core operation
- Trapeziectomy — complete, piecemeal, protect the FCR
- LRTI or suspension is OPTIONAL and only RCT-equivalent
Finish
- Release the adductor if contracted
- Address MCP hyperextension over 30 degrees
- Splint in palmar abduction
Background & Evidence
Epidemiology. Basal thumb osteoarthritis is the second most common site of hand OA after the DIP joints. It affects roughly 15 percent of post-menopausal women radiographically (lower symptomatic prevalence), with a strong female predominance and a peak in the fifth to seventh decades; it is frequently bilateral. Pathoanatomy. Disease begins with attenuation of the volar (beak) ligament, the primary stabiliser of the trapeziometacarpal joint. Laxity allows dorsoradial subluxation of the metacarpal base, abnormal contact stresses and progressive cartilage wear. As the metacarpal migrates the adductor pollicis shortens, producing a fixed adduction contracture, and the MCP joint hyperextends to compensate — the classic thumb Z-deformity. Advanced disease spreads to the STT joint (pantrapezial / Stage IV).
- Radiographic features
- Normal or slightly widened joint; subluxation less than one-third; no osteophytes
- Typical management
- Splint, activity modification, injection
- Radiographic features
- Joint-space narrowing with osteophytes or loose bodies less than 2 mm
- Typical management
- Conservative first; trapeziectomy if it fails
- Radiographic features
- Marked narrowing, subchondral sclerosis and cysts, osteophytes greater than 2 mm
- Typical management
- Trapeziectomy with or without suspension
- Radiographic features
- Pantrapezial disease — the STT joint is also involved
- Typical management
- Trapeziectomy (the STT joint is not separately replaced)
Key evidence. Davis (2004) randomised trapeziectomy versus trapeziectomy with tendon interposition versus full LRTI and found no difference in pain, strength or satisfaction at one year. The same cohort at five years (Gangopadhyay, 2012) confirmed equivalence. The Cochrane systematic review (Wajon, 2015) found no technique superior and that LRTI carried more complications. This consistent message — adding ligament reconstruction or interposition does not improve outcomes and adds morbidity — is why trapeziectomy alone is the evidence-based default and a perennial viva favourite.
References
Trapeziectomy alone vs interposition vs LRTI — randomised trial
Randomised three techniques for basal thumb OA; no difference in pain, strength or satisfaction at one year — the basis for trapeziectomy alone.
Trapeziectomy with or without LRTI — five-year follow-up
Five-year results of the randomised cohort confirmed equivalence between trapeziectomy alone and LRTI, with no advantage to the added reconstruction.
Surgery for thumb (trapeziometacarpal) osteoarthritis — systematic review
No surgical technique demonstrated superiority; LRTI was associated with a higher complication rate than trapeziectomy alone.
Ligament reconstruction for the painful thumb carpometacarpal joint — original staging
The original description of basal thumb instability and the staging system that still guides management.