Dorsal wrist ganglion · scapholunate origin · stalk-plus-capsule excision
- A dorsal wrist ganglion arises from the scapholunate (SL) ligament in 60-70 percent of cases — complete excision of the stalk to its origin at the SL interval is the operation-defining step.
- The ganglion lies between the 3rd extensor compartment (EPL at Lister's tubercle) and the 4th compartment (EDC); the retinaculum is opened longitudinally between them.
- The superficial radial nerve is the structure most at risk — injury occurs in 5-10 percent and causes a painful neuroma. Identify and protect its branches before any deep dissection.
- Complete stalk excision with a 5mm cuff of dorsal capsule drops recurrence from about 59 percent (aspiration) to about 21 percent (open) or 6 percent (arthroscopic) — Level I meta-analysis (Head 2015).
When & Why
Indication. A symptomatic dorsal wrist ganglion that has failed conservative management — pain limiting daily activities or work, limitation of wrist range of motion, functional impairment (weakness, catching, an instability sensation), or a significant cosmetic concern — particularly recurrence after aspiration. Surgery is also justified for diagnostic uncertainty (an atypical presentation needing histology, a solid component on imaging, or concern for occult tumour). Relative indications include patient preference for definitive treatment after multiple aspirations, and a large ganglion (greater than 2cm) where aspiration has a high failure rate. Contraindications. Absolute: active infection over the surgical site, or severe comorbidity precluding surgery. Relative: an asymptomatic ganglion (observation is preferred), a first presentation without a trial of aspiration, poor skin quality or heavy previous scarring, a bleeding diathesis or anticoagulation needing optimisation, and a keloid tendency or connective tissue disorder. The one decision that matters. Surgery is not the only option, and the ganglion that has not been given a fair trial of non-operative care should not yet be operated on. When surgery is indicated, every technique begins with the same principle — complete excision of the stalk at its scapholunate origin with a cuff of dorsal capsule:
Simple office procedure, but about 59 percent recurrence (Head 2015). A reasonable first-line trial for symptomatic relief in a patient who does not want surgery.
The standard operation — stalk plus capsular cuff excision through a small dorsal incision; about 21 percent recurrence. The evidence-based default when surgery is indicated.
Resects the stalk from inside the joint; about 6 percent recurrence and faster return to work, but unproven superiority over open excision and needs arthroscopy skills.
Consent specifically for superficial radial nerve injury or a painful neuroma (5-10 percent), wrist stiffness (10-20 percent, usually temporary), scar problems (5-10 percent), and recurrence (about 21 percent after open excision). Reassure the patient that the capsular defect is not repaired and scars naturally, and that the cosmetic outcome is best with a transverse incision in the skin creases. Setup. Supine, arm on a hand table, wrist pronated, upper-arm tourniquet inflated to 250-275 mmHg after exsanguination. Loupe magnification (2.5-3.5x) is mandatory — nerve and stalk identification is the whole game.
The Operation
The goal is to expose the ganglion through a small dorsal incision, identify and protect the superficial radial nerve, open the extensor retinaculum between the 3rd and 4th compartments, trace the stalk down to its scapholunate origin, and excise it with a cuff of dorsal capsule while preserving the SL ligament itself. The exposure is laid out in full as the first steps below — it is the heart of the operation.
Operative sequence
- Supine, arm on a hand table, wrist pronated; upper-arm tourniquet.
- Mark the ganglion BEFORE exsanguination — it flattens and becomes hard to find once the tourniquet is inflated.
- Mark the expected course of the superficial radial nerve dorsoradially, and mark Lister's tubercle (the landmark for the 3rd compartment and EPL).
- Confirm transillumination to verify the cystic nature of the mass; apply the tourniquet and exsanguinate with elevation or an Esmarch bandage.
- Transverse incision (author's preference): 2-3cm over the ganglion, following Langer's lines and the natural skin creases for the best cosmetic result. It crosses superficial radial nerve branches, so careful identification is essential, and it is harder to extend.
- Longitudinal incision: 3-4cm along the radial border of the 4th compartment, placed slightly ulnar to avoid the nerve. Easier nerve protection and deeper dissection, and easier to extend for revision — but a more visible scar.
- Incise skin sharply with a #15 blade and handle the skin edges with fine-toothed forceps to minimise trauma.
- Immediately on entering the subcutaneous fat, identify the superficial radial nerve branches — typically 3-5 branches that fan across the dorsal wrist, dorsoradial to the incision, emerging from under brachioradialis about 7-9cm proximal to the radial styloid.
- Use blunt dissection with fine scissors to expose and trace each branch proximally and distally, then place vessel loops around them for protection throughout the procedure.
- Use bipolar cautery only, kept well away from nerve; excessive traction causes neuropraxia. This is the step that prevents the most common and most troublesome complication.
- Develop the subcutaneous plane down to the extensor retinaculum overlying the ganglion.
- Palpate and identify Lister's tubercle (the bony prominence on the dorsal distal radius).
- Identify the EPL tendon running ulnar to Lister's tubercle in the 3rd compartment, and the EDC tendons ulnar to it in the 4th compartment. The ganglion lies between these two compartments, emerging from the scapholunate joint deep to the retinaculum.
- Open the extensor retinaculum longitudinally between the 3rd (EPL) and 4th (EDC) compartments — this is the interval through which the ganglion stalk passes from deep (SL joint) to superficial (ganglion).
- Protect EPL radially and EDC ulnarly during the opening. The stalk often becomes visible passing through this interval.
- Identify EPL before opening the retinaculum and maintain awareness throughout — EPL laceration is rare but devastating.
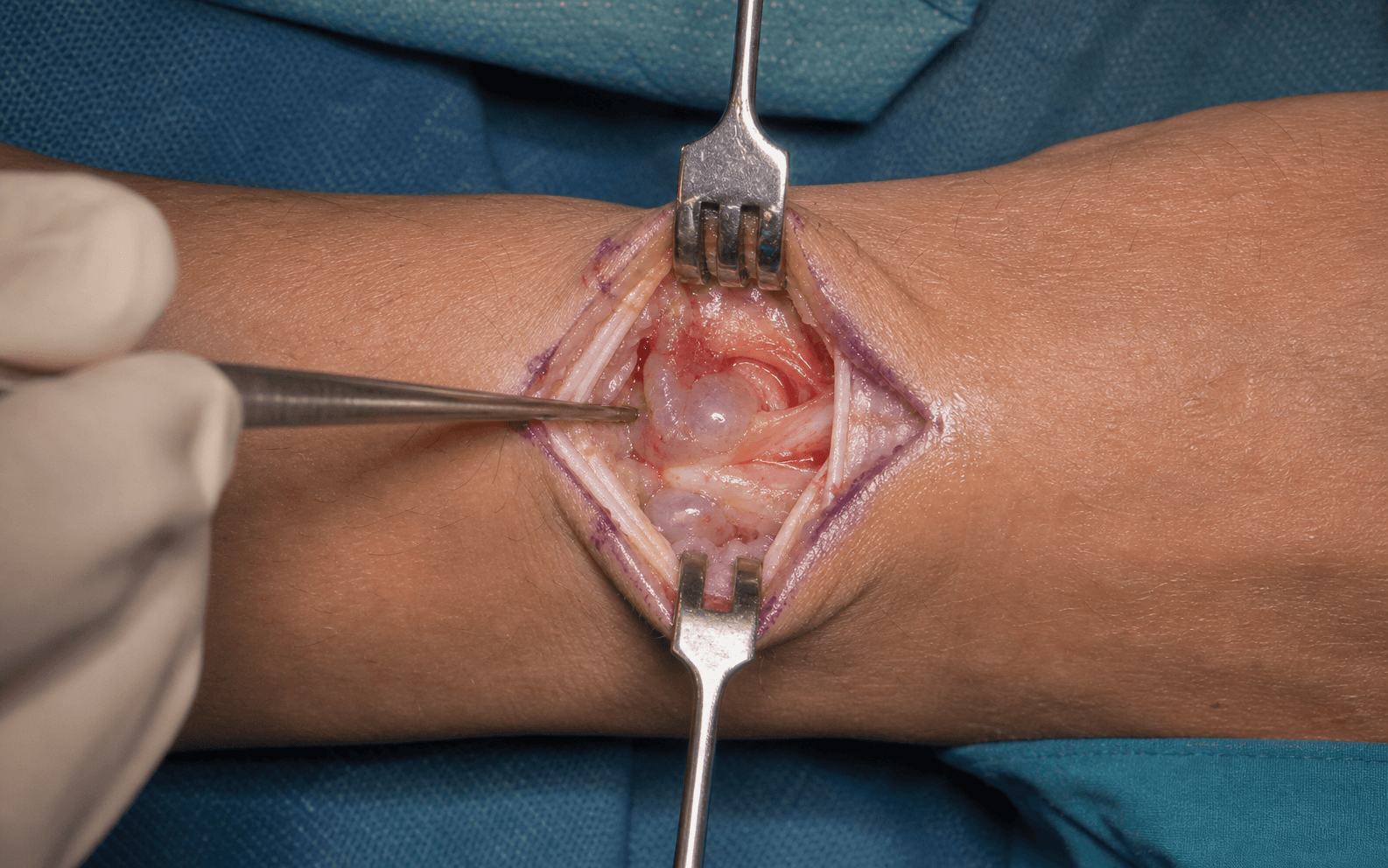
- Mobilise the ganglion circumferentially using sharp and blunt dissection. The ganglion has a thick fibrous wall but no true capsule.
- Dissect it off the adherent tendons (EPL, EDC, ECRB, ECRL) with predominantly blunt technique; avoid grasping the ganglion directly with instruments, as rupture makes stalk identification harder (rupture is acceptable if it occurs — the stalk is what matters).
- Ligate or cauterise small feeding vessels away from the protected nerves.
- Identify the narrowed stalk at the base of the ganglion and follow it deep, between EPL and EDC, toward the wrist joint.
- The stalk passes through the retinaculum and inserts on the dorsal wrist capsule at the scapholunate (SL) interval. Gentle traction on the ganglion demonstrates the direction of the stalk; palpate the wrist joint line as a guide to depth.
- Use loupe magnification. If the stalk is unclear or appears to have multiple small attachments rather than one discrete stalk, trace every attachment down to the dorsal capsule and consider a small capsulotomy to visualise the connections from inside the joint.
- Excise the stalk at its origin from the dorsal wrist capsule, taking a 5mm cuff of capsule around the base — down to the level of the SL ligament and articular cartilage.
- Preserve the integrity of the SL ligament itself — excise capsule only, never ligament substance, or you will create a DISI-pattern carpal instability.
- The specimen is the ganglion plus the stalk plus the capsular cuff, removed en bloc. An inadequate capsulectomy (less than 5mm) is the main cause of recurrence.
- Send all excised tissue for histopathology to confirm a ganglion (thick fibrous wall, no epithelial lining, mucinous contents) and exclude occult pathology.
- Inspect the defect: confirm the SL ligament is intact, the stalk base is completely excised, and no cyst fragments remain. A capsular defect of 1-2cm is acceptable and expected, and is not repaired.
- Deflate the tourniquet and achieve meticulous haemostasis with bipolar cautery for small vessels and ties for larger ones — avoid cautery near the nerve branches, using ties or clips instead. Irrigate the wound.
- Repair the extensor retinaculum with interrupted 4-0 or 5-0 absorbable sutures to restore anatomy and prevent extensor bowstringing; ensure the EPL sits in its groove at Lister's tubercle. Leaving a small defect to reduce adhesions is an acceptable alternative.
- Close the subcutaneous tissue with 5-0 absorbable suture to minimise dead space, and the skin with 5-0 nylon interrupted sutures or a subcuticular 5-0 Monocryl plus Steri-Strips.
- Apply a soft gauze and crepe dressing with the wrist in neutral. No rigid splint is needed unless the patient prefers one for comfort.
Before any deep dissection, identify the superficial radial nerve branches in the subcutaneous fat dorsoradial to the incision. There are typically 3-5 branches fanning across the dorsal wrist, only 2-3mm deep, and injury (in 5-10 percent of cases) causes numbness or a painful neuroma — the most common and most troublesome complication. Protect every branch with vessel loops, use blunt dissection, keep bipolar cautery well away, and never dissect blindly. If a branch is transected, a larger one (greater than 1mm) is repaired primarily with 8-0 or 9-0 nylon under magnification and the injury documented and discussed with the patient.
The single most important technical point is complete excision of the stalk at its origin from the scapholunate ligament, with a 5mm cuff of dorsal capsule. This is the key difference between surgical excision (open about 21 percent, arthroscopic about 6 percent recurrence) and aspiration (about 59 percent recurrence). Trace the stalk to the SL interval, excise a 5mm capsular margin, and protect the SL ligament substance to prevent carpal instability.
The stalk arises from the dorsal SL ligament, but the ligament substance must be preserved — excise only the capsular cuff. An over-aggressive capsulectomy that breaches the SL ligament causes a DISI-pattern carpal instability (scapholunate gapping greater than 3mm, scapholunate angle greater than 70 degrees). Equally, do not repair the capsular defect: it scars naturally, and repairing it risks stiffness.
Aftercare & Complications
Rehabilitation | Phase | Timing | Activity & immobilisation | |-------|--------|---------------------------| | 1 | 0-2 weeks | Soft dressing, no routine splint; elevate for 48 hours; finger range of motion immediately and wrist range of motion from day 2-7; sutures out at 10-14 days | | 2 | 2-4 weeks | Light activities of daily living; driving when comfortable (usually 2-3 weeks); begin scar massage | | 3 | 4-6 weeks | Full wrist range of motion; light strengthening; return to light work and sport | | 4 | 6-12 weeks | Return to heavy work and sport; continue scar management for 3-6 months | No formal hand therapy is needed for uncomplicated cases — refer only for significant stiffness at 6 weeks, nerve symptoms, or CRPS concerns. Recurrence, when it occurs, usually appears at 6-12 months. Complications
- Recognition
- Palpable mass at the original site, usually 6-12 months; may be asymptomatic; confirm with ultrasound or MRI if uncertain
- Prevention
- Complete stalk excision to the SL origin with a 5mm capsular cuff; remove all cyst wall; send for histology
- Management
- Observe if asymptomatic; aspiration if symptomatic; revision excision if recurrent after aspiration — warn of higher nerve-injury risk from scarring
- Recognition
- Numbness or painful neuroma over the dorsal thumb, index and middle finger; positive Tinel; usually apparent immediately
- Prevention
- Identify all branches early under loupe magnification; vessel-loop retraction; no cautery near nerves; blunt dissection
- Management
- Neuropraxia settles over 6-12 weeks; a transected larger branch is repaired primarily with 8-0 or 9-0 nylon; persistent neuroma — desensitisation, gabapentin, excision with burial or grafting
- Recognition
- Reduced flexion/extension or radial/ulnar deviation at 2-6 weeks; check for CRPS signs (pain, swelling, colour change)
- Prevention
- Early range of motion day 2-7; avoid rigid splinting; gentle technique; meticulous haemostasis
- Management
- Hand therapy with range-of-motion exercises and stretching; NSAIDs; most resolve by 3 months; manipulation under anaesthesia rarely for persistent stiffness beyond 6 months
- Recognition
- Raised, red or painful scar; keloid extending beyond the wound
- Prevention
- Transverse incision in Langer's lines; tension-free fine-suture closure; early massage and silicone
- Management
- Silicone gel, pressure therapy, scar massage, intralesional steroid; revision if functionally limiting
- Recognition
- Loss of thumb IP extension; lag on testing; usually recognised intra-operatively
- Prevention
- Identify EPL at Lister's tubercle before opening the retinaculum; maintain awareness throughout; blunt dissection at the ganglion-tendon interface
- Management
- Partial tear (less than 50 percent): epitenon repair; complete tear: primary repair with a 4-0 braided core and 6-0 epitendinous suture, splint 6 weeks; delayed diagnosis: EIP to EPL transfer
- Recognition
- Visible tear, scapholunate gapping greater than 3mm and an scapholunate angle greater than 70 degrees; later DISI pattern on radiograph
- Prevention
- Excise only a 5mm capsular cuff; visualise the SL ligament first; sharp dissection at the capsule-ligament junction
- Management
- Small capsular injury: observe; significant tear: primary repair with a suture anchor or transosseous sutures plus K-wire stabilisation for 6-8 weeks; chronic instability: reconstruction or fusion
- Recognition
- Wound erythema, warmth or discharge, usually at 3-10 days
- Prevention
- Single-dose prophylaxis (cephazolin); sterile technique; meticulous haemostasis; tension-free closure
- Management
- Superficial: oral flucloxacillin or cephalexin; deep: wound washout, IV antibiotics, culture-directed therapy
Viva & Exam Focus
S.T.A.L.K.S.T.A.L.K. — critical steps for complete excision
E.P.L.E.P.L. — protecting the most important tendon
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old secretary presents with a 2cm dorsal wrist ganglion causing pain with typing. She had aspiration 6 months ago with recurrence. She requests surgical excision. Walk me through your consent discussion and surgical planning.”
“You are performing ganglion excision and have mobilized the ganglion, but you cannot clearly identify the stalk — it appears to have multiple small attachments rather than one clear stalk. How do you proceed?”
“Post-operatively at 6 weeks your patient has good wound healing and no recurrence, but significant wrist stiffness with 50% loss of flexion/extension compared to the other side, and pain with movement. They are frustrated, as you told them early mobilization would prevent this. How do you manage this patient?”
Indications
- Symptomatic ganglion (pain, ROM or functional limitation) that has failed aspiration
- Diagnostic uncertainty needing histology; recurrence after multiple aspirations
- Contraindications: asymptomatic (observe), untried aspiration, active infection
Key anatomy
- Arises from the SCAPHOLUNATE ligament in 60-70% — the dorsal portion at the SL interval
- Lies between the 3rd compartment (EPL, Lister's tubercle) and the 4th compartment (EDC)
- Superficial radial nerve: 3-5 branches fan across the dorsal wrist subcutaneously — MOST AT RISK
- The dorsal SL ligament is the thickest portion (3mm) and the primary restraint — preserve it
Critical steps
- Mark the ganglion BEFORE exsanguination (it flattens with the tourniquet); mark the SRN course and Lister's tubercle
- Transverse incision (cosmesis) OR longitudinal along the 4th compartment (easier dissection)
- IDENTIFY the superficial radial nerve branches immediately and protect them with vessel loops
- Open the retinaculum longitudinally between EPL (3rd) and EDC (4th); mobilise the ganglion off the tendons
- CRITICAL: trace the stalk to the SL origin, excise with a 5mm capsular cuff, PRESERVE the SL ligament
- Deflate the tourniquet, haemostasis (no cautery near nerves), repair the retinaculum, close skin
Danger zones
- Superficial radial nerve (dorsoradial, subcutaneous) — 5-10% injury rate, painful neuroma
- EPL tendon (3rd compartment) — laceration is devastating, needs a transfer
- EDC tendons (4th compartment) — injury weakens finger extension
- Scapholunate ligament (stalk origin) — injury causes DISI-pattern carpal instability
- ECRB/ECRL (2nd compartment) — may be adherent to large ganglia
Technique pearls
- STALK EXCISION is the key difference: open about 21% / arthroscopic about 6% recurrence vs aspiration about 59% (Head 2015)
- Loupe magnification (2.5-3.5x) for nerve protection and stalk identification
- Gentle traction on the ganglion shows the stalk direction when it is hard to see
- Excise a 5mm capsular cuff — an inadequate margin causes recurrence
- Do NOT repair the capsular defect — it scars naturally; repair risks stiffness
- A small capsulotomy to visualise from inside the joint is acceptable if the stalk is unclear
Complications
- MOST COMMON: superficial radial nerve injury (5-10%) — numbness or neuroma; prevent by early identification and protection
- Recurrence (open about 21%, arthroscopic about 6%, aspiration about 59%) — from incomplete stalk excision
- Wrist stiffness (10-20%, usually temporary) — early ROM day 2-7, avoid rigid splinting
- Scar problems (5-10%) — massage, silicone, intralesional steroid
- EPL laceration (less than 1%, devastating) and SL ligament injury (less than 1%) — rare but serious
Post-op protocol
- Elevate for 48h; finger ROM immediately; wrist ROM from day 2-7; soft dressing, no routine splint
- Sutures out at 10-14 days; scar massage from 2 weeks
- Return to desk work 2-3 weeks; full activities 4-6 weeks
- Send ALL tissue for histology: thick fibrous wall, NO epithelial lining, mucinous contents
Exam tips
- EMPHASISE stalk excision — the critical technical point and the difference from aspiration
- ALWAYS name the superficial radial nerve as the structure most at risk
- Quote the anatomy: SL origin (60-70%), between the 3rd (EPL) and 4th (EDC) compartments
- If asked about the capsule: do NOT repair the defect — it scars, and repair increases stiffness
- MNEMONIC S.T.A.L.K. — Superficial nerve, Third/fourth compartments, Access retinaculum, Locate stalk, Keep capsular cuff
Background & Evidence
Epidemiology. Ganglion cysts are the commonest soft-tissue mass of the hand and wrist, with a female predominance and a peak in the second to fourth decades; the dorsal wrist is the most frequent site. Roughly half resolve spontaneously, which underpins observation as first-line management for the asymptomatic cyst (Gude 2008). Pathoanatomy. Two theories coexist. The classical mucin-coalescence theory holds that extra-articular mucin droplets coalesce and the cyst wall and pedicle form later. The valve-like duct theory (Angelides 1976) describes a one-way duct between the joint and the cyst: synovial fluid is pumped into the cyst but cannot return, which is why a ganglion refills after aspiration and why excising the cyst alone (leaving the stalk) recurs. The dorsal wrist ganglion originates from the scapholunate ligament in 60-70 percent of cases; attachments may also arise elsewhere over the dorsal capsule, especially near the capitate (Clay 1988). Surgical anatomy — the dorsal extensor compartments. Lister's tubercle is the key landmark: the 3rd compartment (EPL) lies just ulnar to it, and the 4th compartment (EDC) lies ulnar to that. The ganglion and its stalk pass between the two.
- Contents
- APL, EPB
- Relevance to the ganglion
- Radial border; rarely involved
- Contents
- ECRL, ECRB
- Relevance to the ganglion
- Over the radial styloid; may adhere to large ganglia
- Contents
- EPL
- Relevance to the ganglion
- Ulnar to Lister's tubercle — KEY LANDMARK, radial side of the ganglion
- Contents
- EDC, EIP
- Relevance to the ganglion
- Central — GANGLION LOCATION, ulnar side of the ganglion
- Contents
- EDM
- Relevance to the ganglion
- Ulnar side; not involved
- Contents
- ECU
- Relevance to the ganglion
- Ulnar border, in the groove of the ulnar head
The scapholunate ligament. Its dorsal portion is the thickest (3mm) and the primary restraint to scaphoid flexion; the ganglion stalk arises from it, but the ligament substance must be preserved to avoid a DISI-pattern instability. The superficial radial nerve emerges from under brachioradialis about 7-9cm proximal to the radial styloid and fans into 3-5 dorsal sensory branches across the wrist — the structure most at risk. The posterior interosseous nerve lies deep to the 4th compartment and the radial artery is volar to the SL joint, protected by the dorsal approach. Treatment evidence. Head's Level I meta-analysis (2015) pooled 35 studies and 2,239 ganglia and remains the benchmark for counselling patients on recurrence and complications by modality.
- Recurrence
- About 59%
- Complication rate
- About 3%
- Comment
- Office procedure; a reasonable first-line trial
- Recurrence
- About 21%
- Complication rate
- About 14%
- Comment
- Stalk plus capsular cuff excision — the standard operation
- Recurrence
- About 6%
- Complication rate
- About 4%
- Comment
- Resects the stalk from inside the joint; faster return, unproven superiority over open
References
Wrist ganglion treatment: systematic review and meta-analysis
- 35 studies, 2,239 ganglia. Mean recurrence: open excision 21%, arthroscopic excision 6%, aspiration 59%
- In RCTs, surgical excision reduced recurrence by 76% versus aspiration; in cohort studies by 58%
- Complication rate: arthroscopic 4%, open excision 14%, aspiration 3%
The dorsal ganglion of the wrist: its pathogenesis, gross and microscopic anatomy, and surgical treatment
- 500 dorsal ganglia over 25 years; 346 followed a minimum of 9 months with only 3 recurrences
- Demonstrated a one-way, valve-like duct system between the scapholunate joint and the ganglion
- Cure depended on excising all attachments to the scapholunate ligament, not just the cyst
The treatment of dorsal wrist ganglia by radical excision
- 62 dorsal ganglia: although scapholunate origin is usual, attachments may also arise elsewhere over the dorsal capsule, especially near the capitate
- 2 recurrences; persistent discomfort after excision was not uncommon on review of 52 cases
- One patient developed scapholunate instability
Prospective outcomes of arthroscopic treatment of dorsal wrist ganglia
- 52 patients, mean follow-up 39 months; significant gains in flexion, extension and grip strength
- 9 recurrences (17.3%); mean time off work 14 days with 19 returning immediately
- Authors recommend arthroscopy as a primary treatment option for dorsal ganglia
Ganglion cysts of the wrist: pathophysiology, clinical picture, and management
- Roughly 50% of ganglia resolve spontaneously, supporting observation as first-line for asymptomatic cysts
- Mucin-coalescence theory: extra-articular mucin droplets coalesce, with cyst wall and pedicle forming later
- Aspiration carries high recurrence; surgery lowers recurrence but raises the complication rate
Further reading 1. Dias J, Buch K. Palmar wrist ganglion: does intervention improve outcome? A prospective study of the natural history and patient-reported treatment outcomes. J Hand Surg Br 2003;28(2):172-6. PMID: 12631492. 2. Thornburg LE. Ganglions of the hand and wrist. J Am Acad Orthop Surg 1999;7(4):231-8. PMID: 10434077. 3. Zubowicz VN, Ishii CH. Management of ganglion cysts of the hand by simple aspiration. J Hand Surg Am 1987;12(4):618-20. PMID: 3611666. 4. Westbrook AP, Stephen AB, Oni J, et al. Ganglia: the patient's perception. J Hand Surg Br 2000;25(6):566-7. PMID: 11106520. 5. Varley GW, Needoff M, Davis TR, et al. Conservative management of wrist ganglia. Aspiration versus steroid infiltration. J Hand Surg Br 1997;22(5):636-7. PMID: 9752922. 6. Horvath A, Zsidai B, Konaporshi S, et al. Treatment of primary dorsal wrist ganglion — a systematic review. J Wrist Surg 2022;12(2):177-90. PMID: 36926205. [PRISMA review; aspiration recurrence 7-72%, open excision 6-41%, arthroscopic 0-16%]