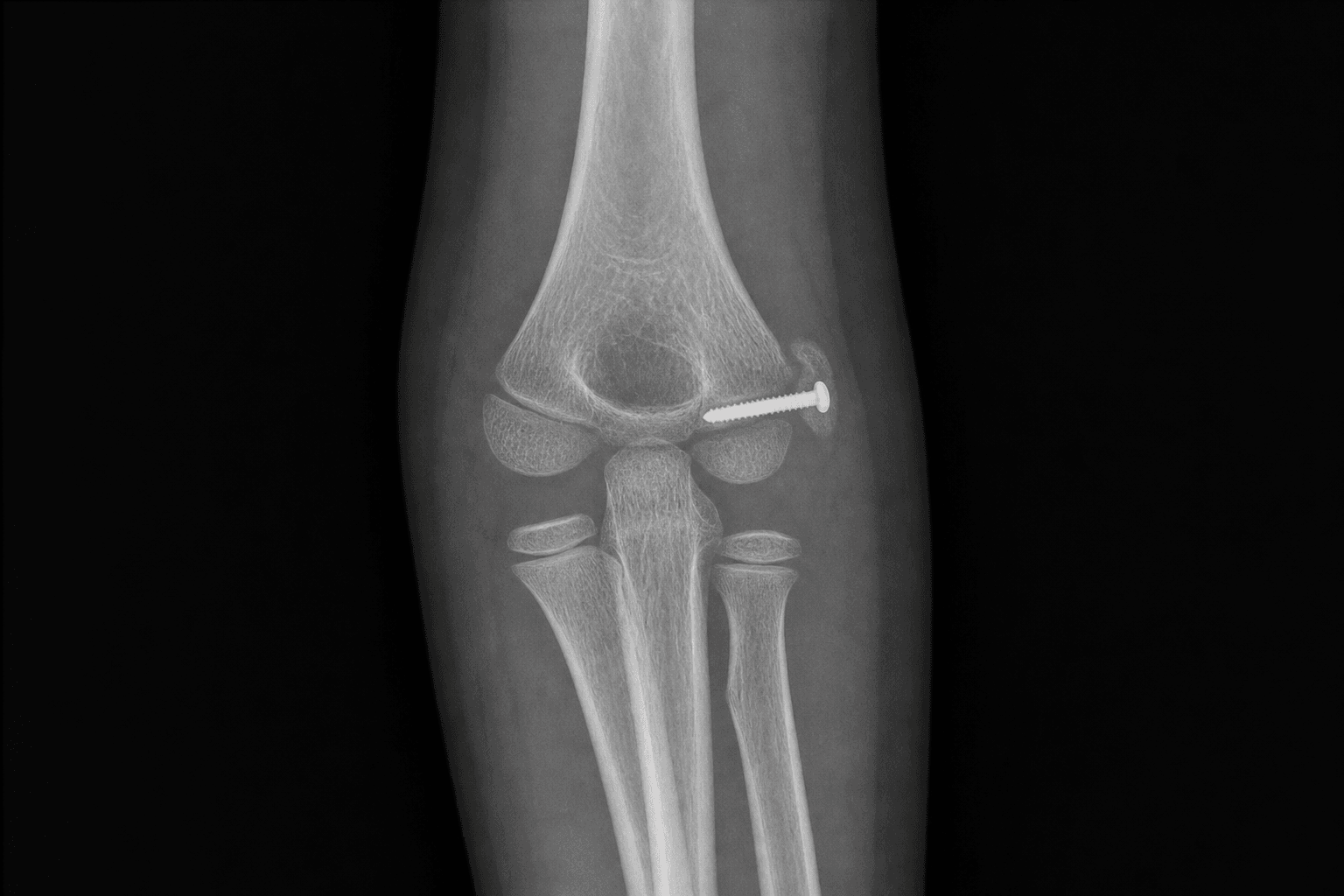
Open reduction and internal fixation of a displaced medial humeral epicondyle apophyseal avulsion · intermediate
- The medial epicondyle is a traction APOPHYSIS for the flexor-pronator mass and the ulnar collateral ligament, not a true epiphysis. It contributes little to longitudinal growth, so growth disturbance is uncommon. It ossifies around 5 to 7 years and fuses to the distal humerus in early adolescence.
- The injury is an AVULSION from acute valgus overload (flexor-pronator and UCL pull) and up to half occur with an elbow dislocation. The fragment can be drawn into the joint (incarcerated), which is an ABSOLUTE indication for ORIF because it will not reduce with a cast and it blocks motion.
- Absolute indications are an incarcerated intra-articular fragment, ulnar nerve dysfunction, and open injury. Displacement alone (the traditional greater-than-5-mm rule) is CONTESTED: the Kamath systematic review found no evidence that fixing a displaced fragment outperforms nonoperative care.
- The ulnar nerve is the key danger structure. It lies posterior to the medial epicondyle in the cubital tunnel, immediately deep to the operative field, and must be identified and protected first throughout the medial approach.
When & Why
Indication. Operative fixation of a paediatric medial epicondyle (apophyseal avulsion) fracture is reserved for the absolute indications below. The commonest error is operating purely for displacement, which the modern evidence does not support. ### Absolute indications
- Incarcerated (intra-articular) fragment that does not reduce after closed reduction of the elbow — the fragment blocks motion and will not unite in a functional position.
- Ulnar nerve dysfunction — especially a nerve incarcerated within the joint or a persistent symptomatic neuropathy.
- Open fracture.
- Vascular injury requiring exploration (rare).
- An irreducible elbow dislocation in which the fragment is interposed and prevents reduction. ### Relative indications (the contested ground)
- Significant displacement — the traditional thresholds of greater than 5 mm, greater than 10 mm, and greater than 15 mm are widely debated and are not supported as standalone indications by modern evidence.
- High-demand overhead-throwing athletes in whom valgus stability is critical to function.
- Objective valgus instability on stress testing, indicating incompetence of the ulnar collateral ligament origin.
- A fragment that lies within the cubital tunnel and irritates the ulnar nerve.
In the overhead-throwing athlete the medial epicondyle carries the origin of the anterior bundle of the ulnar collateral ligament, the prime static restraint to valgus. Keep a lower threshold for anatomic fixation here than in a non-thrower so that UCL tension is restored — an incompletely reduced fragment leaves valgus laxity that is disabling for a pitcher.
Contraindications
Absolute — a fracture without incarceration, nerve compromise, open injury, or demonstrated instability: these do well nonoperatively. Relative — gross swelling or fracture blisters that delay safe surgery, and a near-skeletal-maturity child with a chronic, asymptomatic fibrous nonunion. ## The displacement-threshold controversy Traditional teaching (Smith; Hines) recommended ORIF for displacement greater than 5 mm, with some authors proposing thresholds of greater than 10 mm or greater than 15 mm, citing theoretical risks of nonunion, valgus instability, and ulnar nerve problems. Modern evidence challenges this position: - The Kamath systematic review (2009) found no conclusive evidence that operative treatment of displaced medial epicondyle fractures improves outcome over nonoperative care, and highlighted the lack of high-quality prospective studies.
- Farsetti and colleagues (2001) reported excellent long-term elbow function in patients treated nonoperatively despite residual displacement and frequent fibrous union.
- Josefsson and Danielsson (1986) found that adults reviewed long after childhood nonoperative treatment were largely asymptomatic, even when the fragment had gone on to fibrous union.
- Louahem and colleagues (2010) showed in a multicentre series that long-term outcome was driven by associated elbow injuries and ulnar nerve involvement rather than by the degree of fragment displacement. The defensible modern position is to operate for absolute indications (incarceration, ulnar nerve dysfunction, open injury, instability), to treat the remainder nonoperatively, and to individualise for the high-demand throwing athlete in whom the ulnar collateral ligament origin must be restored. ## Non-operative treatment - A long-arm splint or cast at 90 degrees of flexion for 1 to 3 weeks, followed by early active motion.
- Acceptable for minimally displaced fractures and for displaced fractures that carry no absolute indication.
- Fibrous union is common and is usually asymptomatic; it is not by itself an indication for surgery.
- Counsel the family to expect a minor loss of terminal extension and a small residual cosmetic bump at the medial epicondyle.
Fibrous union of a nonoperatively treated fragment is common and is usually asymptomatic (Farsetti; Josefsson and Danielsson). It is not by itself an indication for surgery — fix only a nonunion that is genuinely symptomatic (pain or instability).
- Operative (ORIF)
- Bony union expected with fixation
- Non-operative
- Often fibrous; usually asymptomatic
- Operative (ORIF)
- Near-complete when early motion is allowed
- Non-operative
- Minor loss of terminal extension is common
- Operative (ORIF)
- Delayed; progressive throwing programme from about 3 months
- Non-operative
- Symptom-guided; often sooner for non-throwers
- Operative (ORIF)
- Restored when the UCL origin is reduced
- Non-operative
- Usually adequate; test throwing athletes specifically
- Operative (ORIF)
- Ulnar nerve, infection, stiffness, hardware
- Non-operative
- Stiffness; asymptomatic nonunion
- Operative (ORIF)
- Incarceration, nerve dysfunction, instability, throwers
- Non-operative
- Most fractures without an absolute indication
Consent specifically for ulnar nerve injury (the commonest nerve problem), stiffness and loss of terminal extension, hardware prominence, infection, and the possibility of an asymptomatic fibrous union if treated nonoperatively. Setup. Supine with the arm on a hand table and the shoulder externally rotated so the medial elbow faces the surgeon (alternatively supine with the arm across the chest over a bolster); a pneumatic upper-arm tourniquet; general anaesthesia with pre-operative antibiotics; and an image intensifier essential throughout.
The Operation
The goal: through the medial (Hotchkiss) approach, identify and protect the ulnar nerve first, expose the fragment still attached to the flexor-pronator mass, reduce it anatomically, and hold it with a single cannulated screw and washer — restoring the ulnar collateral ligament origin. The exposure is laid out in full below, because nerve-safe dissection is the whole game.
Operative sequence
- Supine, arm on a hand table, shoulder externally rotated so the medial elbow faces the surgeon; a well-padded bump helps deliver the elbow.
- Pneumatic upper-arm tourniquet; image intensifier available throughout.
- Palpate and mark the medial epicondyle, the olecranon, and the course of the ulnar nerve behind the medial epicondyle — the incision must give access to both the fragment and the nerve.
- Make a longitudinal or gently curved incision over the medial epicondyle, centred between the medial epicondyle and the olecranon, long enough to expose both the fragment and the ulnar nerve.
Plan the incision so you can comfortably reach the ulnar nerve proximally and the displaced fragment distally. In a throwing athlete or any case with pre-operative ulnar symptoms, make it generous enough to allow anterior transposition of the nerve if it proves necessary.
- Before mobilising the fragment, identify the ulnar nerve proximal to the cubital tunnel and trace it gently distally; protect it with a vessel loop.
- Decompress the roof of the cubital tunnel.
- If there is pre-operative ulnar neuropathy, if the nerve is compressed, or if the fragment was incarcerated near the nerve, perform an anterior subcutaneous transposition.
The nerve can be draped distally over the fragment and is easily injured by a clamp placed blindly. Identifying it first, decompressing the cubital tunnel, and protecting it with a vessel loop converts a hazardous step into a safe one.
Failing to identify the ulnar nerve before fragment mobilisation is the cardinal error — it can lie directly on, or be dragged with, the fragment. Avoid excessive traction on a small-calibre nerve while decompressing the cubital tunnel (use gentle, blunt dissection), and actively explore for a nerve incarcerated within the joint alongside the fragment whenever the pre-operative picture suggests it.
- Follow the flexor-pronator mass distally to the displaced fragment, which remains attached to the mass, and deliver it gently.
- If the fragment is incarcerated within the joint, extract it carefully after protecting the ulnar nerve and the articular cartilage.
- Clear haematoma and early callus from both the fragment and its bed on the distal humerus to allow an anatomic reduction.
- Reduce the fragment onto its bed using a small pointed reduction clamp or a towel clip, seating the cortical margins flush.
- Confirm the reduction on AP and lateral fluoroscopy before placing any fixation.
Residual haematoma or callus is the common cause of a malreduction. Clear the bed meticulously, hold the reduction with a pointed clamp, and confirm it fluoroscopically before any fixation — because the screw will faithfully hold whatever reduction you give it.
- Place a guide wire from the fragment across the distal humerus toward the lateral column, aiming for the capitellar or lateral cortex while avoiding the olecranon fossa (a screw here blocks extension) and the joint surface.
- Confirm wire position, trajectory, and length on fluoroscopy and measure.
- Drill and place a partially threaded cannulated cancellous screw (commonly 4.0 mm or 4.5 mm) with a washer; engage the far (lateral) cortex for purchase without over-penetrating it.
- Avoid over-compression that could comminute the fragment, and avoid multiple drill passes.
Aim the guidewire toward the lateral column and stop short of the far cortex, then check the lateral view carefully — the screw must not sit in the olecranon fossa or the joint. The washer matters: the paediatric fragment is soft cancellous bone, and a screw head alone can sink and lose reduction.
A screw or wire breaching the olecranon fossa or the joint causes a block to extension and cartilage damage. Over-compression can comminute a small fragment — use a washer and stop once the fragment is seated. Multiple drill passes weaken the fragment, so plan the wire, confirm it, then drill once. Finally, check the ulnar nerve is clear and not subluxing over the washer after fixation.
- Through a full arc of flexion-extension and pronation-supination, confirm the fragment is stable and the elbow extends fully with no bony block.
- Confirm the ulnar nerve is neither compressed nor subluxing over the hardware.
- Take final fluoroscopic images to confirm reduction and hardware position.
- Irrigate, achieve haemostasis, and close in layers over the ulnar nerve.
- If the ulnar nerve was transposed, close the cubital tunnel fascia appropriately so the nerve sits in a stable anterior position.
- Apply a long-arm splint or cast at 90 degrees of flexion with the forearm in neutral for 3 to 4 weeks.
Fixation alternatives For very small or comminuted fragments, use K-wires with a tension band, or suture fixation of the flexor-pronator origin to the distal humerus.
Avoid smooth K-wires across the medial epicondyle as definitive fixation in older children unless protected, because of pin-site problems and loss of fixation. The cannulated screw is preferred whenever the fragment will accept it.
Variations for special situations Incarcerated fragment. After reducing any elbow dislocation, recognise the fragment trapped within the joint using the CRITOE order and a true lateral film. Extract it carefully while protecting the ulnar nerve and the articular cartilage, fix it anatomically, and explore the ulnar nerve, which may be symptomatic or incarcerated alongside the fragment. Ulnar nerve management. Document nerve status pre-operatively. Intra-operatively, decompress the cubital tunnel and transpose the nerve anteriorly (subcutaneous) when there is pre-operative neuropathy, severe compression, or incarceration. Confirm after fixation that the nerve does not sublux over the screw or washer. Overhead-throwing athlete. An acute displaced fracture in a thrower deserves a lower threshold for anatomic fixation to restore the UCL origin. Counsel on a delayed return to throwing and on age-appropriate pitching-load limits (rest days and pitch counts). Elbow dislocation. Reduce the dislocation first, then reassess the fragment and the neurovascular status. Fix the fragment if it is incarcerated or unstable, and use a brief period of protected motion to limit the stiffness that follows a paediatric elbow dislocation.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Activity | |-------|--------|----------------|----------| | 1 | 0 to 4 weeks | Long-arm splint or cast at 90 degrees, forearm neutral | Elevation and simple analgesia; finger active motion; radiographs at 1 to 2 weeks | | 2 | 4 to 6 weeks | Removable splint; avoid valgus stress | Begin active then active-assisted elbow range of motion | | 3 | 6 to 8 weeks | Splint for heavy tasks only | Progressive motion and light strengthening once union is advancing | | 4 | 8 to 16 weeks | Night splint only if needed | Non-contact sport from 8 to 12 weeks; progressive throwing from about 3 months | Avoid valgus stress for the first 6 weeks to protect the UCL origin. Non-contact activities resume from around 8 to 12 weeks once motion and strength are full and pain-free. Overhead throwing is delayed: a progressive throwing programme typically begins no earlier than 3 months, with full competitive pitching often at 4 to 6 months. Complications
- Recognition
- Numbness or paraesthesia in the ulnar one and a half digits; intrinsic weakness; cold intolerance
- Prevention
- Identify and protect the nerve first; decompress the cubital tunnel; keep hardware clear of the nerve
- Management
- Observe for a neurapraxia; explore promptly if a complete and persistent deficit is present
- Recognition
- Loss of terminal extension; a flexion contracture; reduced pronation-supination
- Prevention
- Stable fixation that allows early motion; brief immobilisation
- Management
- Physiotherapy; static-progressive splinting for a developing contracture
- Recognition
- Progressive stiffness with a palpable or calcified mass about the elbow
- Prevention
- Early motion; avoid repetitive soft-tissue trauma
- Management
- Prophylaxis in high-risk head-injured patients; excision once mature if functionally limiting
- Recognition
- Valgus laxity on stress testing; pain or collapse of function with throwing
- Prevention
- Anatomic reduction and rigid fixation restoring the UCL origin
- Management
- Structured rehabilitation; reconstruct the UCL if chronically incompetent in a high-demand thrower
- Recognition
- Persistent radiographic lucency at the fragment base without symptoms
- Prevention
- Reassure if asymptomatic
- Management
- Consider fixation only if the nonunion is symptomatic (pain or instability)
- Recognition
- Loss of reduction on radiographs; local irritation over the hardware
- Prevention
- A screw of adequate length engaging the far cortex with a washer; protected immobilisation
- Management
- Revise fixation if the fragment is displaced
- Recognition
- Erythema, swelling, warmth, or discharge; systemic features
- Prevention
- Aseptic technique and perioperative antibiotics
- Management
- Wound swab and oral antibiotics; surgical washout if deep
- Recognition
- Change in the carrying angle; a medial prominence
- Prevention
- Growth disturbance is rare because the medial epicondyle is an apophysis
- Management
- Counsel on a small residual bump; correct only a significant angular deformity
- Recognition
- Persistent blocked motion; a fragment visible within the joint
- Prevention
- Recognise with the CRITOE order and a true lateral film
- Management
- Extract the fragment and fix it anatomically, with nerve protection
Viva & Exam Focus
MEDIALThe fracture at a glance
OPERASWhen to operate
Trap — after an elbow dislocation the medial epicondyle can be drawn into the joint; on the AP film it sits near the trochlear region and is mistaken for the trochlear ossification centre or a normal variant. Fix — use the CRITOE order: the medial epicondyle ossifies before the trochlea, so a trochlea that appears too early, or a medial epicondyle absent from its normal position, is the incarcerated fragment. An incarcerated fragment is an absolute indication for ORIF; confirm with a true lateral and a CT if doubt remains, then extract and fix it.
Location — the ulnar nerve lies posterior to the medial epicondyle in the cubital tunnel, immediately deep to the surgical field; it can be dragged distally with the fragment or, rarely, incarcerated within the joint alongside it. Risk — direct injury during dissection, traction, or post-operative compression over hardware; pre-injury ulnar symptoms are common with this fracture. Protection — identify it first, protect it with a vessel loop, decompress the cubital tunnel, and consider anterior transposition when there is pre-operative neuropathy or the fragment was incarcerated.
Trap — applying the traditional greater-than-5-millimetre displacement rule as an absolute indication to operate. Fix — displacement alone is contested. The Kamath systematic review found no evidence that ORIF of a displaced fragment improves outcome over nonoperative care, and Farsetti and Josefsson showed good long-term function with fibrous union. Operate for incarceration, nerve dysfunction, or instability, not for displacement alone.
Trap — apparent fragment position is unreliable when the elbow is splinted in flexion, and the fragment may be confused with the trochlea, the lateral condyle, or a normal ossification centre. Fix — obtain true AP and lateral views (and a comparison view of the opposite elbow in subtle cases). Actively exclude an associated elbow dislocation and a lateral condyle fracture, confirm the radiocapitellar line, and use the CRITOE order to locate the medial epicondyle.
Why it matters — the medial epicondyle bears the ulnar collateral ligament origin, so an incompletely restored fragment leaves valgus laxity that is disabling for an overhead thrower. Fix — in high-demand throwing athletes keep a lower threshold for anatomic reduction and rigid fixation to restore UCL tension, and counsel on a delayed, progressive return to throwing.
Trap — the paediatric elbow stiffens readily after this injury, especially when associated with a dislocation, and prolonged immobilisation compounds the loss of motion. Fix — use stable fixation that allows early motion, immobilise briefly, and begin guided range-of-motion exercises; watch for heterotopic ossification, the risk of which rises with a concomitant elbow dislocation or a head injury.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 12-year-old boy fell onto his outstretched hand. Radiographs show a medial epicondyle fracture with the fragment displaced approximately 8 mm but lying outside the joint, no elbow dislocation, and a normal ulnar nerve examination. How do you manage him?”
“A 13-year-old presents after an elbow dislocation that has been reduced in the emergency department. The post-reduction AP radiograph shows what appears to be a trochlear ossification centre, but the medial epicondyle is not visible in its normal position. The child has ulnar-distribution paraesthesia. What is going on and how do you manage it?”
“You are fixing a displaced medial epicondyle fracture in a 14-year-old elite junior baseball pitcher. What specific considerations apply, and how do your fixation and rehabilitation differ from those of a non-throwing child?”
Key diagnosis points
- The medial epicondyle is an APOPHYSIS (not a true epiphysis) — growth disturbance is rare
- Mechanism: acute valgus avulsion by the flexor-pronator mass and UCL; up to half occur with elbow dislocation
- Incarceration trap: the fragment mimics the trochlear ossification centre — use the CRITOE order (medial epicondyle ossifies before the trochlea)
- Wilkins classification: Stage 1 minimally displaced; Stage 2 displaced extracapsular; Stage 3 incarcerated with elbow reduced; Stage 4 incarcerated with elbow dislocated
- Document ulnar nerve and brachial artery status before and after any reduction
Surgical anatomy
- Flexor-pronator mass (pronator teres, FCR, PL, FCU, FDS) originates from the medial epicondyle
- The ulnar collateral ligament anterior bundle originates here — the priority in a throwing athlete
- The ulnar nerve lies posterior to the medial epicondyle in the cubital tunnel — the key danger structure
- CRITOE: Capitellum, Radial head, Internal (medial) epicondyle, Trochlea, Olecranon, External (lateral) epicondyle
- Ossifies at 5 to 7 years; fuses to the distal humerus at 13 to 15 years
Indications
- ABSOLUTE: incarcerated intra-articular fragment, ulnar nerve dysfunction, open fracture, vascular injury, irreducible dislocation with interposed fragment
- RELATIVE: significant displacement (contested), high-demand throwing athletes, objective valgus instability, fragment irritating the ulnar nerve
- Displacement alone (the traditional greater-than-5-mm rule) is NOT an evidence-backed standalone indication
- Nonoperative care: long-arm splint at 90 degrees for 1 to 3 weeks then early motion — good outcomes even with fibrous union
- Stages 3 and 4 (incarceration) always require surgery; Stage 4 also needs urgent reduction of the dislocation
Operative technique — key steps
- 1. Supine, arm on a hand table, shoulder externally rotated; pneumatic tourniquet; image intensifier essential
- 2. Longitudinal incision between the medial epicondyle and the olecranon
- 3. Identify and protect the ulnar nerve FIRST; decompress the cubital tunnel; transpose anteriorly if symptomatic
- 4. Expose the fragment (still attached to the flexor-pronator mass); extract it carefully if incarcerated
- 5. Clear haematoma and callus; reduce anatomically and confirm on AP and lateral fluoroscopy
- 6. Guide wire toward the lateral column; cannulated cancellous screw with a washer; engage the far cortex without breaching the olecranon fossa or the joint
- 7. Verify full motion with no block to extension and a clear ulnar nerve
- 8. Splint at 90 degrees for 3 to 4 weeks
Danger zones
- The ulnar nerve in the cubital tunnel — identify and protect it before fragment mobilisation
- The olecranon fossa and the joint surface — a screw here blocks extension and damages cartilage
- The opposite (lateral) cortex and posterior structures — over-penetration risks neurovascular injury
- The incarceration imaging trap — a trochlear centre that appears too early is the trapped medial epicondyle
- The flexor-pronator/UCL attachment — a malreduction leaves the UCL origin under wrong tension
Complications
- Ulnar nerve injury or neuropathy — the most common nerve problem; identify and protect the nerve; transpose when symptomatic
- Loss of terminal extension and stiffness — common, especially with a dislocation; stable fixation and early motion limit it
- Heterotopic ossification — uncommon; higher with a dislocation or a head injury
- Valgus instability — relevant in throwers; restore the UCL origin anatomically
- Fibrous nonunion — common after nonoperative care and usually asymptomatic; fix only if symptomatic
Special cases
- Incarcerated fragment: recognise with CRITOE and a true lateral; extract and fix; explore the ulnar nerve
- Ulnar nerve: decompress; transpose anteriorly (subcutaneous) for pre-operative neuropathy, severe compression, or incarceration
- Throwing athlete: lower threshold for anatomic ORIF; protect from valgus for 6 weeks; progressive throwing from about 3 months; full pitching at 4 to 6 months
- Elbow dislocation: reduce first, reassess, fix if incarcerated or unstable; use protected motion to limit stiffness
- Chronic apophysitis (little league elbow): rest and a structured throwing programme; reserve fixation for acute displaced fractures
Background & Evidence
The medial epicondyle — an apophysis. The medial epicondyle is a traction APOPHYSIS on the posteromedial distal humerus, not a true epiphysis. It contributes little to longitudinal growth, so growth disturbance is uncommon after injury or fixation. It ossifies around 5 to 7 years of age (girls earlier than boys) and fuses to the distal humeral metaphysis around 13 to 15 years. CRITOE — the order of ossification of the elbow. Capitellum, Radial head, Internal (medial) epicondyle, Trochlea, Olecranon, External (lateral) epicondyle. The medial epicondyle ossifies BEFORE the trochlea — the anatomical basis of the incarceration imaging trap.
An entrapped fragment on the AP film can mimic the trochlear ossification centre, but the medial epicondyle ossifies before the trochlea (CRITOE). So an apparent trochlea in the wrong place, or appearing too early, with the medial epicondyle absent from its normal position, is the trapped medial epicondyle — an absolute indication for ORIF.
Do not confuse the medial epicondyle (an apophyseal avulsion) with the lateral condyle (a true Salter-Harris IV epiphyseal injury that demands anatomic reduction) or a supracondylar fracture — they are distinct injuries with different management.
Musculoligamentous attachments. The flexor-pronator mass origin (pronator teres, flexor carpi radialis, palmaris longus, flexor carpi ulnaris, and flexor digitorum superficialis) and the ulnar collateral ligament origin (the anterior bundle is the prime static restraint to valgus) both arise from the medial epicondyle. The avulsion occurs because acute valgus stress tensions the flexor-pronator mass and the UCL, levering the apophysis off the distal humerus. The ulnar nerve. The ulnar nerve courses posterior to the medial epicondyle through the cubital tunnel, immediately deep to the operative field. It may be displaced distally with the fragment or, rarely, incarcerated within the joint alongside it. Pre-injury ulnar nerve symptoms occur in a substantial minority of these fractures, so the nerve must always be identified and protected. Associated injuries to exclude. Elbow dislocation (common — assess and reduce first), a lateral condyle fracture (do not miss, as it requires its own management), a radial neck fracture, an olecranon fracture, and an extension-type supracondylar fracture. Document the ulnar nerve and the vascular (brachial artery) status before and after any reduction.
- Description
- Minimally displaced
- Operative?
- No — nonoperative
- Description
- Displaced, extracapsular, elbow reduced
- Operative?
- No — nonoperative (contested if high displacement)
- Description
- Fragment incarcerated in the joint, elbow spontaneously reduced
- Operative?
- Yes — absolute indication
- Description
- Fragment incarcerated in the joint, elbow still dislocated
- Operative?
- Yes — urgent reduction plus fixation
- Description
- Repetitive valgus overload — little league elbow apophysitis
- Operative?
- No — rest and a structured throwing programme
Key evidence — the displacement controversy. The consistent message across four decades of study is that operating purely for displacement is not supported. Kamath (2009), in a systematic review, found no conclusive evidence that operative treatment improves outcome over nonoperative care. Farsetti (2001) reported excellent long-term elbow function despite residual displacement and frequent fibrous union, and Josefsson and Danielsson (1986) confirmed that adults reviewed long after childhood nonoperative treatment were largely asymptomatic. Louahem (2010) showed that long-term outcome was driven by associated elbow injuries and ulnar nerve involvement rather than by displacement. Hines (1987) anchored the traditional operative approach with reliable ORIF results, but the displacement thresholds that work informed are now applied more selectively — operate for incarceration, nerve dysfunction, open injury, or instability.
References
Operative versus non-operative management of pediatric medial epicondyle fractures: a systematic review.
- Systematic review of the management of displaced medial epicondyle fractures of the humerus in children
- Found no conclusive evidence that operative treatment improves outcome over nonoperative care
- Highlighted the lack of high-quality prospective studies to settle the displacement-threshold controversy
Long-term results of treatment of fractures of the medial humeral epicondyle in children.
- Long-term follow-up of medial epicondyle fractures in children managed without internal fixation
- Reported good elbow function despite residual displacement and frequent fibrous union
- Supported nonoperative management when an absolute operative indication was absent
Epicondylar elbow fracture in children. 35-year follow-up of 56 unreduced cases.
- Adults reviewed long after childhood medial epicondyle fractures treated nonoperatively
- Demonstrated that displaced and even fibrously united fragments were generally well tolerated clinically
- Reinforced that residual displacement is compatible with good long-term function
Operative treatment of Medial epicondyle fractures in children.
- Reported reliable results with open reduction and internal fixation of medial epicondyle fractures in children
- Supported operative fixation for substantially displaced fragments
- Anchored the traditional operative approach that later evidence has since tempered