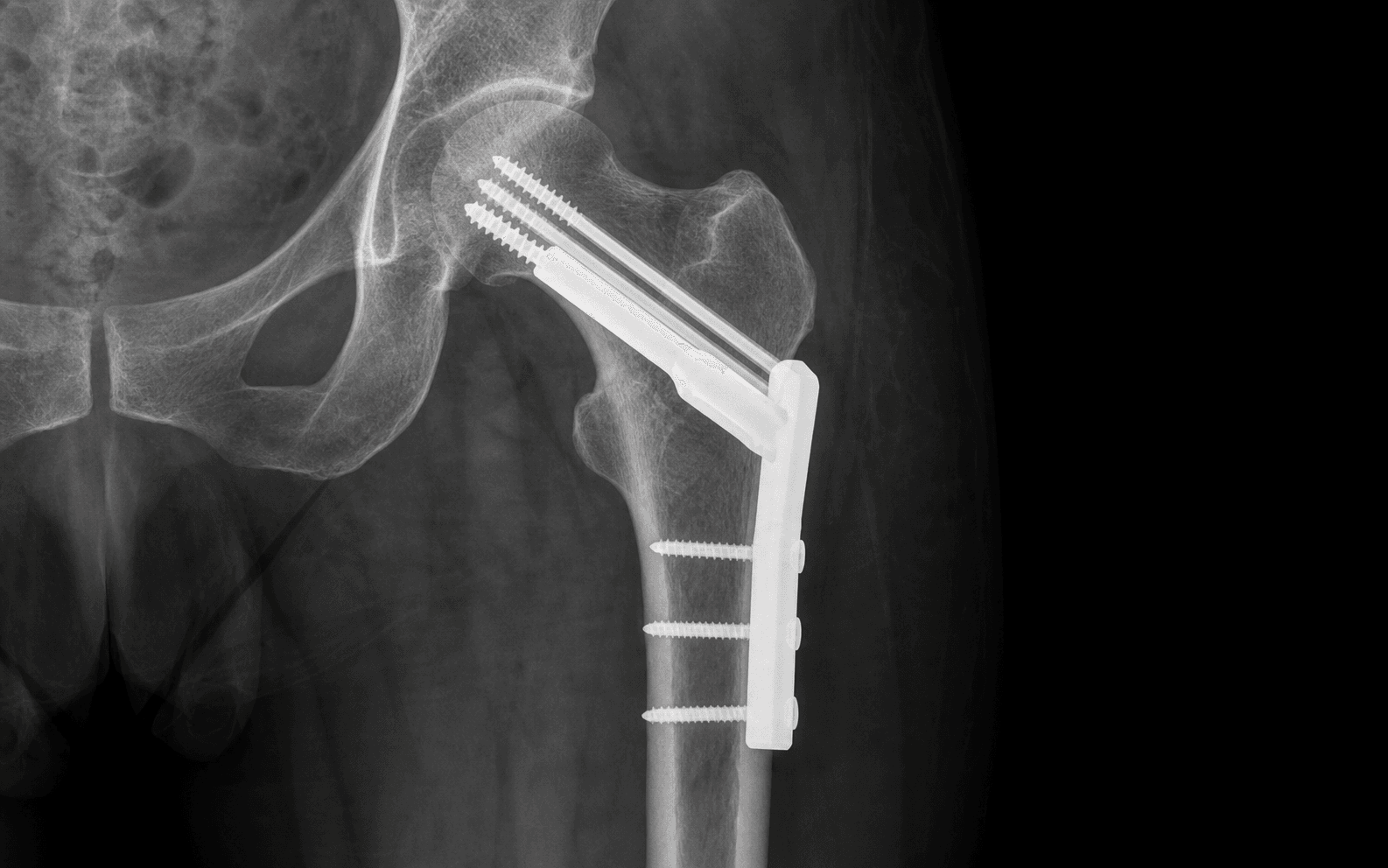
Lateral approach to the proximal femur for a DHS; percutaneous screws for the intracapsular fracture · intermediate
- Garden classification I-IV drives management, but it is displacement (undisplaced I-II versus displaced III-IV) that decides treatment and prognosis.
- Tip-apex distance must be 25mm or less — over 25mm multiplies cut-out risk about six-fold (Baumgaertner).
- Blood supply to the femoral head runs in retinacular vessels within the capsule, which is why displaced intracapsular fractures carry a 15-33 percent AVN risk while extracapsular fractures carry almost none.
- Surgery within 36 hours of admission improves outcomes (NICE), against a background 30-day mortality near 6.7 percent and 1-year mortality near 30 percent (NHFD).
When & Why
The single decision. For a femoral neck (intracapsular) fracture the choice is between internal fixation and arthroplasty, driven by displacement and patient factors, not by the Garden number in isolation. For an intertrochanteric or subtrochanteric (extracapsular) fracture the choice is between a dynamic hip screw (DHS) and a cephalomedullary nail, driven by stability. Intracapsular (femoral neck) fractures — fix or replace?
- Recommended treatment
- Cannulated screws (or sliding hip screw)
- Why
- Capsule intact, retinacular vessels only kinked — AVN risk 5-10 percent; fixation preserves the native head
- Recommended treatment
- Anatomical reduction and fixation (open if closed fails)
- Why
- Preserve the native femoral head; accept AVN/nonunion risk in return for easier later revision
- Recommended treatment
- Arthroplasty — hemiarthroplasty or THR
- Why
- Fixation fails too often (AVN 15-33 percent, nonunion 15-30 percent); arthroplasty gives one definitive operation
- Recommended treatment
- Total hip replacement
- Why
- Better long-term function; avoids acetabular erosion of hemiarthroplasty
- Recommended treatment
- Arthroplasty
- Why
- Fixation will not hold in diseased bone
Choosing between hemiarthroplasty and THR (when arthroplasty is indicated). Offer THR to independent ambulators with intact cognition, life expectancy greater than 5 years and a healthy acetabulum. Offer hemiarthroplasty to patients with limited mobility, cognitive impairment, significant comorbidity or shorter life expectancy. The HEALTH trial tempers this: in fit patients THR gives at best a marginal functional gain over hemiarthroplasty at the cost of higher dislocation, so it is selected rather than applied routinely. A special case — posterior tilt in undisplaced fractures. Garden I-II does not always mean fix. Posterior tilt of 20 degrees or more on the lateral radiograph (Okike, FAITH secondary analysis) doubles the risk of later conversion to arthroplasty, especially in patients 80 or older — consider primary arthroplasty rather than screws. Extracapsular (intertrochanteric or subtrochanteric) fractures — DHS or nail?
- Recommended implant
- Dynamic hip screw (DHS)
- Why
- Load-sharing sliding implant; reliable for stable patterns
- Recommended implant
- DHS (acceptable)
- Why
- Still reducible with a lateral plate
- Recommended implant
- Cephalomedullary nail
- Why
- DHS fails on unstable patterns; the nail is load-sharing and controls the medial column
- Recommended implant
- Cephalomedullary nail
- Why
- High-stress zone; the nail is the standard
- Recommended implant
- Cephalomedullary nail
- Why
- Better load sharing, faster surgery, earlier mobilisation
Age and functional framing. - Young patients (under 60): preserve the native femoral head at almost any cost. Demand anatomical reduction (under 2mm displacement), accept the AVN/nonunion risk, and proceed to open reduction if closed reduction is inadequate. The trade-off is worth it because revision arthroplasty is easier after failed fixation than a primary arthroplasty revised in a young patient.
- Elderly patients (over 75): a lower threshold for arthroplasty in displaced intracapsular fractures. Weigh surgical risk against functional outcome — an ASA 4 patient may be better served by a 30-minute percutaneous screw fixation than a 90-minute hemiarthroplasty. Always set expectations using registry data (30-day mortality near 6.7 percent, 1-year near 30 percent). Timing and medical optimisation. NICE guidelines recommend surgery within 36 hours of admission for a patient who is medically fit — earlier surgery reduces complications and mortality. Optimise in parallel, not serially: anaemia (restrictive transfusion, Hb under 80 g/L or under 90 g/L if symptomatic or with cardiac disease); anticoagulation (reverse warfarin with vitamin K and PCC, hold DOACs per half-life); cardiovascular (rate and rhythm control, continue beta-blockers); fluids and urine output. Do not delay surgery indefinitely for perfect optimisation — most patients benefit from early surgery. Consent specifically for: fixation versus arthroplasty and what drives the choice; AVN (15-33 percent) and nonunion (15-30 percent) risk if fixing a displaced neck fracture; cut-out and revision surgery; mobility expectations; and the realistic mortality figures.
The Operation
The goal is to reduce the fracture and stabilise it so the patient can mobilise on day one. Two operations share this section: the dynamic hip screw through an open lateral approach (for stable extracapsular fractures), and cannulated screw fixation done percutaneously (for intracapsular fractures). Both begin on a fracture table with image-intensifier control, and both live or die by guide-wire position and the tip-apex distance.
The exposure: the lateral approach to the proximal femur. The DHS is done through a longitudinal lateral incision. The internervous plane lies between vastus lateralis (femoral nerve, anterior compartment) and the posterior compartment muscles, separated by the lateral intermuscular septum. You elevate vastus lateralis anteriorly off the lateral femoral shaft in a subperiosteal plane to expose the lateral cortex for the plate. The structures you must respect, layer by layer:
Anteromedial, 3-4cm medial to the femoral neck. Protected by staying lateral and keeping retractors on bone, not soft tissue.
1-2cm posterior to the posterior femoral cortex at the lesser trochanter level. Avoid any posterior dissection beyond the femur.
Exits the greater sciatic notch superior to piriformis and runs 3-5cm above the greater trochanter tip. Limit proximal dissection above the trochanter to protect it.
Run along the lateral intermuscular septum into vastus lateralis. Control with bipolar cautery, not blind clamping; elevate vastus subperiosteally to preserve them where possible.
Dynamic hip screw — the open lateral approach
- Supine on a fracture table with a radiolucent top; a perineal post between the legs, well padded with foam to protect the pudendal nerve.
- Injured leg in a padded traction boot; uninjured leg in hemilithotomy (abducted 45 degrees, hip and knee flexed) or extended on a lateral support if hemilithotomy blocks the C-arm.
- C-arm on the opposite side from the surgeon. Confirm AP pelvis, AP hip and a true lateral hip are all obtainable before prepping and draping — discovering an inadequate lateral view after draping is the classic error.
- Longitudinal traction with the limb in neutral rotation (not the internal rotation used for intracapsular fractures).
- Restore the neck-shaft angle to 125-135 degrees; slight valgus is preferred over varus (varus under 10 degrees is acceptable).
- Aim for medial cortex continuity or a gap under 2cm, alignment within 5mm on the lateral with no more than 20 degrees of posterior sag.
- Reverse-obliquity or a large posteromedial fragment signals an unstable pattern — abandon the DHS for a nail.
- Palpate the greater trochanter. Make a longitudinal lateral incision centred on the femur, beginning about 2cm distal to the trochanter tip and running 8-12cm parallel to the shaft (longer for a 6-hole plate).
- Incise skin and subcutaneous tissue; control the generous elderly subcutaneous bleeding with diathermy. Identify the white glistening fascia lata.
- Incise the fascia lata in line with the skin for the full length of the incision.
- Identify the anterior edge of vastus lateralis and elevate it anteriorly off the lateral femoral shaft with a periosteal elevator, starting distally (easier) and working proximally, in a subperiosteal plane to preserve its blood supply.
- Place an anterior Hohmann retractor with its tip on the anterior femoral cortex (retracting vastus) and a posterior Hohmann on the posterior cortex. Keep retractors on bone, not soft tissue.
- Control the lateral circumflex perforators along the septum with bipolar cautery.
- Attach the 135 degree (or 150 degree) DHS guide to the lateral cortex. Entry point on the anterior third of the lateral cortex, 1-2cm distal to the vastus ridge, so the wire lies centrally in the neck.
- Aim for centre-inferior in the head: central or inferior-third on AP, central or inferior-third on lateral. Advance a 2.0-2.5mm smooth wire to 5-10mm from subchondral bone.
- Measure the tip-apex distance: distance from wire tip to the femoral head apex on AP plus the same on lateral. The sum must be 25mm or less. If it is over 25mm, reposition the wire more inferior and posterior before reaming.
- Ream over the wire with the cannulated triple reamer (typically 10-12.5mm) to a depth 5-10mm short of the measured wire depth, clearing flutes every 2-3cm and re-checking the wire has not advanced.
- Select a partially-threaded lag screw 5-10mm shorter than the measured depth; the threads must engage only the head fragment so the smooth shaft traverses the fracture and creates lag.
- Advance the screw to leave its tip 5-10mm from subchondral bone. Confirm the screw slides freely in the barrel before assembling the plate.
- Slide the barrel (a 4-hole plate for most fractures; 6-8 hole for subtrochanteric extension or osteoporotic bone) over the lag screw and seat it flush on the lateral cortex.
- Verify 10-15mm of threaded lag-screw shaft is visible outside the barrel on the lateral view — this collapse space is what lets the fracture impact during healing. If the screw is bottomed out, use a shorter screw.
- Hold with a clamp, then insert the 4.5mm cortical distal screws sequentially, bicortical, from distal to proximal (drill 3.2mm, measure, tap in young bone, insert length plus 2-4mm).
- AP: reduction held, lag screw centre-inferior, tip-apex distance 25mm or less, plate flush, distal screws bicortical.
- Lateral: no posterior sag, 10-15mm collapse space visible.
- Release traction slowly under fluoro — the fracture should remain reduced; slight impaction is normal and desired.
Cannulated screw fixation — percutaneous, for the intracapsular fracture
- A standard radiolucent table (no fracture table) suits most screw fixings: the surgeon can manipulate rotation freely, which is the key to reducing an intracapsular fracture. A skilled assistant applies manual traction.
- Reduce with the Leadbetter manoeuvre: flex the hip to 90 degrees, apply traction, internally rotate 15-20 degrees, circumduct, then extend to neutral holding traction and rotation.
- Check reduction on AP and lateral — Garden alignment index about 160 degrees on AP (150 to 170 acceptable) and about 180 degrees on lateral (170 to 190), with displacement under 2mm in the young.
- Place three 2.0-2.5mm wires percutaneously through stab incisions in an inverted triangle: an inferior wire first (entry 2cm distal to the vastus ridge, avoiding the lesser trochanter, determining minimum screw length), then a posterior-superior and an anterior-superior wire.
- The wires must be parallel within 10 degrees of each other and spread more than 15mm apart at the fracture site to resist rotation and shear. All tips 5mm short of subchondral bone on both views.
- Over each wire, drill only the near (lateral) cortex to create a glide hole, so the threads of the 6.5-7.0mm partially-threaded cannulated screws engage the far head fragment only.
- Measure each wire; use the shortest measurement (usually the inferior wire) and select screws 5-10mm shorter, with a 16mm or 32mm thread chosen so the threads cross the fracture.
- Insert all three screws partially, then tighten in an alternating sequence (inferior, posterior, anterior, a few turns each, repeat) so compression is even and no single screw bottoms out first. Watch the fracture gap close on fluoro.
- AP and lateral: three parallel screws, spread over 15mm at the fracture, tips 5mm from subchondral bone, no head penetration.
- Remove the wires. Close the fascia (2-0 Vicryl) and skin; no drain is needed for percutaneous screws.
The femoral neurovascular bundle lies 3-4cm medial to the femoral neck and the sciatic nerve 1-2cm posterior to the posterior cortex at the lesser trochanter. The lateral approach protects both — provided dissection stays on bone and retractors are placed on cortex, not soft tissue. Limit any proximal dissection to within 5cm of the greater trochanter tip to spare the superior gluteal neurovascular bundle.
A tip-apex distance over 25mm multiplies lag-screw cut-out risk about six-fold (Baumgaertner). Before reaming, measure AP and lateral, add them, and reposition the wire centre-inferior if the sum exceeds 25mm. The few minutes spent now prevent a cut-out and a revision operation in 6-12 months.
On the lateral view, 10-15mm of threaded lag-screw shaft must sit outside the barrel. This is the sliding mechanism that lets the fracture impact and compress under load. If the screw is bottomed out in the barrel the construct cannot collapse, and cut-out risk rises — use a shorter screw.
More than 20 degrees of posterior sag on the lateral view quietly increases cut-out risk even when the AP looks acceptable. Always judge reduction on both views, and prefer a nail over a DHS when the medial column or posterior wall is comminuted.
Aftercare & Complications
Rehabilitation — weight-bearing and recovery | Fixation | Weight-bearing | Milestones | |----------|----------------|------------| | Extracapsular (DHS or nail) | Weight-bearing as tolerated from day 1 | Independent mobilisation before discharge; full function by 3 months | | Intracapsular, elderly | Weight-bearing as tolerated from day 1 | As above | | Intracapsular, young (under 60) | Partial (toe-touch to 50 percent) for 6 weeks, then progress | Protects fixation while the head revascularises; full load by 10-12 weeks | | Arthroplasty | Weight-bearing as tolerated from day 1 (unless perioperative fracture) | As above | Mobilise on day 0 or day 1 — early mobilisation reduces pneumonia, DVT, delirium and pressure sores. Use a multimodal analgesia plan built around scheduled paracetamol and a fascia iliaca block, minimising the opioids that drive delirium in the elderly. Aim for discharge once the patient is medically stable, pain is controlled on oral analgesia, and mobility and a safe home environment (occupational therapy assessment, equipment) are in place. Follow-up. At 2 weeks review the wound and mobility. At 6 weeks take an AP pelvis and lateral hip to assess healing, hardware position and early AVN in intracapsular fractures (advance the young intracapsular patient from partial to full weight-bearing if healing is progressing). At 3 months assess union and watch for AVN (MRI is more sensitive than radiograph). At 12 months confirm union and functional outcome. For every patient, treat the underlying osteoporosis: DEXA, a bisphosphonate (alendronate 70mg weekly or zoledronic acid 5mg yearly, which cuts re-fracture risk by about 40 percent), calcium 1200mg plus vitamin D 800IU daily, and a falls-prevention programme. Venous thromboembolism prophylaxis is mandatory. Give LMWH (enoxaparin 40mg subcutaneously daily) or a DOAC (rivaroxaban 10mg daily, apixaban 2.5mg twice daily) starting 6-12 hours post-op once haemostasis is adequate, continuing for a minimum of 35 days (NICE), alongside mechanical prophylaxis until the patient is mobile. Aspirin alone is inadequate. Complications
- Recognition
- Hip pain at 8-24 months; radiograph shows segmental collapse (crescent sign, sclerosis). MRI diagnostic earlier
- Prevention
- Anatomical reduction and early fixation of intracapsular fractures; primary arthroplasty for displaced fractures in the elderly
- Management
- Symptomatic AVN needs arthroplasty (THR if acetabulum healthy, hemi if not). Core decompression is not effective post-trauma
- Recognition
- Persistent pain at 3-6 months, unable to weight-bear, fracture line without bridging callus, loss of fixation
- Prevention
- Anatomical reduction (gap over 2mm impairs healing), stable fixation, early weight-bearing, smoking cessation, nutrition
- Management
- Intracapsular: convert to arthroplasty. Extracapsular: revision nail or blade plate with graft; arthroplasty if severe osteoporosis
- Recognition
- Acute pain, inability to weight-bear, lag screw protruding into the acetabulum on AP or lateral, varus collapse
- Prevention
- Tip-apex distance 25mm or less, centre-inferior position, avoid varus, ensure 10-15mm collapse space
- Management
- Almost always needs revision: nail or blade plate in good bone; arthroplasty in the elderly or osteoporotic
- Recognition
- Trendelenburg gait, leg-length discrepancy, reduced hip motion, pain from altered joint forces
- Prevention
- Anatomical reduction on both views, slight valgus over varus, adequate distal fixation, medial cortex support
- Management
- Mild varus (under 15 degrees) in the elderly: observe. Significant varus: corrective valgus osteotomy (young) or arthroplasty (elderly)
- Recognition
- Calf pain and swelling (DVT); dyspnoea, chest pain, hypoxia (PE). Ultrasound for DVT, CTPA for PE
- Prevention
- Mechanical plus chemical prophylaxis for 35 days minimum, early mobilisation, hydration
- Management
- Therapeutic anticoagulation 3-6 months; thrombolysis or embolectomy for massive PE; IVC filter if anticoagulation contraindicated
- Recognition
- Erythema, drainage, dehiscence, fever; deep: persistent pain, raised inflammatory markers, radiographic loosening
- Prevention
- Cefazolin prophylaxis, meticulous haemostasis, normothermia, glycaemic control, minimise operative time
- Management
- Superficial: oral antibiotics and wound care. Deep early (under 3 weeks): washout with implant retention plus IV antibiotics. Deep late: washout, implant removal if loose, staged revision
- Recognition
- Acute confusion; fever, cough, hypoxia; chest pain and ECG changes; sacral or heel breakdown; dysuria
- Prevention
- Orthogeriatric co-management, early mobilisation, minimise opioids, avoid catheters, pressure care, nutrition
- Management
- Treat the cause; antibiotics and physiotherapy as indicated; prevention is far easier than treatment
Viva & Exam Focus
GARDENGARDEN — staging the intracapsular fracture
TADTAD 25mm or less — the DHS target
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 78-year-old woman who was independently mobile sustains a displaced intracapsular hip fracture (Garden III). She has hypertension and type 2 diabetes. What are your options and how do you decide?”
“During a DHS for an intertrochanteric fracture you measure the tip-apex distance at 28mm after inserting the lag screw and plate. What is the significance, and what do you do?”
“Explain the blood supply to the femoral head, and why displaced intracapsular fractures risk AVN while extracapsular fractures do not.”
Indication
- Intracapsular undisplaced (Garden I-II): cannulated screws any age if anatomically reduced
- Intracapsular displaced, young (under 60-65): fixation if anatomical closed reduction, else open reduction
- Intracapsular displaced, elderly (over 65-70): arthroplasty (THR if fit, hemi if not)
- Extracapsular stable (AO 31-A1): DHS
- Extracapsular unstable (A2/A3, reverse obliquity, subtrochanteric): cephalomedullary nail
- Posterior tilt 20 degrees or more in Garden I-II: consider arthroplasty (Okike)
Exposure and danger
- Lateral approach; internervous plane vastus lateralis (femoral nerve) versus posterior compartment
- Elevate vastus anteriorly, subperiosteal, retractors on bone
- At risk: femoral neurovascular (3-4cm medial), sciatic nerve (1-2cm posterior at lesser trochanter), superior gluteal bundle (3-5cm above GT), lateral circumflex perforators
Critical steps
- Fracture table, perineal post padded, traction 20-30 lbs, check all fluoro views before prep
- Closed reduction intracapsular: Leadbetter (flex, traction, internal rotation, circumduct, extend)
- DHS guide wire centre-inferior on AP and lateral
- Tip-apex distance 25mm or less (over 25mm equals about 6x cut-out)
- Cannulated screws: three parallel (within 10 degrees), spread over 15mm, inverted triangle, tighten alternately
- Collapse space 10-15mm of shaft outside the barrel
Complications
- AVN: displaced intracapsular 15-33 percent, presents 8-24 months, MRI early, arthroplasty
- Nonunion: displaced intracapsular 15-30 percent, convert to arthroplasty
- Cut-out: DHS 3-5 percent (up to 15 percent if TAD over 25mm), revise
- VTE: mandatory LMWH or DOAC for 35 days, early mobilisation
- Medical: delirium 30-50 percent (minimise opioids), pneumonia 5-10 percent
Aftercare
- Weight-bearing: extracapsular or arthroplasty WBAT day 1; young intracapsular partial for 6 weeks
- VTE prophylaxis 35 days minimum (NICE)
- Multimodal analgesia, fascia iliaca block, minimise opioids
- Treat osteoporosis: DEXA, bisphosphonate, calcium and vitamin D, falls prevention
Background & Evidence
Epidemiology. Hip fracture is one of the most common serious injuries of older adults, with a strong female predominance and a peak in the eighth decade and beyond. The major hip-fracture and arthroplasty registries — the UK National Hip Fracture Database (NHFD) and National Joint Registry (NJR), the American Joint Replacement Registry (AJRR), the Australian AOANJRR, and the Swedish (SHAR) and Norwegian registers — consistently report 30-day mortality of roughly 6-8 percent and 1-year mortality of roughly 25-30 percent, and a far lower reoperation rate after hemiarthroplasty than after internal fixation for displaced intracapsular fractures. Garden classification (intracapsular fractures). Garden I and II are undisplaced; III and IV are displaced. It is the displacement — not the stage number — that drives treatment and prognosis, and some Garden I fractures with marked posterior tilt behave as unstable.
- Description
- Incomplete or impacted — valgus impaction, undisplaced
- Typical management
- Cannulated screws if reduced; watch posterior tilt
- Description
- Complete but undisplaced — trabecular alignment preserved
- Typical management
- Cannulated screws (anatomically reduced)
- Description
- Complete with partial displacement — trabecular alignment lost
- Typical management
- Young: reduce and fix; elderly: arthroplasty
- Description
- Complete displacement — fragments fully separated, may rotate
- Typical management
- Young: anatomical reduction and fixation; elderly: arthroplasty
AO/OTA classification (extracapsular fractures). 31-A1 is a stable intertrochanteric fracture (intact medial cortex and lesser trochanter) — suit a DHS. 31-A2 is intertrochanteric with posteromedial comminution (a large fragment makes it unstable). 31-A3 is reverse-obliquity or intertrochanteric with subtrochanteric extension — unstable, suit a nail. Subtrochanteric fractures are AO/OTA 32-A, B and C. Pathoanatomy — why the blood supply governs everything. The femoral head is perfused by retinacular arteries that ascend along the neck within the capsule, arising mainly from the medial femoral circumflex artery (about 80 percent) with a contribution from the lateral femoral circumflex (about 20 percent); they enter the head at the head-neck junction, and the artery of the ligamentum teres is a minor contributor in adults. A displaced intracapsular fracture tears these vessels (AVN 15-33 percent); an undisplaced one only kinks them (5-10 percent); an extracapsular fracture leaves them intact (AVN essentially zero). Capsular tamponade from haematoma may compound the ischaemia — the theoretical rationale for capsulotomy, though a clear benefit is unproven. The neck-shaft angle is 125-135 degrees (reducing with age) with 10-15 degrees of anteversion; the calcar femorale is the dense medial buttress whose integrity marks a fracture as stable, and Ward's triangle is an area of relative weakness inferior to the head. Key evidence. The FAITH trial (2017) found no overall difference in 24-month reoperation between sliding hip screw and cannulated screws for femoral neck fractures in patients 50 or older, though AVN was more frequent with the sliding hip screw and selected subgroups (smokers, displaced, base-of-neck) trended toward it. The HEALTH trial (2019) found THR offered at best a marginal functional gain over hemiarthroplasty in fit patients at the cost of higher dislocation. The Norwegian Hip Fracture Register (Gjertsen, 2010) showed reoperation far higher after screw fixation than hemiarthroplasty (22.6 percent versus 2.9 percent) with no mortality difference, cementing arthroplasty as the standard for displaced neck fractures in the elderly. Okike's FAITH secondary analysis (2019) showed posterior tilt of 20 degrees or more doubled conversion to arthroplasty in Garden I-II fractures. Baumgaertner (1995) established the tip-apex distance, the single most important modifiable technical factor in DHS fixation.
References
The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip
In 198 peritrochanteric fractures fixed with a sliding hip screw, 16 of 19 failures were lag-screw cut-out; mean tip-apex distance was 24mm in healed fractures versus 38mm in cut-outs, and none of 120 screws with a tip-apex distance of 25mm or less cut out. TAD under 25mm is the universally quoted DHS target.
Fracture fixation in the operative management of hip fractures (FAITH): an international, multicentre, randomised controlled trial
In 1108 patients aged 50 or older across 8 countries, sliding hip screw and cannulated screws showed no significant difference in 24-month reoperation (20 percent versus 22 percent). AVN was more frequent with the sliding hip screw (9 percent versus 5 percent); smokers and displaced or base-of-neck patterns trended toward benefit from it.
Effect of posterior tilt on rates of subsequent arthroplasty after internal fixation of Garden-I and II femoral neck fractures (FAITH secondary analysis)
In 555 Garden I-II fractures treated by fixation, posterior tilt of 20 degrees or more doubled the risk of later arthroplasty (22.4 percent versus 11.9 percent); age 80 or older was the other independent predictor.
Total Hip Arthroplasty or Hemiarthroplasty for Hip Fracture (HEALTH trial)
In 1495 independently ambulating patients aged 50 or older, secondary hip procedures at 24 months did not differ between THR and hemiarthroplasty (7.9 percent versus 8.3 percent); THR gave only a small, clinically unimportant functional gain but higher dislocation (4.7 percent versus 2.4 percent).
Internal screw fixation compared with bipolar hemiarthroplasty for displaced femoral neck fractures in elderly patients (Norwegian Hip Fracture Register)
In 4335 patients over 70 with displaced neck fractures, reoperation was far higher after screw fixation (22.6 percent versus 2.9 percent) with equivalent one-year mortality; the hemiarthroplasty group had less pain and better quality of life.
Low-angle fixation in fractures of the femoral neck — the Garden classification
The original description of the four-stage classification of femoral neck fractures that still guides management.
Hip fracture: management — Clinical Guideline CG124
UK guidance recommending surgery within 36 hours where the patient is medically fit, orthogeriatric co-management, multimodal analgesia, early mobilisation, and 35-day VTE prophylaxis. Broadly concords with AAOS and AO Foundation principles globally.