Emergency decompression of forearm compartment syndrome · four compartments, two incisions, never closed primarily
- Pain on passive finger extension (stretching the volar flexors) is the most sensitive clinical test for volar compartment syndrome; pain on passive flexion tests the dorsal compartment. The clinical picture always takes precedence over pressure measurements.
- The forearm has FOUR compartments — superficial volar (PT, FCR, PL, FCU, FDS), deep volar (FDP, FPL, PQ with the AIN), mobile wad (BR, ECRL, ECRB) and dorsal extensor (with the PIN). All four must be completely decompressed.
- The volar incision MUST cross the wrist in a zig-zag pattern (never a straight line, which causes a flexion contracture) and extends into the carpal tunnel for prophylactic median-nerve release.
- Decompress when the absolute compartment pressure is greater than 30 mmHg or the delta pressure (diastolic minus compartment) is less than 30 mmHg — but in a clear clinical case, never delay surgery for a measurement.
- Radial and ulnar pulses can remain present because of extensive collateral circulation — never wait for pulselessness. Never close a fasciotomy primarily; plan a second look at 48 to 72 hours.
When & Why
Indication. Forearm compartment syndrome — a surgical emergency. The diagnosis is primarily clinical: pain out of proportion to the injury, a tense rock-hard forearm, and the single most sensitive test, pain on passive finger extension (which stretches the ischaemic volar flexors). Once the diagnosis is made clinically in a high-risk limb, decompress immediately — delay beyond 6 to 8 hours risks irreversible Volkmann's ischaemic contracture. High-risk injuries that demand a high index of suspicion: - Supracondylar humerus fractures — the leading paediatric upper-limb cause; overall incidence is low (under 1 percent) but rises sharply with vascular injury, the pink pulseless hand, or a median/AIN deficit.
- Both-bone forearm fractures — especially high-energy, displaced, or after manipulation.
- Crush injuries — direct forearm compression, prolonged extrication.
- Arterial injection injuries — intra-arterial drug injection causing chemical injury and swelling.
- Reperfusion after vascular repair — ischaemia of more than 4 to 6 hours followed by revascularisation.
- Burns — circumferential or deep burns with eschar constriction.
- Timing and significance
- Earliest and most reliable sign; pain on passive finger extension is the most sensitive test
- Timing and significance
- Tense on palpation; the compartment feels woody
- Timing and significance
- Extension tests the volar compartments, flexion tests the dorsal — most sensitive test
- Timing and significance
- Median/ulnar distribution; intrinsic-minus positioning
- Timing and significance
- LATE signs — pulses often remain present due to collateral circulation; paralysis indicates established damage
Pressure measurement is reserved for when the diagnosis is uncertain — the unconscious, obtunded, or uncooperative patient, or an equivocal exam. Insert the needle perpendicular to the fascia at the zone of maximal swelling and measure each of the four compartments. Normal resting pressure is 0 to 8 mmHg. Fasciotomy is indicated when the absolute pressure is greater than 30 mmHg, or the delta pressure (diastolic minus compartment) is less than 30 mmHg. In children, some use an absolute pressure greater than 20 mmHg or a delta less than 40 mmHg.
Do NOT delay surgery for pressure measurements when the clinical diagnosis is clear. Compartment syndrome is primarily a CLINICAL diagnosis. A high-risk injury (supracondylar fracture with vascular compromise) plus pain on passive stretch equals emergent fasciotomy regardless of any pressure reading.
Document a neurovascular baseline before surgery — median nerve (APB opposition, sensation to thumb/index/middle), ulnar nerve (interossei/ADM, small/ring sensation), radial nerve (wrist/finger/thumb extension, first web sensation), AIN (FPL and index FDP — pinch, purely motor), and vascular status (radial and ulnar pulses, capillary refill, hand perfusion). This protects the patient and the medicolegal record. Consent for the open wounds, the high likelihood of a skin graft (60 to 80 percent), nerve injury, possible muscle loss and contracture, the second-look operation, and the prolonged rehabilitation. Setup. Supine, arm on a radiolucent arm board, shoulder abducted 80 to 90 degrees, forearm supinated for the volar approach (then pronated for the dorsal). Apply an upper-arm tourniquet but do not inflate it — you must be able to assess perfusion and bleeding. Prepare the entire limb shoulder to fingertips and drape to allow repositioning. Have vascular surgery available if an arterial injury is suspected.
The Operation
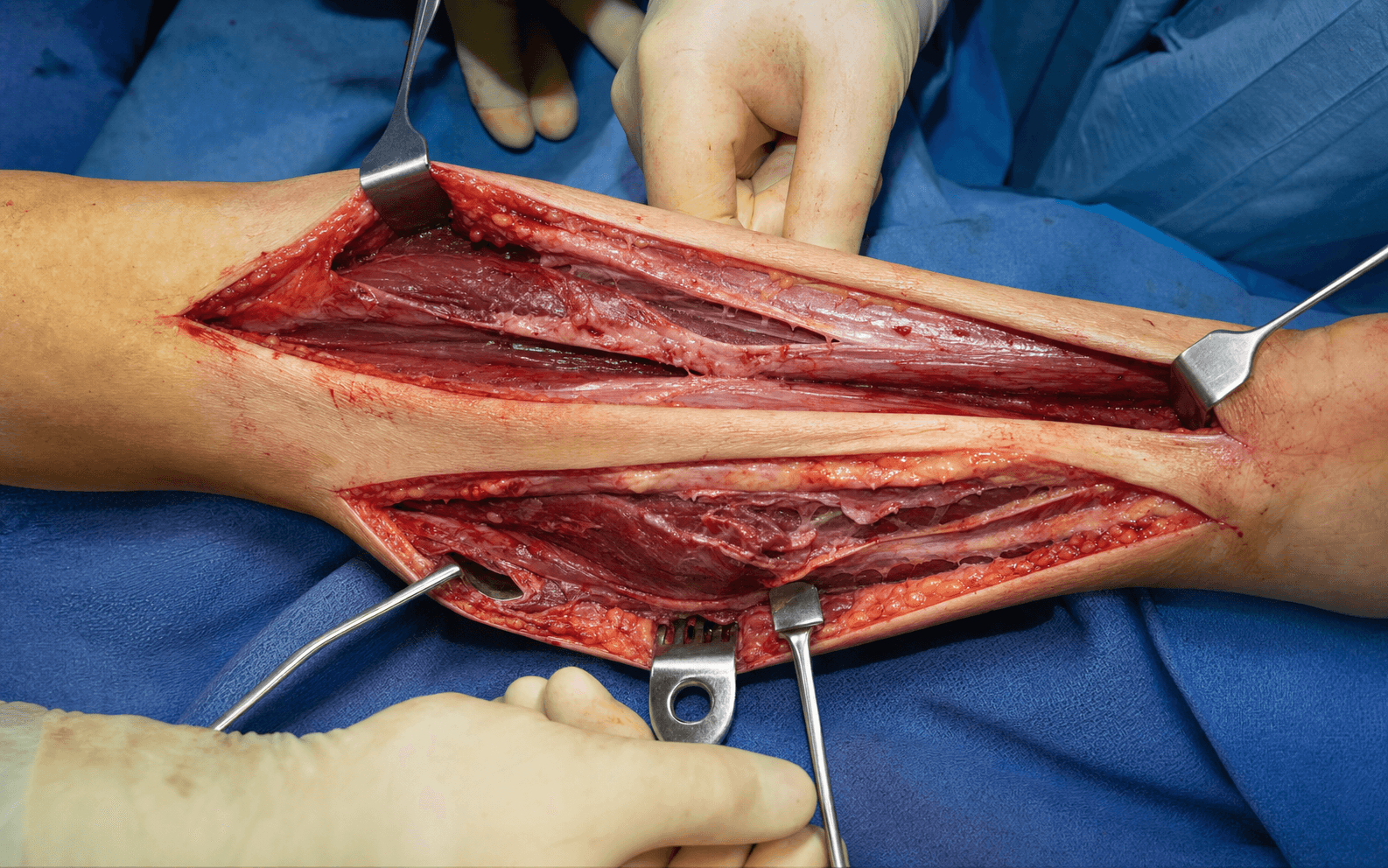
The goal: completely decompress all four compartments through a volar curvilinear incision (superficial volar, deep volar, mobile wad, with extension into the carpal tunnel) and a dorsal longitudinal incision (mobile wad and extensor compartment), then leave every wound open. The exposure and the order of release are laid out step by step below — this is the heart of the operation.
Operative sequence
- Supine, arm on a radiolucent arm board, shoulder abducted 80 to 90 degrees. Forearm supinated for the volar approach, then pronated for the dorsal.
- Apply an upper-arm tourniquet but do NOT inflate it — you must assess perfusion and bleeding.
- Prepare the entire upper limb shoulder to fingertips; drape to allow repositioning. Have vascular surgery on standby if an arterial injury is suspected.
- Hold the four target compartments in mind throughout: superficial volar, deep volar, mobile wad and dorsal extensor.
- Begin about 2 cm distal to the antecubital flexion crease on the ulnar side.
- Curve distally in a lazy-S pattern, crossing the volar wrist in a zig-zag (Z-plasty) configuration.
- Extend toward the ring-finger web space if you are releasing the carpal tunnel.
- NEVER cross the wrist crease in a straight line — it causes a severe flexion contracture.
- In the subcutaneous plane preserve the visible veins (basilic, cephalic, median forearm) and identify and protect the medial and lateral antebrachial cutaneous nerves.
A zig-zag crossing of the wrist crease distributes tension across multiple vectors, prevents a straight-line scar contracture across the joint, and allows later closure or grafting. A straight-line incision across the flexion crease causes a severe flexion contracture and makes the wound the hardest on the forearm to close.
- Identify the biceps tendon (central), the brachial artery (medial to it, palpable pulse), the median nerve (1 cm medial to the artery — a yellow cord), and brachioradialis (lateral).
- Divide the lacertus fibrosus — the thick fascial band from the biceps tendon crossing over the brachial artery and median nerve — under direct vision to decompress the proximal neurovascular structures.
The median nerve lies 1 cm medial to the brachial artery in the antecubital fossa as a yellow cord. It dives between the two heads of FDS about 4 cm distal to the elbow crease — its most vulnerable point. Identify it, retract gently, and avoid traction.
- Incise the investing fascia over the superficial flexors longitudinally from elbow to wrist (full-length decompression).
- Release the pronator teres origin from the medial epicondyle if it is tense.
- Contents: pronator teres (radial, proximal), FCR (radial), palmaris longus (central, absent in about 15 percent), FCU (ulnar) and FDS (deep layer — protect the median nerve between its heads).
- Adequacy check: muscle should bulge through the fasciotomy and feel soft on palpation.
- Elevate the FDS and superficial flexor mass radially to expose the deep compartment — FDP on the ulnar side, FPL on the radial side, pronator quadratus distally.
- Incise the fascia over FDP and FPL longitudinally; release the FDP origin from the ulna if it is tense.
- Identify and protect the anterior interosseous nerve on the interosseous membrane throughout — avoid direct manipulation.
The AIN branches from the median nerve 5 to 8 cm distal to the elbow, runs on the anterior surface of the interosseous membrane, and supplies FPL, the radial FDP (index/middle) and pronator quadratus. It is purely motor and critical for pinch; injury loses thumb IP flexion. If transected, repair it immediately; a contused AIN from ischaemia may recover over 8 to 12 weeks.
- Brachioradialis is the most radial and superficial structure; ECRL lies deep to it, ECRB deepest.
- The radial artery runs under brachioradialis in the proximal-to-mid forearm and emerges between BR and FCR at the junction of the middle and distal thirds (palpable pulse distally).
- The superficial radial nerve runs under brachioradialis and emerges about 9 cm proximal to the radial styloid.
- Incise the fascia over the mobile wad. This compartment is unique — it can be released from either side, and many surgeons release it from both volar and dorsal for complete decompression.
- Extend the volar incision into the palm toward the ring-finger web space (an ulnar-midline direction), avoiding the recurrent motor branch which passes radially to the thenar muscles.
- Incise the transverse carpal ligament under direct vision, from the mid-palm (where the median nerve branches) proximally to the arcuate ligament at the wrist, protecting the median nerve and its motor branch deep to the ligament.
- Performed to prevent intrinsic-muscle ischaemia and median neuropathy from hand swelling. Some surgeons do this routinely, others selectively based on hand symptoms and swelling.
The recurrent motor branch of the median nerve passes radially at the distal edge of the transverse carpal ligament and supplies the thenar muscles (APB, opponens, superficial FPB); injury causes thenar weakness and loss of opposition. Directing the carpal tunnel incision toward the ring finger (ulnar-midline) avoids this structure.
- Systematically check the superficial volar, deep volar and mobile wad: each should bulge and be soft on palpation.
- Signs of inadequate release — muscle not bulging, a compartment still firm, or persistent fascial bands — mean you must extend the fascial releases and ensure full proximal-to-distal decompression.
- Pronate the forearm. Make a longitudinal incision from the lateral epicondyle to Lister's tubercle, over the mobile wad and radial border of the extensor compartment. Lister's tubercle is the palpable dorsal-radial landmark at the wrist (EPL grooves around its ulnar side).
- In the subcutaneous plane identify and protect the dorsal sensory branches of the superficial radial nerve, which emerge from under brachioradialis about 9 cm proximal to the radial styloid — injury causes painful dysaesthesia and numbness over the dorsal thumb and hand.
- From the dorsal side, confirm the mobile wad (BR most superficial/radial, ECRL, ECRB deepest) is fully released — it should bulge from both wounds.
- Incise the fascia over the extensor muscles longitudinally from the proximal forearm to the extensor retinaculum at the wrist.
- Release the supinator fascia proximally to decompress the PIN at the arcade of Frohse. Contents: superficial layer (EDC, EDM, ECU) and deep layer (supinator, APL, EPB, EPL, EIP), with the PIN within the supinator and then between the layers.
The PIN — the deep branch of the radial nerve — penetrates the supinator through the arcade of Frohse about 5 cm distal to the lateral epicondyle and supplies all finger and thumb extensors. Release the supinator fascia to decompress the arcade and avoid deep dissection in the proximal dorsal compartment; injury causes complete finger and thumb extension paralysis.
- Verify all four compartments: superficial volar bulging and soft; deep volar bulging when FDS is elevated and soft; mobile wad bulging from both wounds and soft; dorsal extensor bulging and soft.
- Run a finger along each fascial release proximally to distally — there should be continuous decompression with no residual bands. The fasciae are thickest at the wrist, so ensure the distal release is complete. If any compartment is tense, extend the releases.
- Apply the 4 Cs to every compartment: - Colour — pink is viable, pale/dusky is questionable, black/purple/grey is necrotic. - Contractility — gently squeeze or stimulate with forceps; viable muscle contracts. - Consistency — firm is viable, soft/mushy is necrotic. - Capacity to bleed — a cut edge should ooze blood.
- Clearly necrotic muscle: debride to prevent the myonephropathic syndrome. Questionable muscle: leave it and reassess at the second look in 48 hours — forearm muscle loss is devastating, so avoid over-resection. Viable muscle: leave alone.
Necrotic muscle must be debrided to prevent rhabdomyolysis, myoglobinuria, hyperkalaemia and acute renal failure. But forearm muscle loss causes a devastating functional deficit. For questionable muscle, leave it and reassess at the second look rather than over-debride. Document the viability assessment thoroughly.
- Vascular: radial and ulnar pulses, digital capillary refill, Doppler signals if pulses are not palpable. Improved perfusion is expected after decompression; if pulses remain absent, suspect an arterial injury needing vascular exploration.
- Neurological: median (APB, thumb/index/middle sensation), ulnar (interossei/ADM, small/ring sensation), radial (wrist/finger/thumb extension, first web sensation), AIN (pinch) and PIN (finger/thumb extension). Neurology may NOT improve immediately — neurapraxia from ischaemia recovers over 6 to 12 weeks.
- Document a complete neurovascular exam for the medicolegal record and future comparison.
- Achieve haemostasis at the skin edges with judicious cautery. Do NOT cauterise muscle (it causes further necrosis) — use direct pressure for muscle bleeding. Never blind-clamp a vessel (nerve injury risk).
- Irrigate all wounds copiously with saline, removing debris, haematoma and necrotic fragments.
- The critical principle: never close a fasciotomy wound primarily — it causes recurrent compartment syndrome.
- Leave the wounds completely open. Cover with saline-soaked gauze (or dilute 0.25 percent betadine-soaked gauze) and a bulky absorbent outer layer changed daily, or use negative-pressure wound therapy (VAC), which controls oedema, promotes granulation and reduces infection — change every 48 to 72 hours.
- Apply a volar splint holding the wrist neutral with the fingers free for monitoring. Avoid any circumferential dressing or splint. Elevate the arm to heart level (not above, which reduces perfusion).
Primary closure of a fasciotomy wound causes recurrent compartment syndrome and is never performed. Wounds are left completely open with moist dressings or VAC therapy. Definitive closure is planned at the second look (48 to 72 hours) based on resolution of oedema and muscle viability.
- Location
- 1 cm medial to the brachial artery in the antecubital fossa (yellow cord); dives between the FDS heads 4 cm distal to the elbow — its most vulnerable point
- How to protect it
- Identify early, retract gently, make longitudinal releases parallel to the nerve, no cautery nearby
- Location
- Branches from the median nerve 5 to 8 cm distal to the elbow; on the interosseous membrane in the deep volar compartment; supplies FPL/index-middle FDP/PQ
- How to protect it
- Access the deep compartment by elevating FDS radially; identify the AIN on the membrane; avoid direct manipulation
- Location
- Runs under brachioradialis proximally; emerges between BR and FCR at the junction of the middle and distal thirds
- How to protect it
- Palpate the pulse before incision; identify it when releasing the mobile wad; control bleeding with direct pressure, never blind clamp
- Location
- Run between FCU and FDP along the ulnar border; enter Guyon's canal at the wrist
- How to protect it
- Stay midline with the volar incision; identify them before releasing the deep flexors from the ulnar side
- Location
- Deep branch of the radial nerve; penetrates the supinator at the arcade of Frohse about 5 cm distal to the lateral epicondyle; supplies all extensors
- How to protect it
- Release the supinator fascia to decompress the arcade; avoid deep dissection in the proximal dorsal compartment
Aftercare & Complications
Immediate post-operative monitoring. Elevate the arm to heart level. Neurovascular checks every 2 hours for 24 hours, then every 4 hours — monitor radial and ulnar pulses, capillary refill, finger sensation and motion, and pain level, and palpate through the dressing for tension. Increasing pain or a tense forearm despite open wounds signals recurrent compartment syndrome: remove all dressings, re-examine, and return to theatre for revision if a compartment is still tense. Medical management when muscle necrosis is present — prevent the myonephropathic syndrome. Aggressive IV hydration (target urine output 1 to 2 ml/kg/hour), urine alkalinisation with sodium bicarbonate (urine pH greater than 6.5 prevents myoglobin precipitation in the tubules), and close monitoring of CK (often greater than 10,000 to 50,000 U/L), myoglobin, creatinine, potassium (hyperkalaemia) and calcium (hypocalcaemia). Dialysis is needed if acute renal failure develops — mortality is 5 to 10 percent once ARF occurs. Add skin-flora antibiotics (broad-spectrum if contaminated), DVT prophylaxis, and analgesia that does not mask a developing compartment syndrome. Second look at 48 to 72 hours is mandatory for every patient. Reassess muscle viability with the 4 Cs, debride frank necrosis, preserve any questionable muscle that shows viability, send tissue for culture if infection is suspected, and plan definitive wound closure. Radical debridement may require a further second look.
Minimal oedema, wounds approximate easily, healthy muscle. At 3 to 5 days, approximate without tension, with relaxing incisions if needed. Best cosmetic result, lowest morbidity — but rarely achievable due to skin tension.
The commonest outcome. At 5 to 7 days once granulating, harvest 0.010 to 0.012 inch from the thigh, mesh 1.5:1 or 2:1, and bolster for 5 to 7 days. The volar wrist is the hardest area to close and usually needs a graft.
For exposed tendon, nerve or bone needing vascularised cover — local fasciocutaneous, radial forearm (if the radial artery is intact and not needed), or free tissue transfer. Urgent if vital structures are exposed.
Rehabilitation. Phase 1 (weeks 0 to 2): splint wrist neutral, fingers free, wound care. Phase 2 (weeks 2 to 6): active range of motion, gentle stretching, oedema control, scar massage once healed. Phase 3 (weeks 6 to 12): progressive resistance and function. Phase 4 (months 3 to 6): work- and sport-specific activity, aggressive stretching to prevent contracture. Intensive hand therapy is critical — 3 to 6 sessions a week for 6 to 12 months. Expected outcomes. Full recovery in 40 to 60 percent if fasciotomy is performed within 6 hours; partial recovery (some stiffness or weakness) in 30 to 40 percent; poor outcome in 10 to 20 percent if delayed beyond 8 hours (established Volkmann's contracture). Predictors of a poor outcome are delayed fasciotomy, muscle necrosis requiring debridement, concomitant nerve injury, infection, and non-compliance with therapy.
- Recognition
- Progressive finger/wrist flexion contracture over days to weeks; firm fibrotic muscles; unable to passively extend. Graded mild (2 to 3 fingers), moderate (all fingers and wrist), severe (claw hand)
- Prevention
- Early fasciotomy within 6 to 8 hours; complete four-compartment release; debride necrotic muscle; aggressive post-op therapy
- Management
- Mild: stretching, splinting, flexor slide. Moderate: flexor slide, tendon lengthening, capsulotomies. Severe: muscle excision plus free functioning muscle transfer (gracilis), or amputation. Prevention is the only effective treatment
- Recognition
- Median (weak APB/FPL, thumb-index-middle sensory loss), ulnar (weak interossei/ADM, clawing), radial/PIN (wrist/finger drop), AIN (weak pinch, no sensory). Delayed progressive weakness suggests ischaemic neurapraxia
- Prevention
- Identify nerves before fascial incision; gentle retraction; longitudinal incisions parallel to nerves; no cautery near nerves
- Management
- Immediate laceration: microsurgical repair with 8-0/9-0 nylon. Delayed: nerve graft or transfer at 3 to 6 months. Neurapraxia: observe, therapy, EMG at 6 weeks; recovery 8 to 12 weeks. Neurolysis for chronic compression
- Recognition
- Dark tea/cola-coloured urine (myoglobinuria); oliguria/anuria; CK greater than 10,000 to 50,000 U/L; hyperkalaemia, hypocalcaemia, metabolic acidosis; rising creatinine. Develops 24 to 72 hours after muscle injury
- Prevention
- Early fasciotomy; debride necrotic muscle; aggressive IV hydration (UOP 1 to 2 ml/kg/hr); urine alkalinisation (pH greater than 6.5); monitor CK, creatinine, K, Ca
- Management
- ICU; aggressive IV hydration; sodium bicarbonate drip; treat hyperkalaemia (insulin/glucose, calcium gluconate, kayexalate); dialysis if renal failure. Mortality 5 to 10 percent if ARF develops
- Recognition
- Fever, raised WBC, purulent drainage, erythema, warmth, foul odour, worsening pain; positive cultures; can progress to sepsis
- Prevention
- IV antibiotics at incision (1st-gen cephalosporin, or vancomycin if MRSA risk); thorough irrigation; debride all necrotic tissue; frequent dressings or VAC; second look at 48 to 72 hours
- Management
- Cultures (deep wound, tissue, blood); broad-spectrum antibiotics adjusted by culture (e.g. vancomycin plus pip-tazo); surgical debridement if abscess or necrosis, possibly repeated; sepsis protocol if severe
- Recognition
- Persistent pain out of proportion post-fasciotomy; tense forearm; pain on passive finger motion; muscle not bulging; progressive neurovascular deterioration, within 24 hours
- Prevention
- Systematic four-compartment release (elevate FDS to reach the deep volar; release the mobile wad from both sides); confirm each is bulging and soft; extend releases to the wrist where fasciae are thickest
- Management
- Remove all dressings/splints immediately; re-examine; emergent return to theatre for revision fasciotomy; extend incomplete releases and identify any missed compartment; re-confirm all four soft and bulging
- Recognition
- At second look the wounds will not approximate without excess tension, especially the volar wrist across the flexion crease; a skin gap greater than 2 to 3 cm
- Prevention
- Set the expectation early — most need a graft; plan for STSG from the index operation; VAC promotes granulation for grafting
- Management
- Delayed primary closure (3 to 5 days) if minimal tension; STSG (5 to 7 days) most common; flap coverage (urgent if exposed tendon, nerve or bone)
- Recognition
- Progressive loss of motion at wrist, fingers, elbow and forearm rotation over weeks to months; capsular tightness and adhesions; functional deficit; raised DASH score
- Prevention
- Early mobilisation when wounds stable; aggressive hand therapy; night extension splinting; scar massage; adequate pain control to permit therapy
- Management
- Intensive therapy (active/passive ROM, dynamic splinting, serial casting); if a plateau after 6 months of therapy, consider capsulotomy, tenolysis or flexor slide. Some stiffness is permanent in many cases
Viva & Exam Focus
COMPCOMP — the forearm's four spaces
4 Cs4 Cs — muscle viability
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 10-year-old presents 4 hours after a displaced supracondylar humerus fracture. After closed reduction and K-wire fixation, you note increasing forearm swelling and pain. The radial pulse is present. What is your management?”
“Describe the four compartments of the forearm, their contents, and how you access each during fasciotomy.”
“During forearm fasciotomy, you encounter dusky muscle in the deep flexor compartment that has questionable contractility when stimulated. How do you assess muscle viability and what is your management approach?”
Indications
- Clinical compartment syndrome: pain out of proportion (earliest sign); pain on passive finger extension tests the volar compartments (most sensitive); pain on passive flexion tests the dorsal compartment; a tense rock-hard forearm; paraesthesiae in the median/ulnar distribution
- Pressure thresholds if the diagnosis is uncertain: absolute greater than 30 mmHg, or delta (diastolic minus compartment) less than 30 mmHg. In children some use greater than 20 mmHg or a delta less than 40 mmHg. The clinical picture always takes precedence
- High-risk injuries: supracondylar humerus fractures (leading paediatric cause; incidence under 1 percent but rising sharply with vascular injury, a pink pulseless hand or an AIN deficit), both-bone forearm fractures, crush injuries, reperfusion after arterial repair (ischaemia over 4 to 6 hours)
- Pulses can be PRESENT — the forearm has extensive collateral circulation. Never wait for pulselessness
Key anatomy
- FOUR compartments: superficial volar (PT, FCR, PL, FCU, FDS with the median nerve between the FDS heads 4 cm from the elbow); deep volar (FDP, FPL, PQ with the AIN on the membrane); mobile wad (BR, ECRL, ECRB with the radial artery under BR and the superficial radial nerve); dorsal (all extensors with the PIN entering the supinator at the arcade of Frohse 5 cm from the lateral epicondyle)
- Median nerve: 1 cm medial to the brachial artery in the antecubital fossa; dives between the FDS heads 4 cm distal to the elbow (most vulnerable point)
- AIN: branches from the median nerve 5 to 8 cm distal to the elbow, on the interosseous membrane; supplies FPL, index/middle FDP and PQ. Access by elevating FDS radially
- Radial artery: under brachioradialis proximally, emerges between BR and FCR at the middle/distal junction. Superficial radial nerve emerges from under BR 9 cm proximal to the radial styloid
Critical steps
- VOLAR approach: curvilinear incision on the ulnar side of the antecubital fossa, crossing the wrist in a ZIG-ZAG (Z-plasty) — NEVER a straight line. Extend into the carpal tunnel for prophylactic release
- Divide the lacertus fibrosus. Release the superficial volar (protect the median nerve between the FDS heads). Elevate FDS radially and release the deep volar (protect the AIN). Release the mobile wad from the volar side
- DORSAL approach: pronate; longitudinal incision from the lateral epicondyle to Lister's tubercle; protect the superficial radial nerve branches (9 cm proximal to the styloid). Release the mobile wad dorsally and the extensor compartment including the supinator fascia (decompress the PIN at the arcade)
- CONFIRM: all four compartments bulge and are soft. Never close primarily. Apply a VAC or moist dressings. Second look at 48 to 72 hours is mandatory
Danger zones
- Median nerve between the FDS heads (4 cm distal to the elbow) — most vulnerable point in the volar forearm
- AIN on the interosseous membrane — critical for pinch; protect when releasing the deep volar by elevating FDS
- Radial artery under brachioradialis — direct pressure for bleeding, never a blind clamp
- Ulnar nerve and artery at the ulnar border between FCU and FDP — vulnerable during ulnar-sided and deep-compartment dissection
- PIN in the supinator (5 cm from the lateral epicondyle) — release the supinator fascia to decompress the arcade of Frohse
- Superficial radial nerve dorsal branches (9 cm proximal to the radial styloid) — injury causes painful dysaesthesia
- Recurrent motor branch of the median nerve at the distal TCL — direct the carpal tunnel incision toward the ring finger (ulnar-midline)
- Volar wrist skin across the flexion crease — a zig-zag incision is mandatory; a straight line causes a severe flexion contracture
Technique pearls
- Pain on passive finger extension is the most sensitive test for volar compartment syndrome; flexion tests the dorsal compartment. The clinical diagnosis is paramount — do not delay for pressures in clear cases
- A zig-zag volar incision crossing the wrist is MANDATORY — a straight line across the flexion crease causes a severe contracture. Plan for a likely STSG
- The mobile wad can be released from the volar OR dorsal approach — many surgeons release from both for complete decompression
- The deep volar compartment is accessed by elevating FDS radially — it is a separate compartment requiring a distinct release and is commonly missed
- The 4 Cs of muscle viability; preserve questionable muscle for the second look rather than over-debride
- NEVER close primarily — 60 to 80 percent need an STSG. Second look at 48 to 72 hours is mandatory. The volar wrist is the hardest area to close
Complications
- Volkmann's ischaemic contracture (5 to 30 percent if delayed beyond 8 hours): irreversible flexion deformity from muscle fibrosis. Graded mild (2 to 3 fingers), moderate (all fingers and wrist), severe (claw hand). Prevention is the only effective treatment
- Nerve injuries (5 to 15 percent): median (between the FDS heads, commonest), AIN (loss of pinch), ulnar (clawing), radial/PIN (drop), superficial radial (dysaesthesia). Laceration: immediate microsurgical repair; neurapraxia: observe, recovery 8 to 12 weeks
- Myonephropathic syndrome (10 to 30 percent if severe): rhabdomyolysis to myoglobinuria (tea-coloured urine) to hyperkalaemia to renal failure. Prevent with early fasciotomy, debridement, aggressive IV hydration and urine alkalinisation (pH greater than 6.5). Mortality 5 to 10 percent if ARF develops
- Incomplete release (10 to 20 percent): persistent pain and a tense compartment; the deep volar or mobile wad is commonly missed. Emergent return to theatre for revision
- Infection (15 to 25 percent): IV antibiotics, irrigation, debridement, VAC or frequent dressings
- Wound closure (60 to 80 percent need STSG): the volar wrist is the hardest; flap if exposed structures
- Chronic stiffness (40 to 60 percent): aggressive therapy for 6 to 12 months; capsulotomy or tenolysis after a 6-month plateau
Post-op protocol
- Immediate: elevate; neurovascular checks 2-hourly for 24 hours then 4-hourly. If muscle necrosis: aggressive IV hydration (UOP 1 to 2 ml/kg/hr), alkalinise the urine, monitor CK/creatinine/K/myoglobin
- Dressings: VAC every 48 to 72 hours or moist dressings daily; never circumferential. Splint the wrist neutral, fingers free
- Second look 48 to 72 hours (mandatory): reassess the 4 Cs, debride frank necrosis, plan closure (delayed primary 3 to 5 days; STSG 5 to 7 days; flap if exposed structures)
- Rehabilitation: protection (0 to 2 weeks), early mobilisation (2 to 6 weeks), strengthening (6 to 12 weeks), advanced rehab (3 to 6 months). Intensive therapy is critical — 3 to 6 sessions a week for 6 to 12 months
- Outcomes: full recovery 40 to 60 percent if fasciotomy under 6 hours; partial recovery 30 to 40 percent; poor outcome 10 to 20 percent if delayed beyond 8 hours
Exam tips
- HIGHEST YIELD: supracondylar fractures are the leading paediatric cause; the radial pulse can be PRESENT with compartment syndrome; pain on passive finger extension is the most sensitive test; a zig-zag volar incision is mandatory
- Four compartments (COMP): Central volar, On the bone, Mobile wad, Posterior
- The 4 Cs of viability; preserve questionable muscle; debride frank necrosis to prevent the myonephropathic syndrome
- NEVER close primarily; 60 to 80 percent need an STSG; second look at 48 to 72 hours; the volar wrist is hardest to close
- Preventing Volkmann's contracture is the only effective treatment — decompress within 6 to 8 hours. Delay beyond 8 hours risks an irreversible flexion contracture
Background & Evidence
Epidemiology. Forearm compartment syndrome is most often fracture-driven and male-predominant. In the largest dedicated forearm series (Duckworth, 2012), a fracture of the radius and/or ulna was the cause in 69 percent and isolated soft-tissue injury in 31 percent, with a marked male predominance (82 of 90 patients) and a mean age of 33. The median time from injury to fasciotomy was 12 hours, and a delay of more than 6 hours significantly increased complications. In children, forearm and supracondylar fractures are the dominant triggers (Grottkau, 2005 — 85 percent of 133 paediatric cases were fracture-related, and open fractures significantly raised the risk); a substantial proportion declare only after admission, mandating structured serial monitoring of the at-risk paediatric limb. The four-compartment anatomy is the operative map. The full reference anatomy:
- Contents
- Pronator teres, FCR, palmaris longus (absent in about 15 percent), FCU, FDS
- Key structure at risk
- Median nerve — passes between the two heads of FDS about 4 cm distal to the elbow (its most vulnerable point)
- How it is accessed
- Volar curvilinear incision; longitudinal fasciotomy elbow to wrist
- Contents
- FDP (ulnar), FPL (radial), pronator quadratus (distal)
- Key structure at risk
- Anterior interosseous nerve — on the interosseous membrane; supplies FPL, radial FDP and PQ (purely motor)
- How it is accessed
- Elevate the FDS and superficial flexor mass radially to expose it
- Contents
- Brachioradialis (most superficial/radial), ECRL, ECRB (deepest)
- Key structure at risk
- Radial artery — under brachioradialis, emerging between BR and FCR at the middle/distal junction; superficial radial nerve emerges 9 cm proximal to the radial styloid
- How it is accessed
- Can be released from the volar OR dorsal approach — often both
- Contents
- Superficial: EDC, EDM, ECU. Deep: supinator, APL, EPB, EPL, EIP
- Key structure at risk
- Posterior interosseous nerve — penetrates the supinator at the arcade of Frohse about 5 cm distal to the lateral epicondyle; supplies all extensors
- How it is accessed
- Dorsal longitudinal incision from lateral epicondyle to Lister's tubercle; release the supinator fascia to decompress the PIN
Volkmann's ischaemic contracture — classification (Tsuge/Seddon). The late consequence of delayed or missed decompression: irreversible flexion contracture from muscle fibrosis after prolonged ischaemia. Mild — flexion contracture of 2 to 3 fingers (usually middle/ring), wrist flexion and intrinsics preserved. Moderate — all fingers flexed, wrist flexed, some intrinsic weakness and a sensory deficit. Severe — all muscle groups (flexors, extensors, intrinsics) fibrotic, a severe contracture with claw hand and sensory loss. Prevention — early fasciotomy within 6 to 8 hours — is the only effective treatment; outcome is poor once a contracture is established. Key evidence. Decompression within 6 hours minimises complications (Duckworth, 2012). When clinical assessment is unreliable, continuous differential (delta) pressure monitoring is highly accurate — McQueen (2013) reported estimated sensitivity 94 percent and specificity 98 percent, with only 5 false negatives and 6 false positives — but it supplements, never replaces, a clinical diagnosis. The delta-pressure rule itself was established by McQueen and Court-Brown (1996): an absolute pressure threshold (30 or 40 mmHg) would have led to many unnecessary fasciotomies, whereas a delta pressure (diastolic minus compartment) of less than 30 mmHg produced no missed cases. Ulmer (2002) showed that no single clinical sign is sensitive (13 to 19 percent) but that their absence is reassuring, and the probability of compartment syndrome rises to about 93 percent when three or more findings are present — so serial examination drives the diagnosis.
References
Acute compartment syndrome of the forearm
- Largest dedicated forearm series: 90 patients over 22 years, mean age 33, marked male predominance (82 of 90)
- A fracture of the radius and/or ulna was the cause in 62 patients (69%); isolated soft-tissue injury caused 28 (31%)
- Median time from injury to fasciotomy was 12 hours (range 2 to 72 hours)
- Delay to fasciotomy of more than 6 hours significantly increased complications (p=0.018); complications occurred in roughly a third of patients
- Younger age and crush injury were independent risk factors for needing split-thickness skin grafting for wound closure
The estimated sensitivity and specificity of compartment pressure monitoring for acute compartment syndrome
- 850 monitored patients with tibial diaphyseal fracture; 152 (17.9%) underwent fasciotomy
- Continuous differential (delta) pressure monitoring had estimated sensitivity 94% and specificity 98%
- Estimated positive predictive value 93% and negative predictive value 99%
- Only 5 false negatives and 6 false positives, supporting the delta-pressure threshold as a robust decision aid
Compartment monitoring in tibial fractures: the pressure threshold for decompression
- Prospective study of 116 tibial diaphyseal fractures with 24-hour continuous anterior compartment monitoring
- Using absolute pressure thresholds (30 or 40 mmHg) would have led to many unnecessary fasciotomies (43% and 23% respectively)
- A differential pressure (diastolic minus compartment pressure) of less than 30 mmHg as the threshold produced no missed cases of acute compartment syndrome
- Established the delta pressure less than 30 mmHg rule now used across all limb compartments
The clinical diagnosis of compartment syndrome of the lower leg: are clinical findings predictive of the disorder?
- Systematic review of clinical signs for compartment syndrome diagnosis
- Sensitivity of individual clinical findings was low (13% to 19%); specificity and negative predictive value were high (97% to 98%)
- Probability of compartment syndrome rose to about 93% when 3 or more clinical findings were present
- Clinical findings are most useful by their ABSENCE to exclude the diagnosis
Compartment syndrome in children and adolescents
- 133 paediatric cases from the National Pediatric Trauma Registry; boys outnumbered girls 4 to 1, median age 12 years
- 85% of cases were sequelae of fractures; forearm fractures were the most common upper-extremity cause
- Open fractures significantly increased the risk for both forearm and leg compartment syndrome
- 60% went directly from emergency room to theatre, implying the remainder developed compartment syndrome after admission or were diagnosed late
Acute compartment syndromes: diagnosis and treatment with the aid of the wick catheter
- Classic description of the compartment pressure measurement technique using the wick catheter
- Established the concept of measuring intracompartmental pressure to support the diagnosis
- Foundational work underpinning later absolute and delta pressure thresholds for decompression
Acute compartment syndrome of the forearm
- Detailed anatomic description of the four forearm compartments
- Surgical technique for both volar and dorsal forearm fasciotomy
- Review of complications including Volkmann's ischaemic contracture
Acute compartment syndrome: who is at risk?
- Identified the patient and injury factors that raise the risk of acute compartment syndrome
- Reinforced the pressure thresholds: absolute greater than 30 mmHg or delta pressure less than 30 mmHg
- Emphasised that the clinical diagnosis is paramount over isolated measurements
Diagnosis and management of extremity compartment syndromes: an orthopaedic perspective
- Comprehensive review of compartment syndrome diagnosis and management including fasciotomy techniques
- Covers the principles of complete compartment release and wound management
- Discusses the recognition and prevention of complications such as Volkmann's contracture
Diagnostic techniques in acute compartment syndrome of the leg
- Review of diagnostic techniques including clinical examination, pressure measurement, and newer modalities
- Discusses the role and limitations of each diagnostic method
- Supports the primacy of clinical diagnosis supplemented by pressure measurement when needed
Ultrasound-guided release of forearm compartment syndrome
- Describes the four forearm compartments and their release techniques
- Emphasises the importance of complete decompression of all compartments
- Explores ultrasound as an adjunct to guide fasciotomy
Acute pediatric upper extremity compartment syndrome in the absence of fracture
- Paediatric-specific considerations of upper-extremity compartment syndrome
- Demonstrates that compartment syndrome can occur in children without a fracture
- Discusses lower diagnostic thresholds used in some paediatric studies
The treatment of unreduced supracondylar humerus fractures with vascular compromise in children
- Management of supracondylar fractures with vascular injury and compartment syndrome risk
- Addresses the pink pulseless hand and the threshold for exploration and fasciotomy
- Links vascular compromise to the heightened risk of forearm compartment syndrome