Fresh cadaveric transplant · Large lesions over 4cm² · Mature hyaline cartilage in a single stage
- OCA is the only cartilage restoration option that transfers mature hyaline cartilage with its subchondral bone in a single stage, making it first-line for large defects, failed prior cartilage surgery and lesions with bone loss.
- Fresh (not frozen) graft is essential — fresh allograft stored at 4°C keeps living chondrocytes; freezing destroys the cells (less than 1% viability).
- Optimal implantation is within 28 days of harvest, and the graft must be size-matched to the recipient through a tissue bank.
- No donor-site morbidity, and unlike OATS or ACI it restores subchondral bone stock.
- Survival depends on correcting the mechanical environment — malalignment, ligament and meniscal deficiency must be addressed or the graft will fail.
When & Why
OCA is the only cartilage restoration option that transfers large volumes of mature hyaline cartilage together with its subchondral bone in a single operation. It fills a critical niche for defects that are too large for autograft, have failed previous cartilage surgery, or involve bone loss — and it does so without donor-site morbidity.
OCA uniquely restores both hyaline cartilage and subchondral bone in one stage. Understanding fresh versus frozen tissue and the narrow storage window is what examiners test.
Indications and contraindications
- Large lesions over 4cm² that exceed OATS donor capacity - Failed prior cartilage surgery (OATS, microfracture, ACI) - Osteonecrosis with cartilage damage - Post-traumatic defects with bone loss - Bipolar (kissing) lesions (selected cases) - Young patients unsuitable for arthroplasty
- Diffuse osteoarthritis - Inflammatory arthropathy - Active infection - Uncorrected malalignment - Non-compliant patient - Unrealistic expectations
Clinical assessment
- Prior cartilage surgery (failed OATS, microfracture, ACI) - Large traumatic defect - Osteonecrosis symptoms (night pain, rest pain) - Mechanical symptoms (catching, locking, swelling) - Activity level and expectations
- Joint effusion — often present - Crepitus — may indicate cartilage damage - Tenderness — localized to the affected compartment - Alignment — assess for malalignment - Stability — rule out ligamentous insufficiency
Before OCA, assess and address every contributing factor: malalignment (osteotomy), ligament insufficiency (reconstruction) and meniscal deficiency (meniscal allograft or preservation). An OCA placed into a malaligned, unstable or meniscal-deficient knee will fail.
Investigations and sizing
Investigation protocol
Weight-bearing AP, lateral, Rosenberg and skyline views. Assess joint space, alignment, osteoarthritic change and subchondral bone. Sizing films are sent to the tissue bank for donor matching.
Defines lesion size and location, subchondral bone status (oedema, cysts, avascular necrosis), bone-marrow lesion extent and any associated meniscal or ligament pathology.
Precise donor-recipient size matching; 3D reconstruction helps with complex defects and confirms available bone stock.
Tissue banks use CT or X-ray measurements to match donor to recipient. The graft should be matched to within 2-3mm. An oversized graft can be trimmed; an undersized graft cannot fill the defect adequately.
Choosing OCA over other cartilage procedures
- OCA
- Over 4cm²
- OATS
- 1-4cm²
- ACI/MACI
- Over 2cm²
- OCA
- Hyaline (Type II)
- OATS
- Hyaline (Type II)
- ACI/MACI
- Hyaline-like
- OCA
- Single
- OATS
- Single
- ACI/MACI
- Two
- OCA
- None (allograft)
- OATS
- 10-15%
- ACI/MACI
- None (biopsy only)
- OCA
- Restores bone
- OATS
- Transfers with plug
- ACI/MACI
- Requires intact bone
- OCA
- Limited (tissue bank)
- OATS
- Immediate (patient)
- ACI/MACI
- Requires cell culture
Choose OCA when the lesion is over 4cm² (exceeding OATS capacity), prior cartilage surgery has failed, there is bone loss or avascular necrosis, the lesion is bipolar, or the patient is young and unsuitable for arthroplasty. Choose OATS for a single 1-4cm² lesion without bone loss where timing is critical. Choose ACI/MACI for a large lesion without bone loss when OCA is unavailable or the patient prefers autologous tissue. Concomitant procedures
- Procedure
- HTO or DFO
- Timing
- Staged or concurrent
- Procedure
- ACL reconstruction
- Timing
- Concurrent or staged
- Procedure
- Meniscal allograft
- Timing
- Concurrent preferred
- Procedure
- PCL reconstruction
- Timing
- Usually staged
Pre-operative coordination with the tissue bank
Pre-operative steps
Contact the tissue bank, provide sizing imaging (CT/X-ray) and request a size-matched graft. Confirm availability and timing.
Confirm graft arrival and harvest date. Verify it is within the storage window (under 28 days from harvest) and review the donor screening documentation.
Prepare the graft bench, have a back-up plan if the graft proves unsuitable intra-operatively, and confirm standard arthroscopy and open equipment.
Fresh OCA should be implanted within 28 days of harvest for optimal chondrocyte viability; beyond this, viability falls significantly. The window is rigid — the patient and operating room must be available when the graft arrives.
The Operation
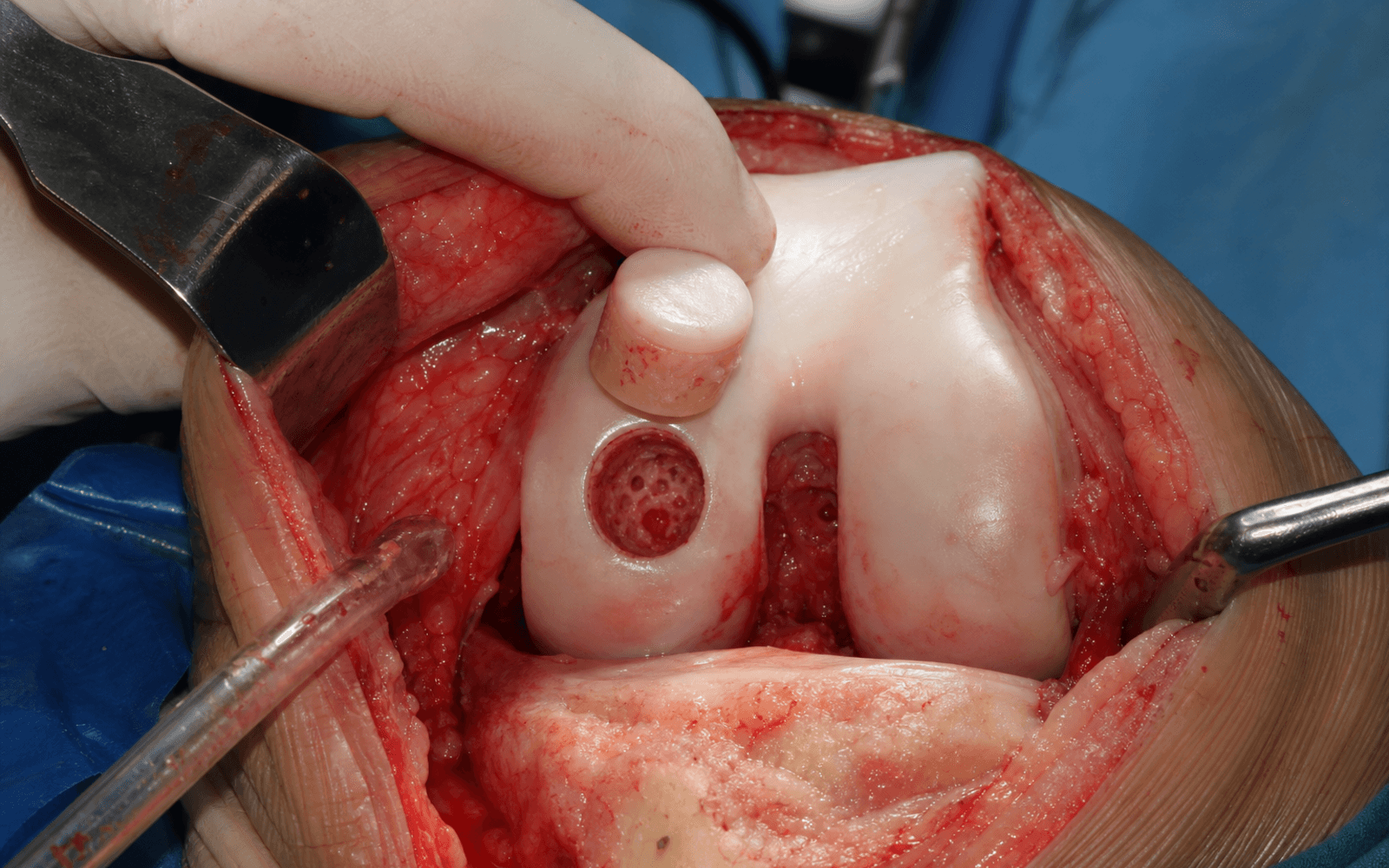
The goal is to expose the defect through a mini-open (usually medial or lateral parapatellar) approach, prepare a perpendicular recipient socket that matches the graft geometry, harvest and contour a size-matched fresh allograft dowel, and seat it flush so that living hyaline cartilage and subchondral bone are transferred in one stage. The exposure and the dowel/plug technique form the backbone; shell and hemicondylar variants are adaptations for larger or more complex defects.
Fresh OCA stored at 4°C maintains chondrocyte viability for the storage window; frozen graft stored at -80°C has less than 1% viability because freezing destroys the cells. Only fresh allograft is used for cartilage restoration — frozen allograft is structural bone only.
Operative sequence (dowel / plug technique)
- Supine with a thigh-side support and a lateral post as needed; upper-thigh tourniquet.
- Standard knee arthroscopy set-up plus the allograft instrumentation and graft on the back table; confirm the graft is within the storage window before draping.
- Examine the whole joint — confirm lesion size and location, assess the menisci, ligaments and opposing articular surface, and exclude diffuse degeneration that would contraindicate the graft.
- Measure the defect and plan the graft geometry (dowel for a contained circular or oval lesion, shell for a larger or irregular defect).
- A mini-open approach is typical: a medial parapatellar arthrotomy for medial femoral condyle lesions, lateral for lateral condyle — whichever gives perpendicular access to the defect (see the medial parapatellar approach to the knee).
- The exposure must be adequate for the sizing corer and graft instrumentation; a modest arthrotomy with the knee flexed to deliver the condyle usually suffices.
- Mark the lesion boundaries.
- Use a recipient sizing corer to create a cylindrical socket perpendicular to the articular surface, matching depth to the available graft depth and aiming for a stable, intact rim of surrounding cartilage.
- Harvest the dowel from the size-matched allograft condyle using a matching corer, matching articular curvature and orientation to the recipient.
- Trim the cancellous bone depth to match the recipient socket so the graft will seat flush.
- Insert the graft into the recipient site; press-fit is usually sufficient. The graft should be flush or 1mm proud — never recessed below the surrounding cartilage.
- If the graft is unstable, add bioabsorbable pins; avoid metal hardware where possible.
- Confirm graft stability and congruity through a full range of motion.
- Layered closure over a drain if needed; release the tourniquet and obtain haemostasis. Apply a bulky dressing and a brace locked for transfer.
Handle the articular surface gently and keep it moist with saline throughout. Minimise tourniquet time and do not compress or traumatise the cartilage during insertion — the living chondrocytes are the whole point of the procedure.
The graft must sit flush with the surrounding articular surface or at most 1mm proud. A recessed graft leaves a step-off that concentrates load and fails; an excessively proud graft catches and delaminates. Press-fit is usually enough; add bioabsorbable pins only if the graft is unstable.
Larger or irregular defects. The same principles — perpendicular fit, flush seating, secure fixation — extend to a shell graft (a thin cartilage-bone slice over a shallow 5-10mm bed, fixed with bioabsorbable pins or headless screws, which preserves recipient bone stock and allows custom shaping) and to hemicondylar grafts for massive defects (rigid plate-and-screw fixation, longer rehabilitation, higher failure rate). The full graft-geometry classification is detailed under Background & Evidence.
Aftercare & Complications
Weight-bearing and rehabilitation Rehabilitation is longer than after OATS because the deeper bone graft needs more time to integrate. Hemicondylar grafts may need 3-4 months of protection before full weight-bearing.
Weight-bearing progression
Strict non-weight-bearing or toe-touch only. Longer protection than OATS because of the deeper bone integration required.
Progressive weight-bearing from 25% to 75%; crutches continued.
Wean from crutches; full weight-bearing by 16 weeks, continuing to avoid impact.
OCA rehabilitation is longer than OATS because deeper bone grafts need more time to integrate. Hemicondylar grafts may need 3-4 months of protection before full weight-bearing.
Return to activity
Activity progression
Swimming, cycling, elliptical. No running or jumping.
Jogging progression; sport-specific drills begin.
Return to sport if criteria are met — longer than after OATS or microfracture. Consider permanent activity modification for large grafts.
Outcomes and prognosis
- Survivorship
- 85-90%
- Considerations
- Good early results expected
- Survivorship
- 75-85%
- Considerations
- Progressive decline begins
- Survivorship
- 65-75%
- Considerations
- Can act as a bridge to arthroplasty
In young patients unsuitable for arthroplasty, OCA can delay TKA by 10-15 years on average. Even if the graft eventually fails it preserves bone stock and still allows eventual arthroplasty — a valuable strategy in patients too young for definitive replacement.
Complications
- Incidence
- 10-15% at 10 years
- Risk factors
- Large or deep grafts, poor integration
- Prevention / management
- Protect weight-bearing, optimise biology
- Incidence
- Very rare
- Risk factors
- Inadequate donor screening
- Prevention / management
- Rigorous donor screening protocols
- Incidence
- 5-10%
- Risk factors
- Deep grafts, poor vascularity
- Prevention / management
- Protected loading, avoid smoking
- Incidence
- 5-10%
- Risk factors
- Early loading, poor bone quality
- Prevention / management
- Extended non-weight-bearing for deep grafts
- Incidence
- Rare for cartilage
- Risk factors
- Deep bone grafts
- Prevention / management
- Cartilage is immune-privileged
Disease transmission is possible with any allograft, though very rare. All donors undergo rigorous screening — serology, nucleic-acid testing, culture and medical-history review. HIV and hepatitis C transmission have been reported historically but are extremely rare with modern protocols.
Viva & Exam Focus
FRESHFRESH — why fresh matters
LARGELARGE — when to use OCA
Exam viva scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old man has a 5cm² full-thickness cartilage defect on the medial femoral condyle after failed microfracture two years ago. What are your treatment options?”
“Why do we use fresh osteochondral allograft rather than frozen, and what are the storage considerations?”
“A 35-year-old has bipolar (kissing) lesions on the medial femoral condyle and tibial plateau after a failed HTO. What are your options?”
Definition
- Fresh cadaveric osteochondral graft
- Bone plus hyaline cartilage transplant
- Living chondrocytes preserved
- Single-stage procedure
Fresh versus frozen
- Fresh at 4°C = over 70% viability
- Frozen at -80°C = under 1% viability
- Fresh essential for cartilage restoration
- 28 days optimal storage window
Indications (LARGE)
- Large lesions over 4cm²
- AVN or bone loss present
- Revision after failed cartilage surgery
- Geometric matching from tissue bank
- Extensive defects (bipolar, hemicondylar)
Key numbers
- Over 4cm² = typical size indication
- 28 days = quoted fresh storage window at 4°C
- Over 70% = commonly-taught fresh chondrocyte viability
- 82% = femoral-condyle survivorship at 10 years (Levy 2013)
- Bipolar grafts = clearly worse than unipolar
Advantages
- Mature hyaline cartilage (Type II)
- Single-stage surgery
- No donor-site morbidity
- Restores bone stock
- Large-lesion capability
Disadvantages
- Limited availability
- Narrow storage window
- Disease-transmission risk (rare)
- Logistical coordination required
- Higher cost than autograft
- Storage temperature? 4°C (refrigerated, in nutrient medium) — never frozen for cartilage restoration.
- Viability of fresh OCA at 28 days? Over 70% (commonly taught); note superficial-zone viability already declines beyond about 2 weeks at 4°C.
- Viability of frozen OCA? Less than 1% — freezing destroys chondrocytes.
- Typical lesion size? Over 4cm², where OATS donor capacity is exceeded.
- 10-year survivorship? 75-85% overall; 82% for femoral-condyle grafts (Levy 2013).
- Bipolar versus unipolar? Substantially worse — bipolar grafting is a recognised predictor of failure.
Background & Evidence
Why fresh matters — chondrocyte viability Cartilage restoration depends on living chondrocytes maintaining the matrix, which is why only fresh allograft is used.
- Fresh (4°C)
- Over 70% at 28 days
- Frozen (-80°C)
- Less than 1%
- Fresh (4°C)
- Preserved
- Frozen (-80°C)
- Preserved
- Fresh (4°C)
- 14-28 days optimal
- Frozen (-80°C)
- Years
- Fresh (4°C)
- Limited, requires coordination
- Frozen (-80°C)
- Readily available
- Fresh (4°C)
- Yes — living cartilage
- Frozen (-80°C)
- No — structural only
- Avascular — no access for immune cells - Chondrocytes encased in matrix - Low immunogenicity of cartilage matrix - Bone is immunogenic — deeper grafts may generate a response
- Bone-to-bone healing: 8-12 weeks - Cartilage: minimal integration (fibrocartilaginous junction) - Subchondral bone remodels over 1-2 years - Deeper grafts integrate more slowly
Graft-geometry classification and common locations
- Description
- Cylindrical grafts (like a large OATS)
- Best for
- Contained circular or oval lesions
- Description
- Thin cartilage-bone slice over a shallow bed (5-10mm)
- Best for
- Large surface lesions, good bone stock
- Description
- Entire condylar surface
- Best for
- Massive defects, failed TKA salvage
- Description
- Both articulating surfaces
- Best for
- Tibial plus femoral kissing lesions
- Considerations
- Most common, good access
- Technique
- Dowel or shell
- Considerations
- Match curvature carefully
- Technique
- Dowel or shell
- Considerations
- Requires precise contouring
- Technique
- Shell often better
- Considerations
- Technically challenging
- Technique
- Shell graft
- Considerations
- Uncommon, difficult access
- Technique
- Dowel or shell
Global availability and regulation
- Fresh OCA availability is limited everywhere because of the narrow storage window - Tissue must come from an accredited bank: AATB (US), and national tissue authorities or EU Tissue Directive standards elsewhere - Some regions import grafts from US tissue banks where domestic supply is scarce - Cost and logistics are universal barriers - When fresh OCA is unavailable: OATS (smaller lesions) or ACI/MACI (no bone loss)
- Document graft harvest date and storage duration - Record donor screening documentation - Document surgical technique and fixation - Consent must include disease-transmission risk - Record the size-matching process
Consent must cover disease-transmission risk (very low but real), the potential for failure and conversion to TKA, and realistic sport expectations. Document the graft arrival and harvest date (confirm within window), record that donor screening was reviewed, and note the storage and surgical technique — if the graft fails early, this documentation is protective.
References
OCA long-term survivorship of the femoral condyle
- 129 knees, median 13.5-year follow-up: graft survivorship 82% at 10 years, 74% at 15 years, 66% at 20 years
- Graft failure (revision OCA or arthroplasty) in 24%; reoperation in 47%
- Age over 30 at surgery and two or more prior surgeries on the knee predicted failure
- Modified Merle d'Aubigne-Postel and IKDC pain and function scores improved durably
Storage temperature and chondrocyte viability
- At 4°C, chondrocyte viability fell to about 45% en face and only about 20% in the vulnerable superficial zone by 28 days
- Storage at 37°C maintained much higher viability at 28 days (about 80% surface, about 65% superficial zone)
- Cartilage thickness, glycosaminoglycan and collagen content were preserved at both temperatures
- Cell viability deteriorates faster than matrix — the matrix outlasts the living cells
OCA for steroid-associated femoral condyle osteonecrosis
- 28 knees (mean age 24 years, mean graft area 10.8 cm²), mean follow-up 67 months
- Graft survival 89% (25 of 28); 76% scored over 15 on the modified d'Aubigne-Postel scale
- IKDC pain and function and Knee Society scores improved markedly
- Arthroplasty was avoided in 27 of 28 knees at last follow-up
Return to sport after OCA
- 43 athletes (mean age 33), mean 2.5-year follow-up
- Limited return to sport in 88% (38 of 43); full return to pre-injury level in 79% (34 of 43)
- Mean time to return to sport 9.6 months
- Age 25 years or older and symptom duration over 12 months reduced the chance of return
Fresh OCA for post-traumatic knee defects
- 60 femoral-condyle grafts: 95% survival at 5 years, 85% at 10 years
- 65 tibial-plateau grafts: 95% at 5 years, 80% at 10 years, 65% at 15 years
- Failures were salvaged by graft removal or conversion to total knee arthroplasty
- Durable joint preservation in young, active post-traumatic patients