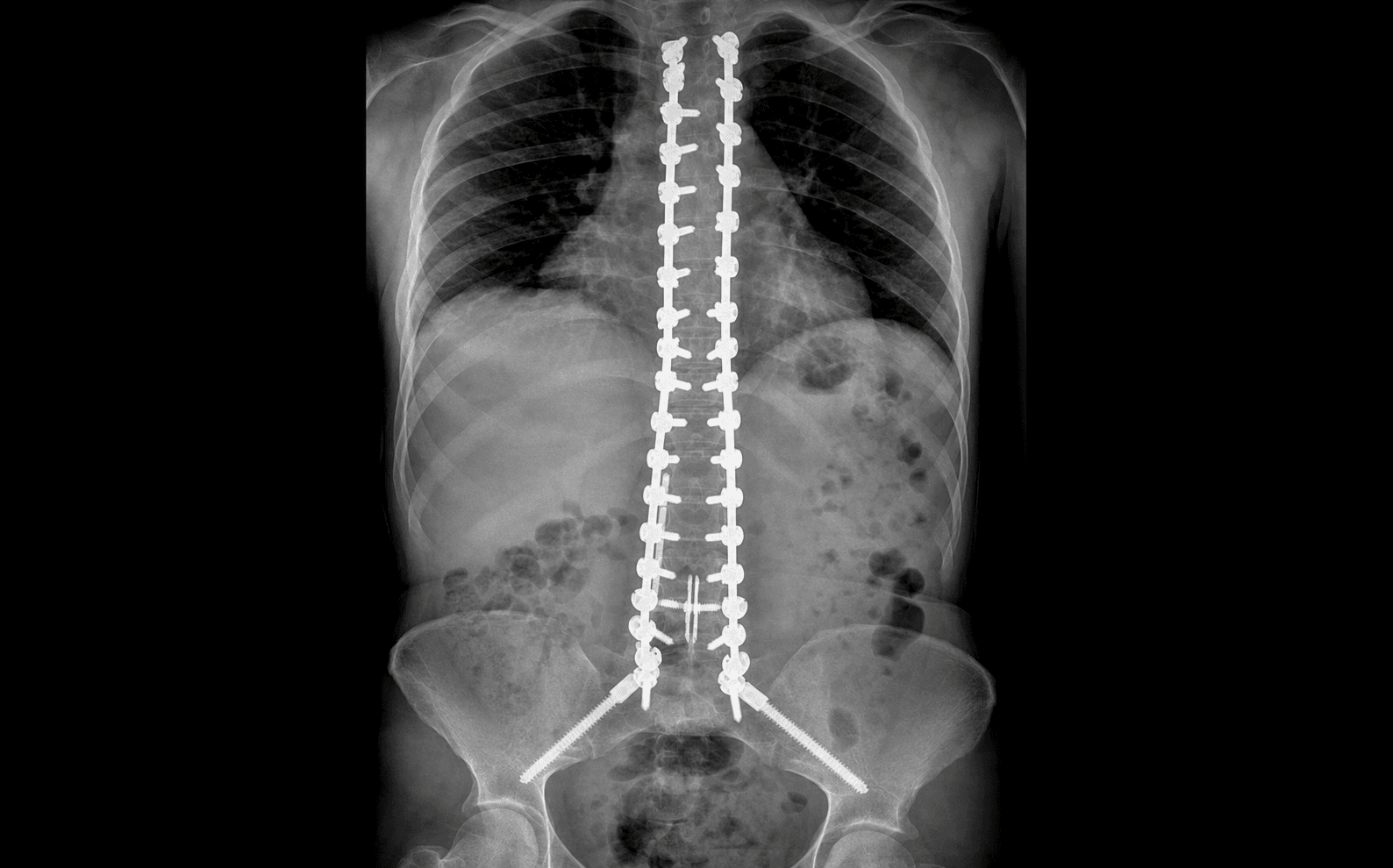
Posterior midline instrumentation from the upper thoracic spine (T2/T3) to the pelvis (S1 + bilateral iliac screws) for progressive neuromuscular scoliosis in Duchenne/Becker muscular dystrophy · advanced
- Progressive neuromuscular scoliosis in Duchenne or Becker muscular dystrophy (DMD/BMD) with a curve greater than 20–30 degrees that is progressing despite bracing.
- Goals: prevent curve progression, restore sitting balance, correct pelvic obliquity, ease nursing care and reduce pain. Surgery does NOT halt the FVC decline — that tracks progressive muscle weakness, not the curve (a high-yield exam point).
- Operate in the sweet spot: curve 30–50 degrees, FVC greater than 40 percent predicted, EF greater than 30 percent, while the patient still has reasonable quality of life.
- Pedicle screws at EVERY level (osteoporotic bone — no skipped levels), T2/T3 to pelvis, with MANDATORY pelvic fixation (bilateral iliac + S1 screws).
- Glucocorticoids have markedly reduced scoliosis incidence and severity — steroid-treated boys present later and fewer need fusion.
When & Why
Indication. Progressive neuromuscular scoliosis in Duchenne or Becker muscular dystrophy — a curve greater than 20–30 degrees that is documented to be progressing despite bracing — in a patient who still has adequate pulmonary function (FVC greater than 30–40 percent predicted) and adequate cardiac function (EF greater than 30 percent), and who retains a reasonable quality of life. Curves that have not progressed, and patients in whom cardiopulmonary reserve has already collapsed, are not served by surgery. Goals of surgery. Prevent curve progression, restore and maintain sitting balance, correct pelvic obliquity, ease nursing care and seating, and reduce back pain. Counsel families honestly that fusion does not halt the FVC decline — that tracks progressive muscle weakness, not the curve (Shapiro et al.). The indication is seating, comfort and deformity prevention, not respiratory preservation. Timing — the one decision that matters. Too early is unnecessary surgery; too late is prohibitive risk. The window balances four variables:
Curve less than 20 degrees, FVC greater than 60 percent. Unnecessary surgery — small curves may be watched or braced, and the relentless progression is not yet established.
Curve 30–50 degrees, FVC 40–60 percent, EF greater than 30 percent, reasonable quality of life. Operate here, before pelvic obliquity sets in and reserve collapses.
Curve greater than 70–80 degrees, FVC less than 30 percent, EF less than 25 percent. Prohibitive respiratory and cardiac risk — the operation is now more dangerous than the disease.
Pre-operative optimisation. Every DMD fusion is a multidisciplinary case. The cardiopulmonary work-up is the rate-limiting step and a perennial viva topic:
CARDIACCARDIAC — the pre-operative checklist
Consent specifically for the major risks: respiratory failure (20–30 percent), blood loss requiring transfusion (greater than 50 percent), infection (5–10 percent), neurologic deficit (1–3 percent), pseudarthrosis (10–20 percent), proximal junctional kyphosis (10–20 percent), dural tear (5–10 percent), and the honest statement that the operation will not preserve lung function. Setup. Prone on a Jackson table or chest rolls with the abdomen hanging free (reduces venous bleeding). Lines: arterial line for tight BP control and anticipated blood loss, Foley, core temperature, and neuromonitoring leads. Regional or neuraxial techniques are generally avoided; this is a general-anaesthetic, ICU-bound case.
The Operation
The goal is a rigid, segmentally instrumented posterior fusion from T2/T3 to the pelvis that corrects the coronal curve and pelvic obliquity while protecting the spinal cord, nerve roots, great vessels and iliac vessels. The exposure is the long posterior midline subperiosteal dissection, laid out in full as the first steps below.
Operative sequence
- Prone on a Jackson table or chest rolls; arms alongside the body or on boards at less than 90 degrees abduction (shoulder contractures); head neutral or slight extension — avoid excessive flexion (airway compromise).
- Abdomen hangs free — reduces IVC compression and venous engorgement, which directly reduces epidural bleeding.
- Meticulous padding of forehead (avoid globe pressure), chest and osteoporotic ribs (fracture risk), iliac crests (high pressure), knees, anterior shins and elbows. DMD skin is fragile and the case is long (5–8 hours).
- Monitoring: neuromonitoring (SSEP/MEP — note MEPs are often poor or absent at baseline in DMD), arterial line, Foley, core temperature.
- Posterior midline incision from the T2 spinous process to the sacrum/upper buttock (40–50 cm).
- Incise skin, subcutaneous tissue (fatty in DMD, with minimal muscle) and the posterior fascia.
- Plan the subcutaneous layer as the main strength layer — muscle atrophy limits fascial closure at the end.
- With a Cobb elevator, strip the paraspinal muscles off the spinous processes, laminae and transverse processes bilaterally.
- Expose the entire posterior elements: spinous processes, laminae, facets, transverse processes and pars.
- At the pelvis, expose the sacrum and the posterior iliac wings bilaterally to receive the iliac screws.
- Place self-retaining retractors (Taylor, Schofield).
- Haemostasis throughout: thrombin-soaked sponges, bipolar cautery and bone wax. Osteoporotic bone and fatty tissue bleed readily — inadequate haemostasis now is the source of large blood loss later.
- Entry point: junction of the transverse process and superior articular process, 2–3 mm lateral to the facet.
- Thoracic pedicles are small (4–6 mm) and angulated medially; create the pilot hole with a high-speed burr.
- Trajectory converges 10–15 degrees medially, toward the vertebral body centre; probe all four walls with a ball-tip probe before insertion (medial wall breach equals cord injury).
- Insert polyaxial screws (4.5–5.5 mm diameter, 35–45 mm length). Screws go at EVERY level — no skipped levels in osteoporotic DMD bone. T2–T4 pedicles are the smallest and carry the highest malposition risk.
- Entry point: junction of the transverse process and superior facet, slightly more lateral than thoracic.
- Lumbar pedicles are larger (8–15 mm); trajectory converges 10–15 degrees medially.
- L5 screws need a steep caudal trajectory (45–50 degrees) toward the sacral promontory; confirm with lateral fluoroscopy (the screw should parallel the superior endplate).
- Entry: the S1 lateral mass (junction of the facet and ala).
- Trajectory anterior and lateral toward the promontory; large screws (7.5–8.5 mm, 45–55 mm); aim for bicortical purchase.
- Classic iliac screws: entry at the PSIS or 1–2 cm caudal; trajectory from PSIS toward the AIIS, running between the inner and outer iliac tables; long screws (7.5–9.5 mm diameter, 70–100 mm length), placed bilaterally. Fluoroscopy confirms the trajectory (parallel to the iliac crest on AP, caudal on lateral). Offset connectors link the iliac screws to the main rods.
- S2-alar-iliac (S2AI) screws — the modern alternative: entry 1 cm caudal and lateral to the S1 foramen, crossing the SI joint into the ilium. The start point is more medial and in-line (no offset connector needed), the screw head sits deeper (less prominence and skin breakdown), and removal rates are lower. Now widely preferred over Galveston and iliac-bolt techniques in many global centres; both achieve the goal of rigid pelvic fixation.
- Stiff neuromuscular curves (essentially all DMD cases) need release to correct.
- Complete facetectomies — remove the inferior and superior articular processes at 4–6 apical levels — to unlock the curve.
- Resect the ligamentum flavum at the release levels; preserve the dura and control epidural bleeding with bipolar and thrombin-soaked Gelfoam.
- A Smith-Petersen osteotomy (a V-shaped posterior opening that hinges on the anterior disc) is usually sufficient. Avoid PSO and VCR — too much cord-stretch risk and unnecessary in neuromuscular curves.
- 5.5–6.0 mm cobalt-chrome (stiffer, better for long constructs) or titanium (lighter, MRI-compatible).
- Pre-contour to thoracic kyphosis 35–45 degrees and lumbar lordosis 40–50 degrees; use gradual bends (sharp angles are stress-risers) and contour for the entire construct, T2 to pelvis.
- Insert the concave rod first; thread it into the screw heads using the reduction tabs and provisionally tighten the set screws; insert the convex rod similarly.
- Cantilever correction: apply force to the rod and reduce the screws progressively.
- Compression on the convex side, distraction on the concave side; derotation to correct the rib hump; translation of the apical vertebrae toward the midline.
- Goals: coronal curve reduced to less than 20–30 degrees (perfect correction is not required), sagittal balance restored, lumbar lordosis maintained, sitting balance preserved.
- Continuous SSEP/MEP monitoring — any change mandates STOP. Over-correction risks flat back and junctional kyphosis; osteoporotic bone risks screw pullout.
- Decorticate the laminae, facet joints (after facetectomies), transverse processes, pars, sacral ala and posterior iliac wings with a high-speed burr down to bleeding cancellous bone; irrigate while burring to avoid thermal injury to the dura and cord. DMD bone is osteoporotic — maximal surface area is needed for fusion.
- Autograft is limited (minimal local bone from spinous processes/facets), so morselised cancellous allograft is the PRIMARY graft source; DBM and synthetic substitutes (calcium phosphate, hydroxyapatite) supplement it. BMP is controversial (off-label in the spine; seroma, ectopic bone) but is considered in poor-quality bone. Pack graft generously over the whole decorticated bed.
- Torque-limiting driver (80–120 in-lbs); tighten cranial to caudal, bilateral, and confirm all screws are secure.
- Apply two to three transverse cross-links (proximal thoracic, mid-thoracic, lumbosacral) for rotational stability and to prevent rod migration.
- Offset connectors link the iliac screws to the main rods (the iliac screws sit lateral to the rod trajectory).
- Haemostasis: bipolar for soft tissue, bone wax for bone, thrombin-soaked Gelfoam and Floseal, and copious antibiotic irrigation.
- Two to four large-bore Jackson-Pratt drains (high output is expected — they reduce haematoma).
- Closure: thoracolumbar fascia if there is adequate tissue (often minimal in DMD); the subcutaneous layer (0 or 2-0 Vicryl) is the main strength layer; running absorbable subcuticular or interrupted nylon for skin; consider a VAC dressing if wound tension is high.
Iliac screw medial breach perforates the inner table and strikes the iliac artery and vein — catastrophic bleeding. Aim the trajectory anteriorly (PSIS toward AIIS), not medially. The superior gluteal artery exits the greater sciatic notch 2–3 cm from the PSIS and is injured if the trajectory is too posterior. An S1 anterior breach threatens the presacral vessels. Inadequate pelvic fixation leads to pseudarthrosis and sacral screw pullout.
Neurologic injury comes from cord ischaemia due to stretch or distraction. Monitor SSEP and MEP continuously during correction; any change mandates STOP, release the correction, and maintain MAP greater than 85 mmHg. If signals do not recover, further release the construct and consider a wake-up test. It is better to undercorrect than to cause a paraplegia — DMD patients care more about sitting balance than cosmesis.
Check the abdomen hangs free — this alone meaningfully reduces venous engorgement and epidural bleeding across a 5–8 hour case. DMD patients have fragile skin (pressure ulcer risk), osteoporotic ribs (fracture risk) and contractures (limited ROM), so meticulous padding is non-negotiable.
The iliac screw trajectory is anterior (PSIS toward AIIS), between the iliac tables — never medial (iliac vessels) and never posterior (superior gluteal artery at the sciatic notch). Fluoroscopy confirms the line in both planes. Countersink the start hole to reduce posterior prominence and skin breakdown.
Average loss is 1–3 litres and more than half of patients need transfusion. Crossmatch 4–6 units, use a cell saver, maintain controlled hypotension (MAP 65–75 mmHg during exposure, then raise MAP greater than 85 mmHg for correction), maintain normothermia, and correct any coagulopathy promptly.
Aftercare & Complications
ICU management (all DMD patients). Every DMD fusion goes to ICU for 1–3 days minimum, longer if respiratory support is needed. Most discharge by 5–10 days if uncomplicated; complications occur in 20–40 percent of cases. - Respiratory (highest priority): overnight ventilation is often needed; extubate when the patient is awake with a strong cough and good tidal volumes; use BiPAP if marginal; aggressive pulmonary toilet with incentive spirometry, chest PT and frequent suctioning; early mobilisation (sit day 1–2).
- Pain: multimodal — PCA opioids, gabapentin, acetaminophen; consider epidural or intrathecal morphine.
- Cardiac: continuous telemetry (cardiomyopathy risk) with arrhythmia surveillance.
- Neurologic: frequent exams every 2–4 hours initially; check motor and sensory in all extremities; watch for delayed deficit from epidural haematoma.
- Drains: remove when output is less than 30 mL per 8 hours (typically day 3–5).
- Mobilisation: sit day 1–2; transfer to wheelchair day 2–3 (most DMD patients are wheelchair-dependent); no brace is needed — the instrumented fusion is stable.
- Imaging: AP/lateral spine X-rays on day 1 to confirm instrumentation and alignment, then at discharge, 6 weeks, 3 months, 6 months, 1 year, then yearly until skeletal maturity and every 1–2 years after. Long-term monitoring. Watch for infection (fever, wound drainage, rising CRP/ESR), pseudarthrosis (pain, loss of correction, nonunion on X-ray/CT), instrumentation failure (screw pullout, rod fracture) and proximal junctional kyphosis. The functional goals are improved sitting balance and corrected pelvic obliquity, easier seating/transfers/nursing care, reduced back pain, and preserved quality of life — with the explicit caveat that FVC continues to decline with disease progression (Shapiro et al.). Complications
- Recognition
- Hypoxia, hypercarbia, poor tidal volumes, inability to clear secretions, declining mental status
- Prevention
- Pre-op optimisation (FVC greater than 40%), aggressive pulmonary toilet, incentive spirometry, BiPAP, early mobilisation, multimodal analgesia to cut opioids
- Management
- Reintubation if needed, mechanical ventilation, bronchoscopy for mucus plugging, chest PT, treat pneumonia, prolonged ICU stay
- Recognition
- Intra-op loss greater than 1–3 L, hypotension, tachycardia, falling haemoglobin
- Prevention
- Meticulous haemostasis (bipolar, bone wax, Gelfoam), thrombin agents, cell saver, controlled hypotension (MAP 65–75), normothermia, correct coagulopathy
- Management
- PRBC transfusion (4–6 units crossmatched), FFP/platelets if coagulopathic, identify the bleeding source, consider a staged procedure if loss is massive
- Recognition
- SSEP/MEP change intra-op, post-op weakness/numbness, dermatomal deficit, bowel/bladder dysfunction
- Prevention
- Neuromonitoring (SSEP/MEP), gradual correction, avoid over-correction, maintain MAP greater than 85 mmHg, wake-up test if SSEPs change, probe all pedicle screws
- Management
- If intra-op change: STOP, release correction, optimise BP, wait for recovery. Post-op deficit: urgent MRI, surgical decompression if compressive, steroids controversial
- Recognition
- Fever, wound erythema/drainage, raised WBC/CRP/ESR, pain, fluid on imaging, positive cultures
- Prevention
- Pre-op antibiotics (cefazolin 2 g, or vancomycin if MRSA risk), re-dose every 4 h intra-op, normothermia, minimise dead space, drains, meticulous closure
- Management
- Superficial: oral antibiotics and local wound care. Deep: washout and debridement, retain implants if stable, 6 weeks IV antibiotics guided by cultures, suppressive antibiotics if cannot clear
- Recognition
- Persistent pain, loss of correction on serial X-rays, visible gap at the fusion site, motion on flexion/extension films, CT-confirmed nonunion
- Prevention
- Adequate decortication, generous bone graft (allograft plus consider BMP), rigid fixation (screws all levels, pelvic fixation), no smoking, optimise nutrition
- Management
- If asymptomatic with stable implants: observe. If symptomatic or implant failure: revision surgery (remove failed screws, extend fusion if needed, additional graft plus or minus BMP, new instrumentation)
- Recognition
- Increasing kyphosis above the cranial end of the fusion (greater than 10 degrees or greater than 10 degrees more than pre-op), pain, cosmetic deformity
- Prevention
- Avoid over-correction, gradual transition at the upper instrumented vertebra, consider UIV at T2–T4, avoid over-distraction, taper rod diameter
- Management
- If mild and asymptomatic: observe. If severe (greater than 20 degrees), painful or progressive: extend fusion cranially (add 2–3 levels), may need osteotomy at the PJK apex
- Recognition
- CSF leak intra-op (clear fluid), post-op CSF drainage from the wound, positional headache, meningismus
- Prevention
- Gentle dissection (osteoporotic laminae fracture easily), careful osteotomy technique, avoid aggressive retraction, probe pedicles to avoid medial breach
- Management
- Intra-op: primary repair (5-0 or 6-0 Prolene), watertight closure, fibrin glue, Gelfoam overlay, Valsalva test. Post-op leak: bedrest, pressure dressing, lumbar drain if persistent, surgical repair if conservative fails
Viva & Exam Focus
SOLIDSOLID — pelvic fixation requirements
Location: posterior in the spinal canal, 2–3 mm anterior to the lamina. Protection: avoid laminar violation during dissection, confirm every pedicle screw is extra-canal by probing all four walls, and monitor SSEP/MEP during correction.
Location: exit the neural foramina below each pedicle, 2–5 mm inferior to the screw trajectory. Protection: probe the inferior pedicle wall, avoid foraminal dissection, and take care with the steep L5 trajectory.
Location: aorta 15–25 mm anterior to the vertebral body, vena cava 10–20 mm anterior on the right. Protection: limit screw depth to the measured pedicle length minus 5 mm, confirm no anterior breach on fluoroscopy, and probe the anterior wall for resistance.
Location: enters the canal at T9–L2 (left side 80 percent) and supplies the anterior cord. Protection: maintain MAP greater than 85 mmHg during correction, avoid aggressive osteotomies at T9–L2, and watch SSEPs as an ischaemia indicator.
Location: exits the greater sciatic notch 2–3 cm from the PSIS, running between the iliac tables posteriorly. Protection: aim the iliac screw anteriorly (toward the AIIS), not posteriorly; fluoroscopy confirms the trajectory.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 14-year-old boy with Duchenne muscular dystrophy presents with progressive scoliosis. His curve is 35 degrees (thoracolumbar), he is wheelchair-dependent, FVC is 45 percent predicted, and echo shows EF 35 percent. Would you offer surgery? What are the key considerations in timing?”
“Why is pelvic fixation mandatory in neuromuscular scoliosis, and how do you achieve it? What are the specific risks of iliac screw placement?”
“What is the role of neuromonitoring in scoliosis surgery, and what is your algorithm if there are SSEP changes during curve correction?”
Indication
- Progressive neuromuscular scoliosis in DMD/BMD with curve greater than 20–30 degrees and documented progression
- Adequate pulmonary function: FVC greater than 30–40 percent predicted (ideal greater than 40 percent, prohibitive if less than 30 percent)
- Adequate cardiac function: EF greater than 30 percent on echo (need cardiology clearance and optimisation)
- Sweet spot: curve 30–50 degrees, FVC 40–60 percent, EF greater than 30 percent, before prohibitive risks
- Glucocorticoids have markedly reduced scoliosis incidence and severity — steroid-treated boys present later and fewer need fusion
The construct
- Pedicle screws at EVERY level (no skipped levels — osteoporotic bone), T2/T3 to pelvis
- Pelvic fixation is MANDATORY: bilateral S1 plus bilateral iliac screws (PSIS toward AIIS, 70–100 mm) plus offset connectors = four-point fixation
- Iliac trajectory is anterior (PSIS toward AIIS), never medial (vessels) or posterior (superior gluteal artery)
- S2AI screws are the modern, lower-profile alternative; both achieve rigid pelvic fixation
Key anatomy at risk
- Spinal cord: 2–3 mm anterior to the lamina — protect by probing all four pedicle walls and monitoring SSEP/MEP
- Nerve roots: below the pedicles in the foramina — protect by probing the inferior wall, careful L5 trajectory
- Great vessels: 15–25 mm anterior to the vertebral body — limit screw depth, confirm with fluoroscopy
- Artery of Adamkiewicz: T9–L2 (left 80 percent) — maintain MAP greater than 85 mmHg during correction
- Superior gluteal artery: 2–3 cm from the PSIS at the sciatic notch — aim iliac screws anteriorly
Operative pearls
- Thoracic entry: junction of transverse process and superior facet, 2–3 mm lateral to the facet; probe all four walls
- Posterior releases (facetectomies and ligamentum flavum at 4–6 apical levels) are usually sufficient — avoid PSO/VCR
- Correction is gradual and stepwise (cantilever, compression/distraction, derotation, translation) — goal coronal curve less than 20–30 degrees
- Generous decortication over T2 to pelvis; allograft is the primary graft (limited autograft in DMD)
- Blood loss averages 1–3 L — meticulous haemostasis, crossmatch 4–6 units, cell saver, controlled hypotension then raise MAP for correction
Complications
- Respiratory failure (20–30 percent) — most common; prevent with aggressive pulmonary toilet, BiPAP, early mobilisation
- Blood loss needing transfusion (greater than 50 percent)
- Neurologic deficit (1–3 percent) — prevent with neuromonitoring and gradual correction; STOP and release if signals change
- Infection (5–10 percent), pseudarthrosis (10–20 percent), proximal junctional kyphosis (10–20 percent), dural tear (5–10 percent)
Post-op
- All DMD patients go to ICU (1–3 days minimum)
- Respiratory care is the priority — overnight ventilation often needed, extubate when awake with a strong cough
- Frequent neuro checks (every 2–4 h) for delayed deficit
- Drains out when output less than 30 mL/8 h; sit day 1–2, wheelchair day 2–3, no brace needed
- Surgery does NOT stabilise FVC — pulmonary decline continues (Shapiro); counsel families the benefit is seating and comfort
Background & Evidence
Epidemiology and natural history. Before glucocorticoid therapy, around 90 percent of boys with DMD developed a progressive scoliosis once wheelchair-dependent, with curves typically worsening by 1–2 degrees per month. Long-term glucocorticoids (prednisolone/deflazacort) have markedly reduced both the incidence and severity of scoliosis, shifting surgery to fewer, often older patients — this modern natural-history shift must be reflected in any contemporary discussion of timing (Connolly 2013; Birnkrant 2018 DMD Care Considerations). Why pelvic fixation, and how early? Sengupta et al. compared pelvic with lumbar-only (to L5) fixation in 50 DMD patients: lumbar fixation to L5 was adequate only when surgery was performed early, with small curves and pelvic obliquity under 10 degrees; pelvic fixation was required for larger curves and established obliquity, and carried higher blood loss (mean 4.1 L) and longer stay. The lesson: operate before pelvic obliquity is established, and use pelvic fixation once it is. The honest evidence base. The Cochrane systematic review (Cheuk 2015) found that of 49 relevant studies NONE were randomised or quasi-randomised — the entire evidence base for this operation is observational (case-series, Level IV). Families should therefore be counselled honestly: the benefits of fusion (seating, comfort, pelvic obliquity correction) are supported only by observational data, and there is no proof it prolongs life or preserves pulmonary function. Shapiro et al. (1992) showed the FVC decline continues post-operatively (mean 45.3 percent pre-op falling to 28.7 percent at around 3.3 years) — it tracks muscle weakness, not the curve. This nuance is highly examinable. Key evidence messages. (1) Operate in the window before pelvic obliquity and prohibitive cardiopulmonary risk. (2) Pelvic fixation is mandatory once obliquity is established. (3) The indication is seating and comfort, not respiratory preservation. (4) Glucocorticoids have changed who needs surgery.
References
Surgery for scoliosis in Duchenne muscular dystrophy (Cochrane systematic review)
- Of 49 relevant studies, NONE were randomised or quasi-randomised controlled trials — all were prospective or retrospective case series
- There is therefore no high-level evidence that spinal fusion improves survival, respiratory function, quality of life or function in DMD scoliosis
- The entire evidence base for this operation is observational (case-series, Level IV)
Diagnosis and management of Duchenne muscular dystrophy, part 2: respiratory, cardiac, bone health, and orthopaedic management (DMD Care Considerations)
- International multidisciplinary consensus on orthopaedic, respiratory, cardiac and bone-health care across the DMD lifespan
- Glucocorticoids have markedly reduced the incidence and severity of scoliosis, shifting surgery to fewer, often older patients
- Pre-operative cardiac (echo) and respiratory (FVC, sleep study) assessment with optimisation is mandatory; nocturnal non-invasive ventilation may be needed peri-operatively
Pelvic or lumbar fixation for the surgical management of scoliosis in Duchenne muscular dystrophy
- Comparative study of 50 DMD patients: 31 with pelvic fixation (curve ~48 deg, FVC 44%) versus 19 with lumbar fixation to L5 (curve ~20 deg, FVC 58%)
- Lumbar fixation to L5 was adequate ONLY when surgery was performed early, with small curves and minimal pelvic obliquity (under 10 deg)
- Pelvic fixation was required for larger curves and established pelvic obliquity, and carried higher blood loss (mean 4.1 L) and longer stay
Spinal fusion in Duchenne muscular dystrophy: a multidisciplinary approach
- 27 DMD patients; mean pre-operative FVC 45.3% declining to 28.7% at ~3.3 years - surgery did NOT stabilise or improve pulmonary function
- Cardiac involvement common: abnormal shortening fraction (under 28%) in 7 of 16, with near-universal sinus tachycardia - underscores need for pre-op cardiac assessment
- Main benefit was easier, more comfortable wheelchair seating versus progressive deformity in non-operated patients
Corticosteroids can reduce the severity of scoliosis in Duchenne muscular dystrophy
- Long-term glucocorticoid therapy reduces both the incidence and severity of scoliosis in DMD
- Steroid-treated boys are less likely to develop progressive curves requiring fusion, and present later when they do
- Reflects the modern shift in DMD natural history driven by widespread glucocorticoid use