Closed reduction and percutaneous pinning is the standard; open reduction is reserved for the irreducible, open or white/cold pulseless hand | high
- Closed reduction and percutaneous pinning (CRPP) is the gold-standard operative treatment for displaced paediatric supracondylar fractures - open reduction is the exception, not the rule
- Open reduction is indicated ONLY for: an irreducible fracture (usually soft-tissue interposition), an open fracture, a white/cold pulseless hand needing brachial artery exploration, or pin fixation that cannot be achieved closed
- When open reduction IS required for an extension-type fracture, the anterior or medial approach is preferred - a posterior approach is generally avoided because it disrupts the remaining intact posterior periosteal hinge and the distal fragment blood supply, increasing the risk of osteonecrosis and stiffness
- “Know the Gartland classification inside-out (I: undisplaced, II: displaced with intact posterior cortex, III: completely displaced) - it drives every management decision
- “Describe the paediatric elbow neurovascular examination - median (AIN: OK sign), radial (PIN: finger extension), ulnar (intrinsics, sensation) nerves and the radial pulse
- “Compartment syndrome is the nightmare complication - know the early signs (pain with passive finger extension, pain out of proportion), prevention (avoid flexion greater than 90 degrees, overnight monitoring) and urgent management (fasciotomy, do not wait for pressure measurements)
When & Why
Indication. A displaced extension-type supracondylar humerus fracture in a child - Gartland IIB or III - that cannot be managed in a cast alone. Gartland I (undisplaced) is treated non-operatively in an above-elbow cast for three weeks; Gartland IIA/B and III are treated by closed reduction and percutaneous pinning (CRPP), which is the gold-standard operation. Open reduction is the exception, reserved for specific situations below. Other operative indications include a failed closed reduction (a Gartland IIA that will not hold), a fracture needing vascular exploration, an open fracture requiring debridement, and the floating elbow (an ipsilateral forearm fracture) that needs both injuries stabilised. Assess the limb before the operation. Document a detailed neurovascular examination on arrival and again after any manipulation: the radial pulse, capillary refill (less than 2 seconds), and the three nerves at risk - the median nerve (test the anterior interosseous branch with the OK sign - thumb IP plus index DIP flexion), the radial nerve (finger and thumb extension, the posterior interosseous branch) and the ulnar nerve (finger abduction and adduction, intrinsic function, and sensation). The anterior interosseous nerve is the one most often injured by the fracture itself, not by surgery. Obtain AP and lateral radiographs and classify the fracture by Gartland. The one decision that matters. Every displaced fracture begins with an attempt at closed reduction and percutaneous pinning. The only real choice is when to abandon it and open:
The default for every Gartland IIB/III fracture. No incision is made for reduction; pins enter through lateral (and, rarely, medial) stab incisions. Lowest morbidity and fastest recovery.
Only for the irreducible fracture (soft-tissue interposition - usually brachialis, sometimes the brachial artery or median nerve), the open fracture, or the white/cold pulseless hand. The anterior approach addresses the anteriorly-displaced spike and any interposed structures directly and preserves the intact posterior periosteal hinge.
Mandated by a white, cold, pulseless hand that does not re-perfuse after gentle closed reduction. Performed through the same anterior exposure with vascular surgery on standby.
Avoid the posterior approach for a typical extension fracture: it divides the one structure - the posterior periosteum - that is usually still intact as the reduction hinge, and it strips the tenuous distal-fragment blood supply, increasing the risk of osteonecrosis and stiffness. The pulseless hand - decide before you operate. After a gentle closed reduction with the elbow at 60 to 70 degrees of flexion, reassess perfusion. The action depends on the hand's colour and warmth, not on the pulse alone:
- Pulse
- Present
- Action
- Standard CRPP and routine care
- Pulse
- Absent
- Action
- Pulseless pink hand - collaterals are adequate; close observation with hourly overnight neurovascular checks, and a low threshold to explore if any deterioration
- Pulse
- Absent
- Action
- URGENT brachial artery exploration through an anterior approach with vascular surgery on standby
The Operation
The goal is to reduce the fracture closed, hold it with percutaneous K-wires that engage both columns with bicortical purchase, confirm reduction on four fluoroscopic views, and immobilise at modest flexion while protecting the brachial artery and the three nerves at risk. The exposure for the rare open case is the anterior approach, laid out inline as the early steps below - this is the heart of the operation.
Operative sequence
- Supine on a radiolucent arm board or hand table, using the C-arm as the working surface so AP and lateral images are obtained by rotating the shoulder and forearm, not by moving the elbow.
- A tourniquet is usually NOT applied for routine CRPP and must be avoided whenever there is any vascular concern; have vascular surgery contactable if the pulse is absent pre-operatively.
- Prep and drape the entire upper limb from shoulder to fingertips; confirm the contralateral elbow is available (clinically or radiographically) as the reduction reference.
- This is fundamentally a closed procedure - set up so a clean lateral is obtained by externally rotating the shoulder rather than by flexing or extending the fracture.
- With the patient anaesthetised and muscles relaxed: (1) apply longitudinal traction with the elbow in slight extension to disimpact; (2) correct medial/lateral translation and any rotation by direct pressure on the distal fragment; (3) for the typical extension fracture, push the olecranon anteriorly with the thumb and flex the elbow past 90 to 120 degrees to lock the reduction against the intact anterior periosteal hinge while pronating the forearm.
- Posteromedial displacement (the most common pattern) is reduced with the forearm PRONATED; posterolateral displacement is reduced supinated.
- The anterior periosteum is the hinge in an extension fracture - flexion and pronation tension it and stabilise the reduction. Reduction is judged on fluoroscopy, NOT by feel.
- Avoid repeated forceful manipulation (it increases swelling and compartment risk), hyperflexion that compromises a tenuous brachial artery (re-check perfusion after flexing), and over-manipulation that converts a reducible fracture into an unstable one.
- Assess reduction on fluoroscopy: anterior humeral line through the middle third of the capitellum on a true lateral, restored Baumann angle on AP, and aligned medial and lateral columns.
- If reduction is anatomical, proceed to pinning. If the fracture is IRREDUCIBLE after one or two gentle attempts (suggesting interposed soft tissue - usually brachialis, with a "pucker sign" of anterior skin dimpling; sometimes the brachial artery or median nerve), OR the hand is white/cold, OR the fracture is open, convert to OPEN reduction through an anterior (or medial) approach to extract the interposed tissue and inspect the neurovascular bundle directly.
- Do not keep manipulating an irreducible fracture - OPEN it. Use an ANTERIOR approach for an extension fracture (the spike, brachialis, brachial artery and median nerve are all anterior and addressed directly) and preserve the intact posterior periosteum; avoid the posterior triceps-splitting approach.
- Do not accept a malreduction to avoid opening (it causes cubitus varus), and do not persist with closed attempts once true irreducibility is recognised.
- With the reduction held (elbow flexed, forearm pronated), insert smooth K-wires (1.6 mm in small children, 2.0 mm in larger children) through the lateral epicondyle and capitellum via stab incisions.
- Pass each wire across the fracture to engage the opposite (medial) cortex with bicortical purchase; maximise pin SPREAD at the fracture line and ensure both the medial and lateral columns are engaged proximally.
- Two divergent lateral pins suffice for most fractures; add a third lateral pin if there is any concern about stability or pin position.
- Skaggs' four technical points for reliable lateral-entry fixation: (1) maximise pin separation at the fracture site, (2) engage BOTH columns proximally, (3) get adequate bone in the proximal and distal fragments, (4) keep a low threshold for a third lateral pin. Respecting these, lateral-only fixation maintains reduction even in unstable Gartland III/IV patterns and avoids the ulnar nerve entirely.
- Avoid pins too close together (poor rotational control and loss of reduction), unicortical purchase (secondary displacement), and a lateral pin straying anteromedially (risk to the radial/posterior interosseous nerve or brachial artery).
- Only if the medial column is very unstable or comminuted: make a small medial incision down to the medial epicondyle so the entry point is seen, flex the elbow LESS once the lateral pins are in (hyperflexion drives the ulnar nerve anteriorly toward the pin), palpate or directly visualise the ulnar nerve, and direct the pin proximally and slightly anteriorly away from the nerve; confirm no nerve irritation.
- The ulnar nerve subluxes ANTERIORLY over the medial epicondyle in up to a fifth of children, especially in hyperflexion - this is why a "blind" percutaneous medial pin in a maximally flexed elbow is dangerous.
- A meta-analysis of paediatric supracondylar pinning shows iatrogenic nerve injury of roughly 3.4 percent with lateral-only versus 4.1 percent when a medial pin is added, the excess being ulnar nerve injury (Babal 2010).
- Default to lateral-only fixation when adequate - it removes ulnar nerve risk.
- Obtain AP, lateral and both oblique views with the C-arm. Confirm: Baumann angle 65 to 75 degrees on AP; anterior humeral line through the middle third of the capitellum on lateral; no coronal or sagittal angulation; medial and lateral columns aligned; pins engage both cortices proximally; no intra-articular pin penetration.
- The ANTERIOR HUMERAL LINE is critical on the lateral view - it should pass through the MIDDLE THIRD of the capitellum. If it lies anterior there is extension malreduction. BAUMANN ANGLE compared with the contralateral limb best assesses rotation - a difference greater than 5 degrees indicates rotational malreduction. Ensure ZERO medial or lateral translation on the AP view.
- Compare with the contralateral elbow if uncertain.
- Once position is confirmed perfect, advance pins until just engaging the far cortex (avoid prominent sharp tips); bend pins 90 degrees at skin level to prevent migration; cut leaving 1 cm proud of skin for easy removal at 3 to 4 weeks in clinic.
- Some surgeons bury pins beneath the skin if the family is compliant for removal under brief sedation later - this is NOT necessary in most cases.
- Pin migration is prevented by bending at skin. Left-out pins are removed easily in clinic at 3 to 4 weeks without sedation (a quick pull). Dress pins with antiseptic gauze and splint to prevent snagging.
- Watch for pin-track infection (2 to 5 percent incidence), pin migration causing neurovascular injury, and lost pins if cut too short and fallen into the soft tissues.
- Release the tourniquet if used. Assess elbow stability through a gentle flexion/extension arc (avoid forced motion that could displace the fracture or raise compartment pressure). Check mediolateral stability (no opening), palpate the radial pulse (should be present and strong), check capillary refill (less than 2 seconds), and assess median, radial and ulnar nerve function if the child is cooperative.
- POST-REDUCTION VASCULAR ASSESSMENT is mandatory - a pink, pulsatile limb is essential. If the pulse is absent: (1) reduce the elbow flexion angle (a kinked artery), (2) remove any constricting dressings, (3) consider brachial artery exploration if no pulse returns after reduction. Attempt anterior interosseous (median), PIN (radial), and ulnar motor and sensory testing.
- Routine CRPP leaves only pin-site stab wounds - there is NO triceps to repair, which is one reason CRPP is preferred over a posterior open approach.
- If an open reduction was performed, close the anterior (or medial) incision in layers with absorbable subcutaneous suture and a subcuticular skin closure; the brachialis is not formally repaired and the posterior periosteal hinge is left undisturbed. Do not attempt to repair brachialis or strip more periosteum.
- Dress pin sites with antiseptic gauze. Avoid skin tethering against a pin, haematoma under a tightly closed open-reduction wound, and suture knots causing skin irritation.
- Apply a well-padded above-elbow backslab or split cast. Immobilise the elbow at only 60 to 90 degrees of flexion in this swollen, freshly reduced limb - the fracture is held by the pins, NOT by extreme flexion. Position the forearm in the rotation that held the reduction (usually neutral to mid-pronation).
- Avoid a circumferential, tight cast in the acute setting. Once the fracture is pinned, stability comes from the wires, so there is NO need to splint in hyperflexion - flexion beyond 90 degrees kinks the brachial artery and raises forearm compartment pressure.
- Counsel parents on warning signs: severe pain, numbness, white or blue fingers, inability to move the fingers.
- Admit overnight for neurovascular observation: hourly checks of radial pulse, capillary refill, finger motion and sensation, and pain assessment.
- For any concern for compartment syndrome (pain out of proportion, tense forearm, pain with passive finger extension, progressive neurological deficit), REMOVE the splint immediately and reassess - low threshold to return to theatre for fasciotomy.
- COMPARTMENT SYNDROME is the most devastating complication of paediatric supracondylar fractures - it leads to Volkmann ischaemic contracture and permanent disability. It is a CLINICAL diagnosis - do NOT wait for compartment pressure measurement. Pain out of proportion and pain with passive finger/thumb extension are the earliest signs; missed diagnosis is a medicolegal catastrophe.
- Obtain AP and lateral elbow radiographs in recovery to document maintained reduction; check weekly for the first 2 to 3 weeks to ensure no loss of reduction.
- Remove pins at 3 to 4 weeks in clinic (the fracture is healed by this time in children); start gentle active ROM after pin removal - children regain motion quickly and rarely need formal therapy.
- Expect full ROM by 6 to 8 weeks; no contact sports for 8 to 12 weeks. Paediatric bone heals rapidly (3 weeks is adequate for union); remodelling potential is excellent for residual angulation but NOT for rotation (rotation cannot remodel).
After every manipulation and again after pinning, reassess perfusion. Excessive elbow flexion kinks the brachial artery; if the pulse is lost, first reduce the flexion angle and remove any constricting dressing. A pink, warm hand with an absent pulse may be watched overnight (the collaterals are adequate), but a white, cold hand mandates urgent brachial artery exploration through an anterior approach with vascular surgery on standby. A persistently pulseless pink hand with worsening pain or a deepening nerve lesion should be explored, not observed - collateral flow does not always prevent late Volkmann ischaemic contracture.
If a medial pin is needed, insert the lateral pins first, then REDUCE elbow flexion before placing the medial pin - hyperflexion subluxes the ulnar nerve anteriorly over the medial epicondyle and onto the pin path (the dangerous misconception is that maximal flexion protects the nerve). Use a mini-open incision to see the medial epicondyle, palpate or visualise the nerve throughout, and direct the pin proximally away from it. Default to lateral-only fixation whenever it is adequate.
When open reduction is unavoidable, the anterior (or medial) approach addresses the anteriorly-displaced metaphyseal spike and any interposed brachialis, brachial artery or median nerve directly, and preserves the intact posterior periosteal hinge. A posterior triceps-splitting approach divides that hinge and strips the tenuous distal-fragment blood supply - reserve it for the rare flexion-type fracture.
Five structures at risk - know the location and the protection strategy for each:
Anterior to the distal humerus, medial to the median nerve. Assess the pulse before and after reduction; reduce flexion if the pulse is lost; have vascular surgery on standby for the white and cold hand.
Anterior, medial to the brachial artery at the antecubital fossa. Avoid excessive anterior dissection; document the OK sign (AIN) pre-operatively - most AIN palsies are from the injury, not the surgery.
Lateral distal humerus, about 7 to 10 cm proximal to the lateral epicondyle. Limit proximal and lateral dissection; identify it if the approach is extended; keep lateral pins from straying anteromedially.
Cubital tunnel, about 10 to 20 mm medial to the olecranon tip. Identify before any medial pin; reduce flexion and palpate or visualise during insertion; prefer lateral-only fixation.
Branch of the median nerve in the proximal forearm. Document the OK sign (thumb IP plus index DIP flexion) pre-operatively; most palsies are from the injury and recover spontaneously.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Activity | |-------|--------|----------------|----------| | 1 | 0 to 2 weeks | Above-elbow backslab or split cast at 60 to 90 degrees flexion; overnight hourly neurovascular monitoring | Finger active ROM only | | 2 | 2 to 3 weeks | Well-padded splint; weekly radiographs to confirm maintained reduction | Gentle finger and wrist motion | | 3 | 3 to 4 weeks | Pin removal in clinic; splint for comfort | Begin gentle active elbow ROM | | 4 | 4 to 8 weeks | Splint off | Progressive ROM; children self-mobilise through play | | 5 | 8 to 12 weeks | Return to full activity | No contact sports until 8 to 12 weeks | Most children regain full motion by 6 to 8 weeks without formal therapy - they self-mobilise through play. Pins come out at 3 to 4 weeks (paediatric bone unites by three weeks). Residual angulation remodels; rotation does not. Complications
- Recognition
- Pain out of proportion, pain with passive finger extension, tense forearm, rising analgesia needs. The 5 Ps are LATE signs.
- Prevention
- Avoid flexion greater than 90 degrees; overnight monitoring; liberal splint removal; parent education on warning signs.
- Management
- CLINICAL diagnosis - do NOT wait for pressures. Emergent volar (Henry) and dorsal forearm fasciotomy. Later: tendon transfers and contracture release.
- Recognition
- Post-op ulnar sensory or motor deficit; claw hand if severe. Usually neurapraxia.
- Prevention
- Identify the nerve before a medial pin; reduce flexion; palpate or visualise during insertion. Prefer lateral-only fixation.
- Management
- Most neurapraxias resolve in 3 to 6 months with serial EMG. Transection: immediate repair. Late: tendon transfers.
- Recognition
- Progressive varus noted at follow-up; cosmetic concern, usually no functional deficit.
- Prevention
- Meticulous rotational reduction; check Baumann angle versus contralateral (a difference greater than 5 degrees is malreduction).
- Management
- If greater than 15 degrees and symptomatic: lateral closing-wedge osteotomy after skeletal maturity. It does NOT remodel.
- Recognition
- Weekly radiographs show pin migration, fragment displacement, increasing deformity.
- Prevention
- Bicortical purchase, adequate pin spread, confirm reduction intraoperatively; weekly radiographs for 3 weeks.
- Management
- If less than 1 week: return to theatre for re-reduction. If more than 1 week: accept, correct later if needed.
- Recognition
- Erythema, discharge, warmth at pin sites; usually superficial.
- Prevention
- Sterile technique, antiseptic dressing, remove pins at 3 to 4 weeks, avoid pin motion.
- Management
- Superficial: oral antibiotics. Deep: remove pins, IV antibiotics, irrigation and debridement if abscess.
- Recognition
- Weak OK sign (thumb IP plus index DIP flexion). Usually from the injury, not the surgery.
- Prevention
- Document pre-operatively; gentle reduction; minimise anterior dissection.
- Management
- Most resolve spontaneously in 3 to 6 months. EMG at 6 to 8 weeks. Exploration rarely indicated.
Viva & Exam Focus
G-A-R-T-L-A-N-DGARTLAND - the classification that drives management
P-I-N-SPINS - pin configuration decisions
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 6-year-old presents with a displaced supracondylar fracture and an absent radial pulse but pink, warm fingers. How do you manage this?”
“Describe your pin configuration for a Gartland III supracondylar fracture. What are the pros and cons of different configurations?”
“Post-operatively, the parents call concerned that their child is in increasing pain and cannot move their fingers. What is your approach?”
Key indications
- Gartland IIB and III supracondylar fractures
- Failed closed reduction (Gartland IIA)
- Vascular compromise requiring exploration
- Open fracture requiring debridement
- Floating elbow (ipsilateral forearm fracture)
Critical steps
- CRPP is the standard - closed reduction (traction, then flex and pronate for extension fractures)
- C-arm as the operating surface: AP, lateral and both obliques are essential
- Pin configuration: two to three lateral divergent pins default; medial pin only if needed
- Open reduction (anterior approach) only if irreducible, open, or white/cold hand
- Confirm anterior humeral line through the middle third of the capitellum
- Splint at 60 to 90 degrees flexion (NOT greater than 90 degrees) - stability is from the pins
Danger zones
- Brachial artery - anterior, kinked by flexion
- Ulnar nerve - cubital tunnel, medial pin risk
- Median nerve - anterior, avoid excessive dissection
- AIN - document pre-operatively, usually injury not iatrogenic
- Radial nerve - lateral and proximal dissection risk
Exam-day pearls
- Gartland classification drives ALL management decisions
- Baumann angle 65 to 75 degrees - compare to contralateral
- Anterior humeral line through the middle third of the capitellum
- Cubitus varus equals rotational malreduction (does NOT remodel)
- Pulseless pink hand equals controversial - close observation versus explore
- Compartment syndrome is a CLINICAL diagnosis - do not wait for pressures
Pin configuration decision
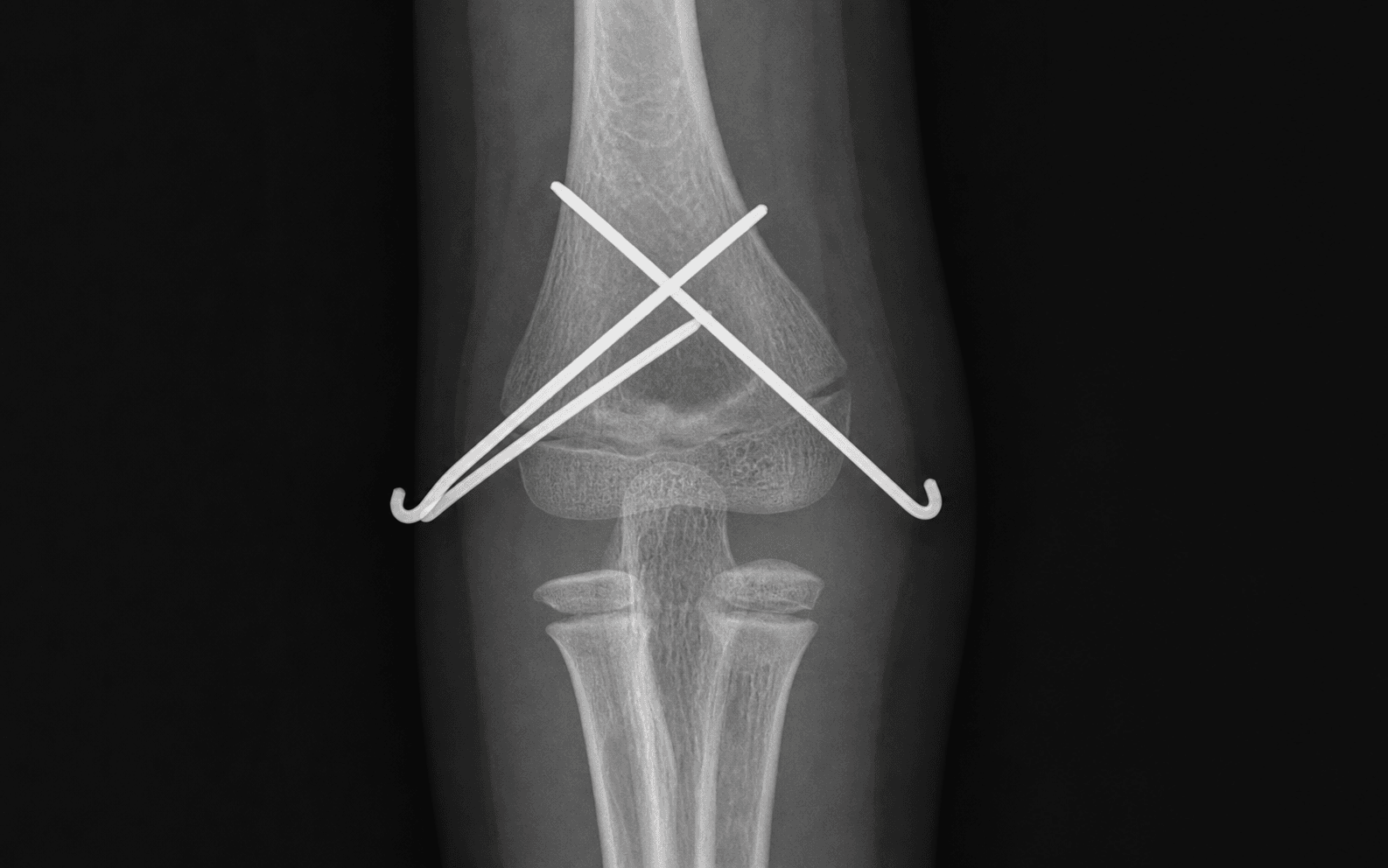
- Two lateral divergent: preferred - good stability, no ulnar nerve risk
- Crossed pins: best torsional stability but added ulnar nerve risk (medial pin)
- Three lateral pins: unstable or comminuted fractures - low threshold for the third pin
- Medial pin: REDUCE flexion first, mini-open, see or palpate the ulnar nerve
Complications to know
- Compartment syndrome then Volkmann contracture (devastating, medicolegal)
- Cubitus varus: most common - rotational malreduction
- Iatrogenic ulnar nerve injury: medial pin technique is critical
- AIN palsy: usually from the injury, 90 percent recover spontaneously
Post-operative protocol
- Above-elbow splint at 60 to 90 degrees flexion
- Overnight hourly neurovascular monitoring
- Weekly radiographs for 3 weeks
- Pin removal at 3 to 4 weeks in clinic
- Full ROM expected by 6 to 8 weeks
Key numbers
- Baumann angle: 65 to 75 degrees (compare contralateral)
- Splint position: 60 to 90 degrees flexion (NOT greater than 90 degrees)
- Pin removal: 3 to 4 weeks
- Union: 3 weeks in children
- Full recovery: 6 to 8 weeks typical
Background & Evidence
Pathoanatomy. A paediatric supracondylar fracture is most often an extension injury from a fall onto the outstretched hand with the elbow hyperextended - the olecranon levers the distal fragment posteriorly. In the typical extension fracture the posterior periosteum remains intact and acts as the reduction hinge (tensioned by flexion and pronation), while the anterior periosteum and brachialis are torn; the distal fragment displaces posteriorly and proximally, dragging the neurovascular bundle across the sharp anterior metaphyseal spike - which is why the brachial artery and the median and AIN nerves are the structures injured. The rarer flexion-type injury is the mirror image: the anterior periosteum is intact and the ulnar nerve is the one most at risk. The modified Gartland classification drives every management decision:
- Description
- Undisplaced or minimally displaced
- Posterior cortex
- Intact
- Management
- Above-elbow cast for 3 weeks
- Description
- Displaced, angulated
- Posterior cortex
- Intact (acts as a hinge)
- Management
- Closed reduction and percutaneous pinning
- Description
- Displaced, rotated
- Posterior cortex
- Intact
- Management
- Closed reduction and pinning (may need open)
- Description
- Completely displaced
- Posterior cortex
- Disrupted
- Management
- Closed reduction and pinning (open if irreducible)
- Description
- Multidirectionally unstable - incompetent periosteum circumferentially
- Posterior cortex
- Unstable in flexion AND extension
- Management
- Closed reduction and pinning (reduce under fluoro in both flexion and extension)
Key radiographic parameters. On the lateral view, the anterior humeral line should pass through the middle third of the capitellum; if it passes anterior to the capitellum there is extension (posterior tilt) malreduction, and posterior to it, flexion malreduction (rare). On the AP view, Baumann angle - the angle between the humeral shaft and the capitellar physis - is 65 to 75 degrees; compare with the contralateral limb, where a difference greater than 5 degrees indicates rotational malreduction. The normal carrying angle is 5 to 15 degrees of valgus. Intra-operatively, obtain all four views (AP, lateral, medial oblique and lateral oblique), confirm the pins engage both cortices, and exclude intra-articular pin placement. Rotational malreduction is the most common cause of cubitus varus - and rotation cannot remodel, which is why a meticulous reduction matters more than the pin configuration.
References
Lateral-entry pin fixation in the management of supracondylar fractures in children
- 124 consecutive displaced supracondylar fractures (Gartland II and III) fixed with lateral-entry pins ONLY
- No loss of reduction, no cubitus varus and NO iatrogenic ulnar nerve injuries in the whole series
- Eight referred failures of lateral pinning were all due to technical errors, not the configuration itself
- Defined the four technical points: maximise pin spread, engage both columns, adequate bone in each fragment, low threshold for a third pin
Nerve injuries associated with pediatric supracondylar humeral fractures: a meta-analysis
- 5148 patients pooled; traumatic neurapraxia occurred at a weighted rate of 11.3 percent
- Anterior interosseous nerve injury predominated in extension-type fractures (34.1 percent of associated palsies)
- Ulnar neuropathy predominated in flexion-type injuries (91.3 percent of associated palsies)
- Iatrogenic palsy 3.4 percent with lateral-only versus 4.1 percent when a medial pin was added; medial pinning specifically raised ulnar nerve risk
Treatment of multidirectionally unstable supracondylar humeral fractures in children: a modified Gartland type-IV fracture
- Described Gartland type IV: fractures unstable in BOTH flexion and extension (incompetent periosteum circumferentially)
- Nine such fractures from 297 displaced injuries, all treated successfully by closed reduction and percutaneous pinning
- No nonunion, cubitus varus, malunion, loss of motion or need for further surgery
- Closed pinning avoided open reduction even in the most unstable pattern
Ischaemia and the pink, pulseless hand complicating supracondylar fractures of the humerus in childhood: long-term follow-up
- 26 children referred with a pink pulseless hand after supracondylar fracture, followed for a mean of 15.5 years
- 23 of 26 presented with established ischaemic (Volkmann) contracture because exploration had been delayed
- Authors recommend URGENT exploration of vessels and nerves when the pink pulseless hand is not relieved by reduction and there is persistent or increasing pain or a deepening nerve lesion
- Highlights that median or AIN dysfunction with pain signals critical ischaemia, not a benign collateralised limb
AAOS Clinical Practice Guideline: The Treatment of Pediatric Supracondylar Humerus Fractures
- Displaced (Gartland II and III) fractures should be treated operatively with closed reduction and percutaneous pinning
- Lateral pin entry is supported; if a medial pin is used, technique should minimise ulnar nerve risk
- Non-operative treatment is reserved for non-displaced (type I) fractures
- Reflects consensus across global practice (AAOS, BOA and BOAST, AO) that CRPP - not routine open ORIF - is the standard of care