Bilateral transpedicular vertebral augmentation with an inflatable bone tamp and PMMA cement for painful osteoporotic or pathological compression fractures · intermediate
- Patient selection is the operation: a subacute fracture (less than 3 months) with bone-marrow oedema on MRI (bright on STIR or T2 fat-suppressed) and mechanical pain that correlates with the level on examination yields the best results; a chronic fracture without oedema responds poorly.
- Bilateral transpedicular cannulation under true AP and lateral fluoroscopy is mandatory. The needle tip must stay lateral to the medial pedicle cortex on AP until the posterior wall is crossed on lateral — a medial breach endangers the thecal sac and cord.
- The inflatable bone tamp creates a contained cavity and elevates the endplates before cement is injected. This allows higher-viscosity PMMA to be delivered at lower pressure than vertebroplasty and reduces (but does not eliminate) cement leakage.
- Cement injection is performed under continuous lateral fluoroscopy with frequent AP checks. Posterior-wall breach, venous filling or disc-space extravasation demands immediate cessation and reassessment before resuming.
- “MRI is essential for selection — STIR or T2 fat-suppressed sequences show bone-marrow oedema; its absence predicts poor pain relief and is a relative contraindication.
- “The transpedicular trajectory must enter the body through the pedicle without a medial breach (cord and thecal sac) or a lateral breach (segmental vessels and pleura in the thoracic spine).
- “Cement should fill the anterior two-thirds to three-quarters of the vertebral body; overfilling raises leakage risk while underfilling gives inadequate stabilisation.
- “Adjacent-level fracture risk is increased after kyphoplasty (about 10–20 percent at 1 year) — counsel patients on osteoporosis treatment and fall prevention.
When & Why
The indication in one line. Balloon kyphoplasty is for a painful vertebral compression fracture with mechanical axial pain that correlates to the fractured level, where the fracture is subacute (typically less than 3 months) and shows bone-marrow oedema on MRI (STIR or T2 fat-suppressed sequences), and where conservative management — analgesia, bracing and physiotherapy for at least 4–6 weeks — has failed. Patient selection is the operation. The single strongest predictor of a good result is MRI bone-marrow oedema: a hypointense fracture line on T1 with bright STIR signal. Chronic fractures without oedema respond poorly (pain relief falls below 50 percent) and are a relative contraindication. Oedema is the gatekeeper — confirm it before offering the procedure. Absolute indications. A painful osteoporotic or pathological compression fracture with mechanical pain correlating to the level; a subacute fracture (less than 3 months) with bone-marrow oedema on MRI; failure of 4–6 weeks of conservative care (analgesia, bracing, physiotherapy); or a pathological fracture (myeloma, lymphoma, metastasis) with mechanical pain and limited life expectancy, where stabilisation improves quality of life. Relative indications. Progressive kyphosis with sagittal imbalance and secondary pain; multiple contiguous fractures where staged augmentation may prevent further collapse; and severe osteoporosis in whom prolonged bracing is poorly tolerated. Absolute contraindications. Active spinal infection or osteomyelitis at the target level; a neurological deficit attributable to the fracture (cord or cauda equina compression needing decompression); a burst fracture with significant retropulsion and canal compromise; and coagulopathy that cannot be corrected. Relative contraindications. A chronic fracture without oedema on MRI; greater than 50 percent vertebral height loss with severe endplate fragmentation (technical difficulty); and allergy to PMMA cement components.
Do not offer kyphoplasty for a chronic fracture without bone-marrow oedema on STIR or T2 fat-suppressed MRI — response rates fall below 50 percent. The procedure relieves a fracture that is still actively oedematous and mechanically painful; an old, settled fracture will not benefit.
Special situations.
- Pathological (tumour) fractures are excellent candidates when the goal is palliation: take a biopsy at the time of cannulation if the diagnosis is uncertain, expect to use smaller cement volumes, and add posterior stabilisation if there is instability or neurological compromise. Leakage consequences may be greater when tumour has eroded the posterior wall.
- Multiple contiguous levels are best staged — two levels per session — to limit cement load and operative time; plan caudal to cranial and reassess alignment after each stage.
Consent specifically for cement leakage (5–10 percent), neurological injury (less than 1 percent), pulmonary cement embolism (3–5 percent, mostly asymptomatic), adjacent-level fracture (10–20 percent at 1 year), infection (less than 1 percent), and the possibility of incomplete pain relief. Counsel that the procedure treats the fracture, not the underlying osteoporosis, which must be managed medically. Setup. Prone on a radiolucent table with chest and pelvic bolsters allowing free abdominal excursion (this lowers epidural venous pressure and bleeding), the spine in slight extension to help endplate reduction. High-quality biplanar fluoroscopy is mandatory — obtain true AP and lateral projections before skin preparation. Single-dose cefazolin at induction (vancomycin if penicillin-allergic); consider vancomycin powder in the wound for high-risk patients. General anaesthesia or conscious sedation per patient tolerance and fracture acuity.
The Operation
The goal is to stabilise the fractured vertebra and relieve mechanical pain by creating a contained cavity inside the vertebral body with an inflatable bone tamp, then filling that cavity with high-viscosity PMMA cement at low pressure — achieving partial height restoration and kyphosis correction with a lower leakage rate than vertebroplasty. The whole procedure is percutaneous, through a bilateral transpedicular corridor, under continuous biplanar fluoroscopy. Why the transpedicular corridor is safe. The pedicle connects the posterior elements to the vertebral body. Advancing a needle down the pedicle's long axis keeps the instrument away from the exiting nerve root (which lies in the foramen just inferior to the pedicle) and the thecal sac and cord (which lie immediately medial to the medial pedicle wall). The posterior vertebral wall is the critical depth landmark — on lateral fluoroscopy the cannula tip must reach, but not breach, the posterior wall before entering the body. Cement can escape along the basivertebral and segmental veins (draining to the azygos system and the vena cava, causing pulmonary embolism) or through fractured endplates into the disc — which is why real-time imaging during injection is non-negotiable.
Operative sequence
- Prone on a radiolucent table with chest and pelvic bolsters; free abdominal excursion; spine in slight extension.
- Obtain true AP and lateral projections before prepping: on AP the spinous process sits exactly midway between the two pedicles, and on lateral the endplates are superimposed. Any obliquity produces a misleading pedicle position and is the root cause of medial or lateral breach.
- Single-dose cefazolin at induction.
- Identify the target vertebra by counting from a fixed landmark (usually L5 or S1) and cross-check against the preoperative MRI.
- On true AP, plan the skin entry 1–2 cm lateral to the pedicle shadow, angled along the pedicle axis so the needle converges to end in the anterior third of the body on lateral view.
- Infiltrate skin and periosteum with local anaesthetic.
- Advance 11- or 13-gauge Jamshidi needles through each pedicle under continuous AP fluoroscopy. The needle tip must remain lateral to the medial pedicle cortex on AP until the posterior wall has been crossed on lateral — only then may it travel medially into the body.
- Advance to the posterior third of the vertebral body, then repeat on the contralateral side.
- Remove the trocar and pass a guidewire or working cannula.
- Confirm both cannulas lie within the body on AP and lateral views before proceeding.
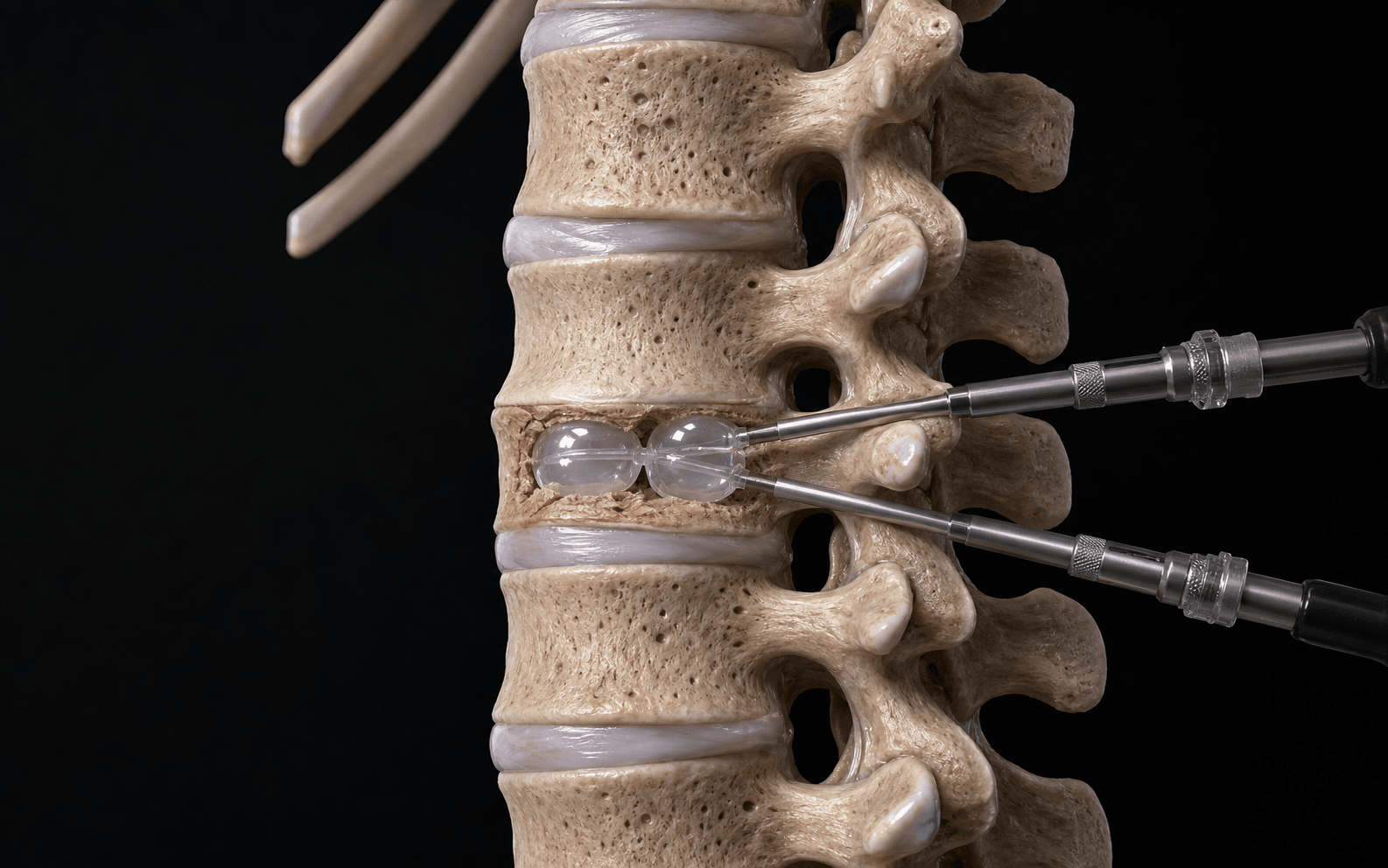
- Pass the deflated balloon tamp through each working cannula into the anterior third of the body.
- Inflate slowly in 0.5 mL increments under lateral fluoroscopy; typical volumes are 2–4 mL per side. Stop when the endplates are elevated or maximum pressure (about 300–400 psi) is reached.
- Deflate and withdraw the tamp, leaving a contained cavity.
- Mix high-viscosity PMMA per the manufacturer's instructions and allow it to reach a toothpaste-like consistency (typically 4–6 minutes after mixing) before loading the delivery system.
- The cavity created in Step 5 is exactly what permits this higher-viscosity, lower-pressure injection.
- Under continuous lateral fluoroscopy, inject cement slowly through both cannulas (simultaneously or sequentially), filling the anterior two-thirds to three-quarters of the vertebral body.
- Watch constantly for posterior-wall breach, venous filling, or disc-space extravasation. Stop immediately if any appears — it is always safer to leave a small unfilled region than to push cement into the canal or veins.
- Obtain final AP and lateral images to confirm cement position and distribution.
- Remove the cannulas while the cement is still soft, to avoid pulling cement tracks.
- Close the stab wounds with absorbable sutures or adhesive strips. No drain is required.
Implants. The only implant is PMMA bone cement — typically 3–6 mL per level. No metallic hardware is used; the cement interdigitates with trabecular bone and gives immediate stabilisation by mechanical interlock once cured.
On AP view the needle tip must stay lateral to the medial pedicle cortex until the posterior wall is crossed on lateral view. A medial breach places the thecal sac and cord at direct risk; a lateral breach in the thoracic spine risks the segmental vessels and the pleura. Stop about 5 mm short of the anterior cortex to avoid anterior penetration. If the trajectory feels wrong, withdraw and redirect — never force.
Inject under live lateral fluoroscopy with an assistant ready to stop instantly. Posterior-wall breach with cement in the canal is a surgical emergency: stop, assess neurology, obtain an urgent CT, and decompress if a deficit develops. Venous opacification threatens pulmonary embolism: stop, give supportive care, and arrange a CT pulmonary angiogram. Disc-space leakage is usually asymptomatic but can accelerate adjacent degeneration.
Obtain a true AP with the spinous process perfectly centred between the pedicles, and a perfect lateral with superimposed endplates, before starting. Any obliquity will mislead you into a medial or lateral breach. Plan the skin entry so the Jamshidi traverses the pedicle in a slightly converging trajectory that ends in the anterior third of the body on lateral view.
Inflate the balloon in 0.5 mL increments while watching the endplates on lateral view. If an endplate fractures rather than elevates, stop immediately — the goal is a contained cavity, not maximal height at the cost of creating a leakage pathway. In very osteoporotic bone, use lower final volumes and accept modest correction.
Do not inject until the PMMA has reached a thick, toothpaste-like consistency, and inject under live lateral fluoroscopy. If you see posterior extravasation or venous opacification, stop, wait about 30 seconds, and reassess. It is always safer to leave a small unfilled region than to push cement into the canal or veins.
Aftercare & Complications
Immediate recovery. Mobilise as tolerated within 2–4 hours; no bracing is required. Analgesia with paracetamol, NSAIDs (if renal function allows) and a short course of weak opioid if needed. Most patients report a substantial reduction in their pre-operative pain within 24 hours. Standing radiographs at 4–6 weeks assess alignment and screen for adjacent fractures. Return to function.
- Light activities — immediately
- Driving — when comfortable, usually 3–7 days
- Heavy lifting — avoid for 6 weeks
- Sedentary work — within 1 week; manual work — 4–6 weeks Treat the disease, not just the fracture. Every patient needs a formal osteoporosis assessment initiated or optimised: a DEXA scan if not recent, calcium and vitamin D supplementation, antiresorptive or anabolic therapy per guidelines and fracture risk, and a fall-prevention programme. The augmentation stabilises one fracture; without medical therapy the next one follows.
- Incidence
- 5–10 percent
- Recognition
- Cement seen outside the body on fluoroscopy — usually the disc space or paravertebral veins
- Prevention & management
- Cavity creation, high-viscosity cement, slow injection under imaging. Observe; most need nothing
- Incidence
- less than 1 percent
- Recognition
- New radicular pain, weakness or sensory loss immediately after the procedure
- Prevention & management
- Stop at the first posterior extravasation. Urgent CT; surgical decompression if a progressive deficit or cord compression
- Incidence
- 3–5 percent (mostly asymptomatic)
- Recognition
- Sudden hypoxia, chest pain or hypotension during injection
- Prevention & management
- High-viscosity cement; avoid venous filling. Supportive ventilation; anticoagulation or endovascular retrieval if symptomatic
- Incidence
- 10–20 percent at 1 year
- Recognition
- New mechanical pain at an adjacent level, confirmed on MRI or radiographs
- Prevention & management
- Optimise osteoporosis therapy and fall prevention. Repeat augmentation at the new level if criteria are met
- Incidence
- less than 1 percent
- Recognition
- Delayed back pain, fever, raised CRP or ESR; MRI shows disc enhancement
- Prevention & management
- Strict sterile technique, prophylactic antibiotics. IV antibiotics for 6 weeks; debridement if abscess or instability
- Incidence
- 2–4 percent
- Recognition
- Sudden loss of endplate contour on fluoroscopy during balloon inflation
- Prevention & management
- Gradual 0.5 mL inflation; lower volumes in severe osteoporosis. Accept modest correction and inject with extra caution
Viva & Exam Focus
KYPHOKYPHO — patient selection & safety
TAMPTAMP — the operative sequence
Stepwise flow for safe balloon kyphoplasty
Critical danger structures and exam traps
A medial breach during cannula placement lets the trochar enter the spinal canal and injure the thecal sac or cord. Use true AP and lateral fluoroscopy throughout: on AP the medial wall must stay lateral to the pedicle shadow until the cannula has passed the posterior wall. Any medial deviation needs immediate redirection.
The posterior vertebral wall is the critical barrier; a breach lets cement enter the canal and compress the neural elements. Posterior-wall fracture lines or tumour erosion are common in pathological fractures. Continuous lateral fluoroscopy during injection is mandatory; any posterior extravasation demands immediate stoppage.
The basivertebral and segmental veins communicate directly with the vertebral body; cement can reach the vena cava and embolise to the lungs. High-pressure injection or low-viscosity cement increases venous filling. Use higher-viscosity PMMA after cavity creation and inject slowly under real-time imaging; stop if any venous opacification appears.
Over-aggressive balloon inflation in severely osteoporotic bone can fracture the superior or inferior endplate rather than elevate it. This opens a direct pathway for cement leakage into the disc and may worsen kyphosis. Inflate the tamp gradually in 0.5 mL increments while monitoring endplate position on lateral fluoroscopy.
Kyphoplasty alters load transfer through the stiffened augmented vertebra, increasing stress at the adjacent levels. New fractures occur in 10–20 percent of patients within 1 year. Optimise osteoporosis pharmacotherapy (bisphosphonates, denosumab or anabolic agents) and consider prophylactic augmentation only in highly selected cases.
Sudden desaturation, hypotension or chest pain during or immediately after cement injection signals embolism. Stop the injection at once, give supportive ventilation, and obtain an urgent CT pulmonary angiogram. Most small emboli are asymptomatic; larger fragments may need endovascular retrieval or anticoagulation in consultation with interventional radiology and respiratory teams.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 72-year-old woman with known osteoporosis presents with 8 weeks of severe mechanical mid-thoracic pain after a minor fall. MRI shows a T8 compression fracture with bone-marrow oedema. She has failed bracing and analgesia. How do you decide whether balloon kyphoplasty is appropriate, and what are the key technical points?”
“During balloon inflation at L1 you notice on lateral fluoroscopy that the superior endplate is fracturing rather than elevating. What do you do?”
“You are performing kyphoplasty at T12 in a patient with myeloma. During cement injection on the right side you see immediate posterior extravasation on lateral fluoroscopy. The patient is under general anaesthesia. What is your response?”
Patient selection
- Subacute fracture (less than 3 months) with mechanical pain and MRI bone-marrow oedema on STIR or T2 fat-sat
- Osteoporotic or pathological (myeloma, metastasis) compression fractures
- Failed 4–6 weeks of conservative care (analgesia, bracing, physiotherapy)
- No neurological deficit, no active infection, no burst component with retropulsion
- Chronic fractures without oedema respond poorly — MRI is mandatory
Key anatomical safety points
- The transpedicular corridor avoids the exiting nerve root (inferior) and the thecal sac (medial)
- True AP and lateral fluoroscopy is essential — a medial pedicle breach risks the cord
- The posterior wall is the critical depth limit before entering the body
- Basivertebral and segmental veins communicate directly with the vena cava — venous cement embolism risk
- The anterior two-thirds to three-quarters of the body is the safe cement fill zone
Operative sequence
- Prone positioning with slight extension; biplanar fluoroscopy mandatory
- Bilateral transpedicular Jamshidi needles to the posterior third of the body
- Inflatable bone tamp to the anterior third; inflate gradually (0.5 mL increments) under lateral view
- High-viscosity PMMA after cavity creation; continuous lateral fluoroscopy during injection
- Stop at the first sign of posterior-wall breach, venous filling or disc extravasation
Advantages over vertebroplasty
- Cavity creation allows higher-viscosity cement at lower pressure
- Modest height restoration (3–5 mm anterior) and kyphosis correction (3–8 degrees)
- Lower cement leakage rate (5–10 percent versus 20–30 percent)
- Similar pain relief and adjacent-fracture rates
Complications
- Cement leakage: 5–10 percent (mostly asymptomatic); posterior breach risks neural injury (less than 1 percent)
- Pulmonary cement embolism: 3–5 percent (mostly small and asymptomatic)
- Adjacent-level fracture: 10–20 percent at 1 year — requires osteoporosis optimisation
- Infection: less than 1 percent — strict sterile technique and prophylactic antibiotics
- Endplate fracture during tamp inflation: 2–4 percent — stop inflation, accept modest correction
Post-operative care
- Mobilise the same day; no bracing required
- Standing radiographs at 4–6 weeks to assess alignment and adjacent levels
- Initiate or optimise osteoporosis pharmacotherapy (DEXA, calcium and vitamin D, antiresorptive or anabolic)
- A fall-prevention programme is essential
- Pathological fractures: consider biopsy at the time of the procedure; smaller cement volumes; a palliative goal
Evidence highlights
- FREE trial: kyphoplasty superior to conservative care for pain and function at 1 to 12 months
- VERTOS II: vertebroplasty accelerates pain relief over conservative care
- Direct comparisons: similar pain scores, modestly greater height restoration with kyphoplasty
- Cement leakage is lower with kyphoplasty but not eliminated
- Adjacent-fracture rates are comparable between techniques; ongoing medical management is key
Background & Evidence
How kyphoplasty differs from vertebroplasty. Both deliver PMMA cement into a painful fractured vertebra for rapid pain relief. Balloon kyphoplasty first creates a contained cavity with the inflatable bone tamp before injection; this permits use of higher-viscosity cement at lower pressure and aims for partial height restoration and kyphosis correction. Vertebroplasty injects cement directly, without prior cavity creation. Landmark evidence. The FREE trial (Wardlaw, 2009) showed kyphoplasty superior to non-surgical care for pain and function at one month, with benefit sustained to 12 months and cement leakage in 9.5 percent with no neurological sequelae. VERTOS II (Klazen, 2010) showed vertebroplasty accelerates pain relief over conservative care. Head-to-head comparisons (Liu, 2010) show equivalent pain scores but modestly greater height restoration and kyphosis correction with kyphoplasty, at the cost of slightly longer operative time. Cement leakage is lower with kyphoplasty but not eliminated; adjacent-fracture rates are comparable between the two techniques. The KAST study and the Taylor meta-analysis confirm durable pain reduction to 24 months with rare major neurological complications.
- Balloon kyphoplasty
- 70–85 percent substantial improvement
- Vertebroplasty
- 70–85 percent substantial improvement
- Balloon kyphoplasty
- 3–5 mm average
- Vertebroplasty
- 1–2 mm average
- Balloon kyphoplasty
- 3–8 degrees
- Vertebroplasty
- 1–3 degrees
- Balloon kyphoplasty
- 5–10 percent
- Vertebroplasty
- 20–30 percent
- Balloon kyphoplasty
- 10–20 percent
- Vertebroplasty
- 10–20 percent
- Balloon kyphoplasty
- 40–60 minutes (two levels)
- Vertebroplasty
- 25–40 minutes (two levels)
References
Balloon kyphoplasty versus non-surgical fracture management for treatment of painful vertebral body compression fractures (FREE)
- FREE trial: 300 patients randomised to kyphoplasty or non-surgical care
- Kyphoplasty produced a greater improvement in SF-36 physical component score at 1 month (difference 5.2 points), sustained to 12 months
- Pain reduction was rapid and maintained; cement leakage occurred in 9.5 percent with no neurological sequelae
Vertebroplasty versus conservative treatment in acute osteoporotic vertebral compression fractures (VERTOS II)
- VERTOS II: 202 patients; vertebroplasty versus conservative care
- Vertebroplasty reduced pain scores by 2.6 points more than conservative care at 1 month
- Benefit persisted to 12 months; 97 percent technical success
Kyphoplasty versus vertebroplasty for the treatment of painful osteoporotic vertebral compression fractures
- Randomised comparison of 100 patients
- Both techniques produced equivalent pain relief at 6 months
- Kyphoplasty achieved greater anterior height restoration (4.2 mm versus 1.8 mm) and kyphosis correction
Balloon kyphoplasty and vertebroplasty for vertebral compression fractures: a systematic review and meta-analysis of 2 years' follow-up
- Pooled analysis of 17 studies, 1093 patients
- Clinically significant pain reduction maintained to 24 months
- Cement leakage 8.6 percent (mostly asymptomatic); neurological injury 0.2 percent
Adjacent vertebral failure after balloon kyphoplasty: a biomechanical and clinical analysis
- Finite-element modelling combined with a clinical cohort
- An augmented vertebra increases adjacent-level stress; the new-fracture rate is about 15 percent at 1 year