Temporary tethering of one side of an open physis to gradually correct angular deformity | intermediate
- Guided growth REQUIRES significant growth remaining — it works by tethering one side of an OPEN physis while the other side keeps growing. Near or after skeletal maturity it cannot work; an osteotomy is needed instead.
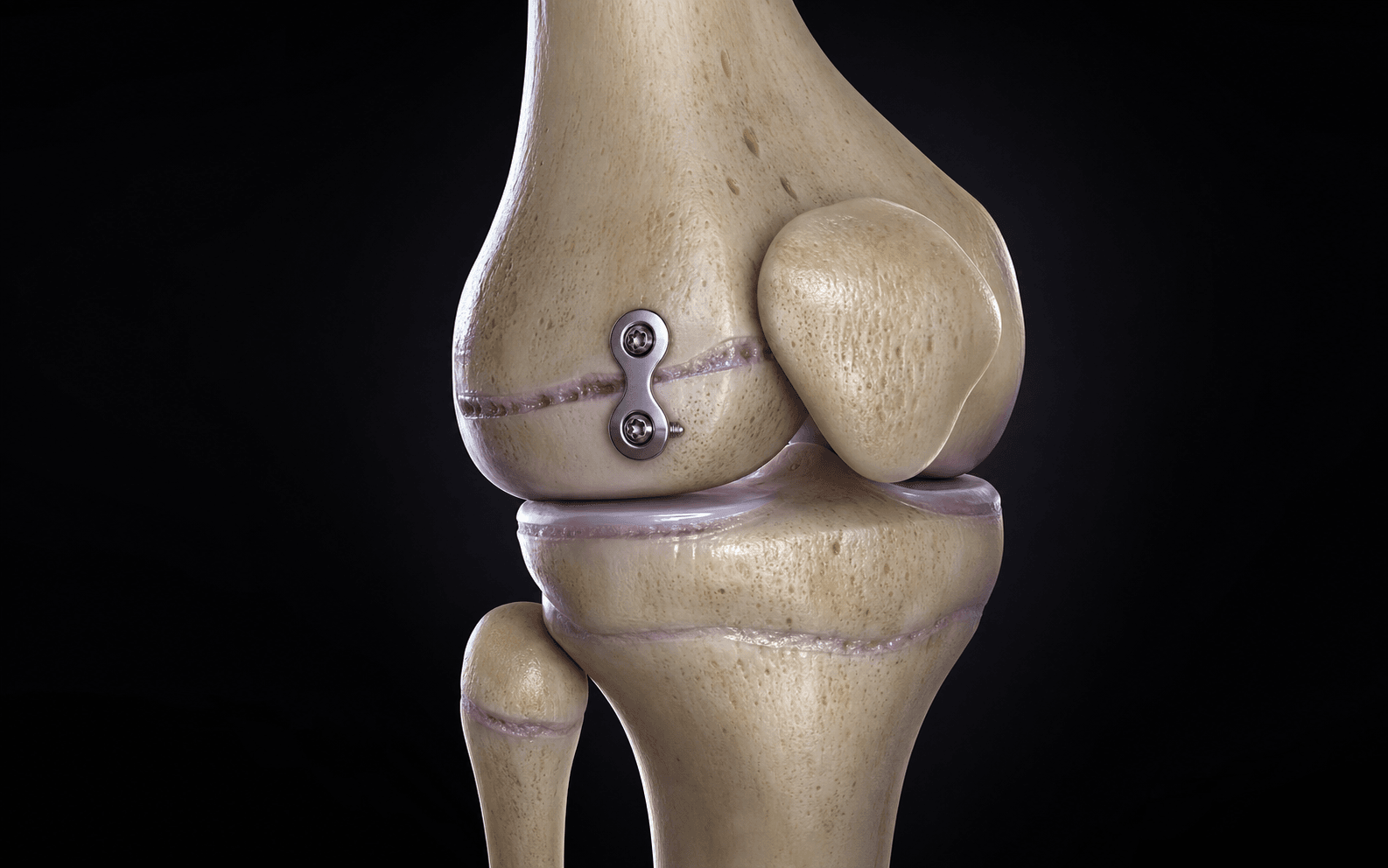
- The tension-band plate (eight-Plate) is a flexible extraperiosteal tether — a single screw in the epiphysis and a single screw in the metaphysis spanning the physis. The screws diverge as growth proceeds; the physis is NOT compressed or crossed.
- This is TEMPORARY and REVERSIBLE — the hardware is removed once alignment is corrected and the physis resumes symmetric growth. This is fundamentally different from permanent epiphysiodesis (for limb-length discrepancy) and from osteotomy.
- OVERCORRECTION is the principal pitfall — 'set and forget' is wrong. The child must be reviewed every 3 to 4 months with alignment radiographs and the plate removed PROMPTLY once neutral is reached, or the deformity reverses in the opposite direction.
When & Why
Indication. A child with a progressive pathological angular limb deformity — most often genu valgum or genu varum around the knee — with significant growth remaining, in whom conservative observation or non-operative care is no longer appropriate. Guided growth gradually corrects the deformity by tethering one side of an open physis so the opposite side keeps growing, swinging the limb back towards a neutral mechanical axis. Strong indications - Progressive pathological angular deformity (genu valgum or varum) with significant growth remaining (rule of thumb: at least 12 to 18 months of growth).
- Mechanical axis deviation beyond physiological limits for age, causing symptoms or documented progression.
- Blount disease (infantile and adolescent tibia vara) with an open, viable physis.
- Metabolic or rachitic deformity (for example hypophosphataemic rickets) once medical control is optimised.
- Sagittal-plane deformity — fixed knee flexion (anterior distal femoral plating) in cerebral palsy or dysplasia. Relative indications include post-traumatic partial physeal injury producing progressive angulation (with sufficient remaining physis), skeletal dysplasia (for example achondroplasia, multiple epiphyseal dysplasia) with symptomatic malalignment, asymmetric deformity at multiple levels (combined femoral and tibial plating), and mild leg-length asymmetry combined with angular deformity. Contraindications - Absolute — a closed or near-closed physis: there is no growth engine to drive correction, so the deformity persists and the family is misled; perform an osteotomy instead. Active infection at the operative site is the other absolute contraindication.
- Relative — physiological genu valgum or varum (a normal developmental variant to observe; physiological valgum peaks around 3 to 4 years and resolves), uncontrolled metabolic bone disease (correct the rickets first — the physis will not respond reliably), and a very stiff or abnormal physis (severe Blount, established physeal bar) where the response is unpredictable — counsel on slower correction and rebound. Consent specifically for the need for close follow-up and a second operation to remove the hardware, the risk of overcorrection if removal is delayed, rebound after removal (especially in young and pathological physes), incomplete correction if insufficient growth remains, implant prominence or irritation, infection, and the small risk of physeal injury from screw misplacement. The key principle — growth modulation, not correction at surgery. Guided growth does not acutely correct the deformity on the table. It tethers one side of an open physis (the convex, longer side over the deformity apex) so that the untethered side continues to grow, gradually swinging the limb back towards neutral. The correction is therefore biological and time-dependent, proportional to the growth rate of the involved physis and the remaining growth — which is why it cannot work at skeletal maturity and why surveillance matters as much as the operation itself. Setup. Supine on a radiolucent table with a sandbag or bump under the ipsilateral hip to control rotation. The image intensifier must be available and tested in both AP and lateral planes before draping. A thigh tourniquet is optional — many surgeons avoid it for these small extraperiosteal exposures. Standing full-length (hip-to-ankle) alignment radiographs are reviewed pre-operatively to measure mechanical axis deviation, mLDFA and MPTA, and to identify the CORA and decide which physis (or both) to plate and on which (convex) side.
The Operation
The goal: place a flexible two-hole tension-band plate extraperiosteally across one side of an open physis, with one screw cleanly in the epiphysis and one in the metaphysis, so that the tethered side slows while the open side keeps growing — gradually correcting the deformity. The exposure is small and gentle, but it is precise work under fluoroscopy: the whole game is localising the physis exactly and keeping both screws clear of it.

Operative sequence
- Supine on a radiolucent table, sandbag under the ipsilateral hip to control rotation; image intensifier tested in AP and lateral before draping.
- Use the image intensifier to identify the target physis precisely and mark the skin over the physis on the convex side of the deformity. The plate's central hole must sit over the physis, with screw trajectories diverging into epiphysis and metaphysis.
- Re-check the deformity direction against the standing alignment film so you mark the convex (longer) side, not the concave side.
- Make a small longitudinal incision centred over the physis on the convex side and dissect down to bone.
- The plate is placed extraperiosteally — preserve the periosteum and the perichondrial ring of LaCroix; do not strip the periosteum over the physis, because stripping itself can stimulate or arrest growth.
- A small, gentle exposure just big enough for the plate is all that is required.
- At the medial distal femur, protect the saphenous nerve and vein; at the lateral proximal tibia, protect the common peroneal nerve (which lies more proximally) and avoid the joint capsule.
- Place the plate so its central hole or eyelet lies over the physis.
- Insert the central guide wire along the physis under fluoroscopy to mark the level.
- Confirm in AP and lateral that the plate straddles the physis with the screw paths diverging away from it; a plate that is too proximal, too distal, or rotated will send the screws towards or across the physis.
- Insert the epiphyseal screw first — the epiphysis is smaller and this is the harder screw to place — then the metaphyseal screw, each through its plate hole, parallel to the physis but on its own side.
- Use cannulated self-tapping screws over the guide wires. The two screws converge slightly towards the plate but never cross the physis.
- As the child grows, these screws splay apart on follow-up films — the divergence is the sign that the construct is working.
- Take final AP and lateral fluoroscopic images: plate centred on the physis, both screws clear of the physis, no joint penetration, no screw breaching the far cortex.
- Irrigate. Close the periosteal or soft-tissue layer loosely, then skin. Apply a simple dressing — no rigid immobilisation is usually required.
- For isolated femoral genu valgum, a single medial distal femoral plate may suffice; for combined femoral and tibial deformity, plate both. Bilateral deformity can be addressed in the same sitting.
- Document exactly which physes were plated, so follow-up imaging and the timing of removal can be planned.
Both screws must straddle the physis — one purely in the epiphysis, one purely in the metaphysis. A screw that crosses the physeal cartilage acts like a transphyseal bar and causes a focal arrest with permanent deformity — the exact opposite of the intended effect. Confirm in two planes (AP and lateral) that each screw is entirely on its own side of the physis, and check that the epiphyseal screw has not breached the joint surface and that no screw is too long.
Do not strip the periosteum or disturb the perichondrial ring over the physis — subperiosteal stripping can itself disturb growth. Keep the incision and dissection minimal to limit implant prominence and infection risk. At the medial distal femur protect the saphenous nerve and vein; at the lateral proximal tibia protect the common peroneal nerve and avoid the joint capsule.
The physis is the radiolucent growth line, not the articular surface — they are close but distinct, and mistaking the joint line for the physis is a classic error. Re-check the deformity direction against the alignment film before incising so you mark the convex (longer) side. Coronal-only imaging misses sagittal screw malposition — always use fluoroscopy in two planes.
I place the epiphyseal screw first because the epiphysis is smaller and it is the harder one to get right. I confirm on AP and lateral that each screw is entirely on its own side of the physis. As the child grows these screws splay apart on follow-up films — that divergence tells me the construct is doing its job.
Confirm the exact physeal level fluoroscopically and mark it on the skin before incising. The central portion of the plate must sit precisely over the physis so that one screw goes cleanly into the epiphysis and the other cleanly into the metaphysis — never across the physis itself.


Aftercare & Complications
Rehabilitation & surveillance | Phase | Timing | Activity & immobilisation | Monitoring | |-------|--------|---------------------------|------------| | Early | Day 0 to 6 weeks | Weight-bear as tolerated; no rigid immobilisation; simple dressing; simple analgesia (paracetamol with or without an NSAID) | Review at 6 weeks — wound check, confirm mobilisation, baseline post-op alignment film | | Surveillance | Every 3 to 4 months | Full activity | Standing long-leg alignment radiographs; track the mechanical axis and screw divergence | | Removal | When neutral | Day-case plate removal | Prompt removal the moment the mechanical axis is neutral | | After removal | To skeletal maturity | Full activity | Continue alignment surveillance — watch for rebound | Surveillance is the defining feature. Review every 3 to 4 months with standing long-leg alignment radiographs, tracking the mechanical axis and watching the screws diverge as correction proceeds. Younger, fast-growing children must be reviewed more frequently — the distal femur corrects at roughly 9 to 10 mm per year, so it corrects and overshoots fast. Pathological physes (Blount, rickets, dysplasia) correct more slowly and less predictably; optimise metabolic disease throughout. Timely removal is the most important decision in the whole pathway. Remove the plate PROMPTLY once the mechanical axis is neutral — leaving it in causes overcorrection in the opposite direction. After removal the physis resumes symmetric growth, which is the basis of reversibility. Do not discharge at removal — continue alignment surveillance to skeletal maturity, because rebound (partial recurrence) can occur, particularly in young children and pathological physes, and may require a second episode of guided growth.
The operation that matters most in guided growth is timely hardware removal. I review every 3 to 4 months with standing alignment films and take the plate out as soon as the mechanical axis is neutral. In a young child, or a Blount knee, I warn the family early that rebound may mean a second episode of guided growth.
Why guided growth is different — reversibility - The flexible tension-band construct tethers one side of the physis without compressing or crossing it; after removal the previously slowed side resumes growth.
- This contrasts with permanent epiphysiodesis — the deliberate, irreversible ablation of a physis used for limb-length discrepancy (a separate indication, timed by growth-prediction methods).
- And with corrective osteotomy — an acute bony correction for the mature skeleton, or for severe or rapidly progressive deformity where no growth remains. Complications
- Incidence
- Common if follow-up lapses (the single most reported complication)
- Recognition
- Mechanical axis crosses neutral into the opposite deformity on serial standing films
- Prevention and management
- Prevention: review every 3 to 4 months; remove the plate promptly once neutral; closer review in fast-growing or young children. Management: remove the plate immediately; if significant, perform guided growth on the OPPOSITE side to re-correct
- Incidence
- Up to 10 to 20 percent or higher in young children and pathological physes (Blount, rickets, dysplasia)
- Recognition
- Recurrence of the original deformity on follow-up after hardware removal
- Prevention and management
- Prevention: consider deliberate mild overcorrection in high-risk physes; continue follow-up to maturity. Management: repeat episode of guided growth; treat the underlying metabolic disease
- Incidence
- Low with plates (higher historically with staples)
- Recognition
- Failure to correct or a paradoxical deformity; physeal bar on MRI or CT; a screw seen crossing the physis
- Prevention and management
- Prevention: screws must straddle (not cross) the physis; extraperiosteal placement; two-plane fluoroscopy. Management: bar resection if focal; completion epiphysiodesis with or without a contralateral procedure; osteotomy for established deformity
- Incidence
- Variable — higher in pathological physes and late presentation
- Recognition
- Mechanical axis fails to reach neutral despite adequate time; screws not diverging
- Prevention and management
- Prevention: confirm adequate growth remains pre-operatively; correct level (CORA); healthy physis. Management: continue if growth remains; if growth is exhausted, perform a corrective osteotomy
- Incidence
- Lower than with staples; screw breakage on removal reported
- Recognition
- Hardware breakage, screw back-out, plate prominence on radiograph; difficulty at removal
- Prevention and management
- Prevention: correct technique and implant selection; timely removal before excessive divergence. Management: retrieve broken hardware; revise the construct if correction is incomplete
- Incidence
- Common but minor
- Recognition
- Local tenderness, bursitis, prominence over the plate (especially medial distal femur, proximal tibia)
- Prevention and management
- Prevention: extraperiosteal low-profile placement through a small incision. Management: reassure; remove the hardware once correction is achieved (often resolves the symptoms)
- Incidence
- Low (less than 1 to 2 percent)
- Recognition
- Erythema, swelling, discharge, fever; raised inflammatory markers
- Prevention and management
- Prevention: sterile technique, prophylactic antibiotics, meticulous closure. Management: antibiotics; washout for deep infection; remove the hardware if infection persists
- Incidence
- Rare with careful technique
- Recognition
- Joint pain, effusion; a screw seen breaching the articular surface on imaging
- Prevention and management
- Prevention: fluoroscopic confirmation in two planes; appropriate screw length and trajectory. Management: reposition or exchange the screw
Viva & Exam Focus
GROWTHGROWTH — prerequisites and principles of guided growth
TETHERTETHER — assessing the angular deformity
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“An 8-year-old girl is referred with progressive, symptomatic genu valgum of the right knee. Standing long-leg radiographs show the mechanical axis lateral to the knee with an abnormal mLDFA and a normal MPTA. There is no metabolic disease. How would you manage her?”
“What is the difference between temporary hemiepiphysiodesis with a tension-band plate and a permanent epiphysiodesis, and why does the choice of implant (plate versus the older Blount staple) matter?”
“A 6-year-old boy with hypophosphataemic rickets had bilateral medial distal femoral tension-band plates inserted 18 months ago and was lost to follow-up. He now returns with the knees deformed in the OPPOSITE direction (varus) and one screw appears broken. What has happened and how do you manage him?”
Core principle
- Tethers ONE side of an OPEN physis so the other side keeps growing — gradual, biological, growth-dependent correction
- REQUIRES significant growth remaining (rule of thumb: at least 12 to 18 months) — no growth means no correction
- TEMPORARY and REVERSIBLE — remove the hardware once corrected; the physis resumes symmetric growth
- Hueter-Volkmann: compression slows growth, reduced load accelerates growth — the biomechanical basis
- NOT the same as permanent epiphysiodesis (for limb-length discrepancy) or osteotomy (acute or mature correction)
Deformity planning
- Standing full-length (hip-to-ankle) alignment radiograph; measure mechanical axis deviation
- Identify the CORA — measure mLDFA (femur) and MPTA (tibia)
- Genu valgum: CORA usually at the distal femur — plate the MEDIAL distal femoral physis
- Genu varum or Blount: CORA usually at the proximal tibia — plate the LATERAL proximal tibial physis
- Always plate the CONVEX (longer) side over the responsible physis; combined deformity may need both levels
Growth rates (planning)
- Distal femur about 9 to 10 mm per year — fastest; corrects and overshoots quickest; review more often
- Proximal tibia about 6 mm per year — common Blount correction site
- Distal tibia about 5 mm per year — ankle valgus (medial malleolar plating)
- Faster physis plus younger child equals faster correction AND faster overcorrection
- Pathological physes (Blount, rickets, dysplasia) correct slowly and rebound more
Implant — tension-band plate (eight-Plate)
- Flexible, extraperiosteal tension band — Stevens (2007)
- One epiphyseal plus one metaphyseal screw straddling (NOT crossing) the physis
- Screws DIVERGE on follow-up films as correction proceeds — the sign it is working
- Has largely replaced the rigid Blount staple (higher extrusion, breakage, permanent arrest)
- The physis is neither compressed circumferentially nor crossed — hence reversibility
Operative technique — key steps
- Localise the physis fluoroscopically in two planes — not the joint line
- Small longitudinal incision over the convex side; EXTRAPERIOSTEAL placement (do not strip the periosteum or perichondrial ring)
- Plate central hole over the physis; central guide wire along the physis
- Epiphyseal screw FIRST, then metaphyseal — each on its own side of the physis
- Confirm both screws clear of the physis and the joint in AP and lateral; protect the saphenous nerve and vein (medial femur) and the peroneal nerve (lateral proximal tibia)
Danger zones
- Insufficient growth remaining — confirm before offering guided growth, else do an osteotomy
- Screw crossing the physis — causes a focal bar and permanent arrest; the cardinal technical error
- Set-and-forget — overcorrection follows lapsed follow-up; review every 3 to 4 months
- Wrong level (ignoring the CORA) — leaves the deformity uncorrected and creates translation
- Subperiosteal stripping over the physis — can itself disturb growth
Follow-up and removal (the defining feature)
- Review at 6 weeks, then every 3 to 4 months with standing alignment radiographs
- Track the mechanical axis and screw divergence
- REMOVE the plate PROMPTLY once the mechanical axis is neutral — the most important decision
- Delayed removal equals overcorrection in the opposite direction
- Continue follow-up to maturity after removal — rebound may need a second episode
Complications
- Overcorrection — commonest; from delayed removal; remove the plate, re-correct the opposite side if needed
- Rebound or recurrence after removal — higher in young or pathological physes; may repeat guided growth
- Physeal injury or premature arrest — low with plates; from a screw crossing the physis; bar resection or osteotomy
- Incomplete correction — insufficient growth or wrong level; osteotomy if growth exhausted
- Implant prominence or irritation, screw breakage (on removal), infection (less than 1 to 2 percent)
Special cases
- Blount disease: lateral proximal tibial plate in early disease (open, viable physis); osteotomy for advanced stages or a bar
- Rickets or metabolic: optimise medical control first; slower correction, higher recurrence; often combined femoral plus tibial
- Skeletal dysplasia: symptomatic malalignment; unpredictable physeal response; close surveillance
- Sagittal plane: anterior distal femoral plating for fixed knee flexion (for example cerebral palsy)
- Permanent epiphysiodesis (separate topic): irreversible, for limb-length discrepancy — do not confuse with guided growth
Background & Evidence
Background. Angular limb deformity in a child is common, but most is physiological — physiological genu varum in the toddler resolves, and physiological genu valgum peaks around 3 to 4 years before resolving. Guided growth is reserved for progressive pathological deformity with growth remaining. Understanding the physis and the Hueter-Volkmann principle is what makes the technique rational. The physis (growth plate). A cartilaginous disc responsible for longitudinal growth. Its zones, from the epiphyseal to the metaphyseal side, are: | Zone | Function | Vulnerability | |------|----------|---------------| | Reserve (germinal) | Stem and resting chondrocytes, matrix storage | Nutrient supply from epiphyseal vessels | | Proliferative | Chondrocyte division, longitudinal stacking | Site of active growth — drives correction | | Hypertrophic | Chondrocyte enlargement, matrix calcification | Weakest zone — the plane of Salter-Harris fractures | | Provisional calcification or metaphysis | Ossification, vascular invasion | Metaphyseal blood supply | Hueter-Volkmann principle: compression across a physis slows growth; reduced load accelerates growth. Tethering one side mechanically modulates growth on that side — the biomechanical basis of guided growth. Why a tension band works. A flexible plate fixed by one epiphyseal and one metaphyseal screw spans the physis on the convex side. The plate resists separation of the two screws on that side, slowing growth there, while the opposite (open) side grows normally. As the open side grows, the limb angulates back towards neutral, and the screws diverge over time on imaging — the sign the construct is working. Because the physis is neither compressed circumferentially nor crossed, growth resumes after hardware removal (reversibility). Growth rates (approximate — central to planning): | Physis | Approximate growth rate | Contribution | |--------|------------------------|--------------| | Distal femur | About 9 to 10 mm per year | Fastest lower-limb physis — corrects quickest | | Proximal tibia | About 6 mm per year | Common site for varus (Blount) correction | | Proximal femur | About 3 mm per year | Minor contributor to length | | Distal tibia | About 5 mm per year | Ankle valgus correction (medial malleolar plating) | A faster physis means faster correction — and faster overcorrection — so review fast-growing and young children more often. The correction rate also depends on the distance of the plate from the joint and on the health of the physis (idiopathic is faster than pathological). Deformity analysis — planning at the CORA. The CORA (centre of rotation of angulation) is the intersection of the proximal and distal mechanical or anatomical axis lines — the true apex of the deformity. For genu valgum the apex is usually at the distal femur (an abnormal mLDFA) — plate the medial distal femoral physis. For genu varum or Blount the apex is usually at the proximal tibia (an abnormal MPTA) — plate the lateral proximal tibial physis. Combined femoral and tibial deformity may both need plating. Always plate on the convex (longer) side over the responsible physis.
- Tension-Band Plate
- Flexible tether on one side of the physis
- Blount Staple
- Rigid staple across the physis
- Permanent Epiphysiodesis
- Permanent destruction of the physis
- Corrective Osteotomy
- Acute bony correction
- Tension-Band Plate
- Yes (remove the hardware)
- Blount Staple
- Partly (remove the staples)
- Permanent Epiphysiodesis
- No
- Corrective Osteotomy
- No
- Tension-Band Plate
- Yes (essential)
- Blount Staple
- Yes
- Permanent Epiphysiodesis
- Yes (for LLD timing)
- Corrective Osteotomy
- No
- Tension-Band Plate
- Angular deformity
- Blount Staple
- Angular deformity (historical)
- Permanent Epiphysiodesis
- Limb-length discrepancy
- Corrective Osteotomy
- Mature, severe, or acute
- Tension-Band Plate
- Low (less extrusion)
- Blount Staple
- Higher (extrusion or breakage)
- Permanent Epiphysiodesis
- Not applicable
- Corrective Osteotomy
- Nonunion or malunion
- Tension-Band Plate
- Low
- Blount Staple
- Higher
- Permanent Epiphysiodesis
- Intended
- Corrective Osteotomy
- Not applicable
Key evidence. Stevens (2007) described the non-locking extraperiosteal two-hole tension-band plate ("eight-Plate") for guided growth — a flexible construct relying on the tension-band principle rather than physeal compression, hinging open as growth proceeds; 32 of 34 patients corrected to neutral, correction roughly 30 percent faster than stapling, with no permanent growth arrests. The flexible construct avoids the compression across the whole physis seen with staples, reducing the risk of permanent arrest and allowing the physis to recover after removal. The rigid Blount staple (Blount and Clarke, 1949) was the historical standard but carried higher rates of implant extrusion, breakage, migration and unintended permanent arrest. Stevens and Klatt (2008) directly documented 45 percent staple migration and 41 percent rebound, contrasted with no migration in the plate cohort — which is why plating has largely superseded stapling. Idiopathic versus pathological physes. Idiopathic genu valgum or varum corrects predictably and relatively quickly — Ballal and colleagues reported correction significantly faster in children under 10 years (p equals 0.05), with only one rebound and no permanent tethers. Blount, rickets and skeletal dysplasia correct more slowly, less completely, and rebound more often — these patients need closer surveillance and counselling about repeat procedures. In early-onset Blount disease, however, tension-band plating nonetheless improved Langenskiold stage and mechanical-axis alignment in most limbs (Hanstein and colleagues, 2023) and is now advocated as first-line surgical treatment.
References
Guided growth for angular correction: a preliminary series using a tension band plate
- Prospective series of 34 patients with 65 deformities of the femur and/or tibia treated with a non-locking extraperiosteal two-hole plate relying on the tension-band principle rather than physeal compression
- 32 of 34 patients (63 deformity levels) corrected to neutral at a mean of 11 months, after which the hardware was removed
- Rate of correction was approximately 30 percent more rapid than with stapling, with NO permanent growth arrests
- 4 patients with bilateral idiopathic genu valgum rebounded and underwent repeat guided growth; 63 of 65 (97 percent) osteotomies were avoided
Correcting genu varum and genu valgum in children by guided growth: temporary hemiepiphysiodesis using tension band plates
- 25 children (37 legs, 51 segments) with coronal-plane deformity around the knee treated with a flexible two-hole plate; mean correction time 16.1 months
- Mean correction rate 0.7 degrees per month at the femur and 0.5 degrees per month at the tibia, and 1.2 degrees per month when femur and tibia were treated concurrently
- Correction was significantly faster in children under 10 years of age (p equals 0.05)
- Only one rebound deformity and NO permanent physeal tethers after a follow-up of 6 to 32 months post-removal
Guided growth for pathological physes: radiographic improvement during realignment
- 14 children with rickets (10 treated with staples, 4 with eight-plates) undergoing 68 guided-growth procedures under medical management
- Staples showed 45 percent implant migration (24 of 53) and 41 percent rebound deformity, whereas the eight-plate cohort had NO hardware migration
- Gradual normalisation of the mechanical axis improved the radiographic appearance and width of physes not only at the knee but also at the hip and ankle
- The authors recommend early guided growth to preserve physeal quality and defer or avoid osteotomy in metabolic bone disease
The effect of guided growth surgery on Langenskiold stage and mechanical axis in early-onset Blount disease
- 25 limbs in 16 children with early-onset Blount disease treated with tension-band plating at a mean age of 5.8 years; implants in situ a mean of 1.9 years
- Langenskiold stage improved in 84 percent of limbs (21 of 25) at latest follow-up and resolved completely in 28 percent
- Mechanical axis deviation improved in 22 of 23 limbs, with neutral or valgus alignment achieved in 87 percent at hardware removal
- 70 percent maintained improved alignment at final follow-up; the authors conclude tension-band plating should be first-line surgical treatment for early-onset Blount disease
Further reading - Blount WP, Clarke GR (1949). Control of bone growth by epiphyseal stapling: a preliminary report. Journal of Bone and Joint Surgery (American) 31A(3):464 to 478 — the original description of physeal stapling for growth control; the historical comparator superseded by tension-band plating.
- Paley D (2002). Principles of Deformity Correction. Springer — the reference text on CORA-based deformity analysis (mechanical axis, mLDFA, MPTA) underpinning level selection for guided growth.