Open reduction internal fixation of displaced transverse patellar fractures · intermediate
- Indications for surgery: articular step-off greater than 2 mm, fracture gap greater than 3 mm, loss of active knee extension, or extensor mechanism discontinuity. Minimally displaced fractures (step-off less than 2 mm with an intact extensor mechanism) are managed non-operatively with a cylinder cast or hinged brace in extension for 4 to 6 weeks.
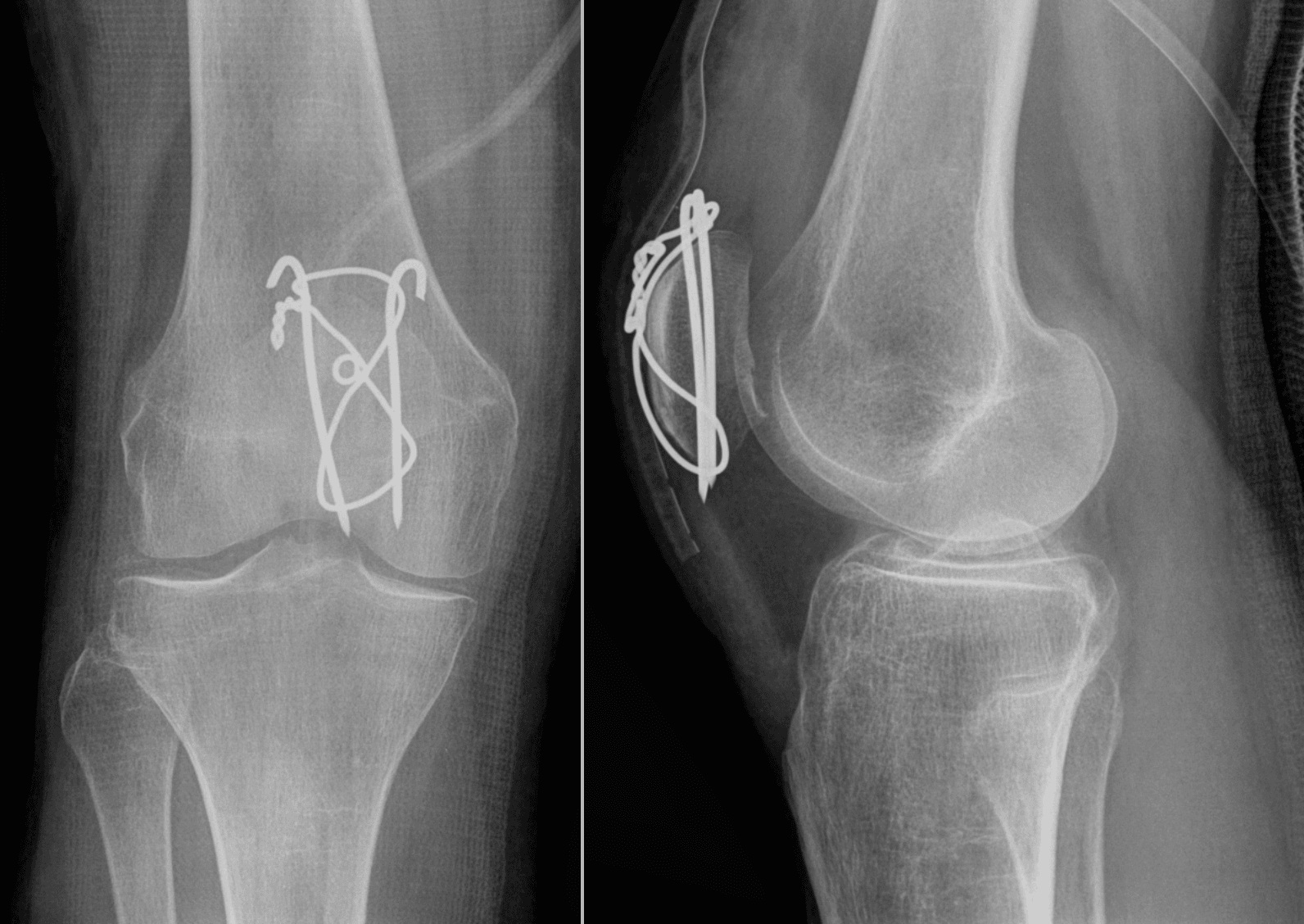
- The modified anterior tension-band principle converts the distractive force of the quadriceps into compressive force across the fracture during knee flexion. Parallel longitudinal K-wires or cannulated screws placed in the anterior half of the patella act as a fulcrum; the figure-of-eight wire anterior to the patella tightens with flexion and compresses the articular surface.
- Anatomic reduction of the articular surface must be confirmed by direct visualisation of the retropatellar surface through the fracture or via a small arthrotomy. Intra-operative fluoroscopy alone is insufficient — a residual step-off greater than 2 mm increases the risk of post-traumatic arthritis.
- Hardware prominence requiring removal occurs in 20 to 50 percent of tension-band cases. Use low-profile constructs, bury K-wire ends, and consider cannulated screw tension-band constructs in patients with thin soft-tissue envelopes to reduce the re-operation rate.
- “The patella is a sesamoid bone within the extensor mechanism — the quadriceps tendon inserts proximally and the patellar tendon distally. Preserve as much patellar bone stock as possible; partial patellectomy is reserved for comminuted inferior or superior pole fractures where stable fixation cannot be achieved.
- “The modified anterior tension band is biomechanically superior to cerclage wiring alone. The anterior figure-of-eight wire must pass through or around the K-wires or screws and be tensioned so that knee flexion produces compression rather than gapping at the articular surface.
- “The inferior pole is a common site of comminution in high-energy injuries. When the inferior pole fragment is too small for fixation, perform a partial patellectomy and reattach the patellar tendon to the remaining patella with transosseous sutures or anchors.
- “Post-operative rehabilitation begins with immediate quadriceps setting and straight-leg raises in a hinged brace locked in extension. Active knee flexion is introduced gradually after radiographic evidence of healing (usually 6 weeks) to avoid fixation failure.
When & Why
Indications. Operative fixation is reserved for fractures that disrupt the articular surface or the extensor mechanism. Absolute indications
- Articular step-off greater than 2 mm or fracture gap greater than 3 mm on radiographs or CT
- Loss of active knee extension (inability to perform a straight-leg raise)
- Open patellar fracture requiring debridement and stabilisation
- Displaced fracture with significant displacement of the extensor mechanism
- Associated ipsilateral injuries requiring surgical stabilisation (tibial plateau, distal femur) Relative indications
- Minimally displaced fracture (step-off less than 2 mm) with preserved active extension but patient preference for early mobilisation
- Athletes or high-demand patients where anatomic reduction may improve long-term function
- Comminuted fractures where partial patellectomy and tendon reattachment can restore a functional extensor mechanism Contraindications. Absolute: a minimally displaced fracture with intact active extension and acceptable alignment (managed non-operatively); a patient medically unfit for surgery; or a chronic non-union with established post-traumatic arthritis where salvage (patellectomy or arthroplasty) is more appropriate. Relative: severe soft-tissue compromise requiring delayed definitive fixation; a low-demand elderly patient with comorbidities in whom extension bracing is acceptable; or a vertical fracture pattern better suited to lag screw fixation alone. Operative versus non-operative. Non-operative care is indicated for a step-off less than 2 mm with an intact extensor mechanism — a cylinder cast or hinged brace locked in extension for 4 to 6 weeks followed by progressive mobilisation gives good to excellent results in 70 to 85 percent of appropriately selected fractures, with a risk of late displacement if bracing compliance is poor. Operative treatment restores articular congruity and allows early mobilisation: modified anterior tension-band wiring achieves union greater than 90 percent in transverse fractures, cannulated screw tension-band constructs show lower rates of hardware prominence and re-operation, and partial patellectomy restores extension with acceptable function when at least 50 percent of patellar height is preserved. The fixation decision. Once you have decided to operate, the pattern dictates the construct:
The benchmark for a transverse mid-patella fracture: parallel anterior K-wires plus a figure-of-eight wire. Union greater than 90 percent in transverse patterns, at the cost of a 20 to 50 percent rate of hardware removal.
For thin soft-tissue envelopes or high-demand patients: 4.0 to 4.5 mm cannulated screws carry the figure-of-eight wire through the screw heads. Lower profile and a lower re-operation rate for hardware irritation.
For a comminuted pole that cannot be reconstructed: excise the fragments and reattach the tendon with transosseous sutures or anchors, preserving at least 50 percent of patellar height.
Setup. Supine on a radiolucent table with a bump under the ipsilateral hip; flex the knee 30 to 40 degrees over a radiolucent triangle or bump to relax the extensor mechanism. A thigh tourniquet is applied but inflated only if needed for visualisation. Regional (spinal or femoral–sciatic block) or general anaesthesia, with a femoral nerve or adductor canal block for post-operative analgesia. Position the image intensifier for AP, lateral and sunrise views so the C-arm can rotate freely around the knee without repositioning the patient. Consent specifically for hardware prominence requiring removal (20 to 50 percent), loss of reduction, non-union (less than 5 percent), infection (1 to 2 percent), extensor lag, post-traumatic arthritis, and the possible need for a future salvage procedure.
The Operation
The goal is an anatomic, stable reduction of the articular surface that lets the knee move early while the fracture unites. The modified anterior tension-band principle makes this possible: during flexion the quadriceps exerts a distractive force across a transverse fracture, but longitudinal implants placed in the anterior half of the patella act as a fulcrum, and the figure-of-eight wire lying anterior to that fulcrum tightens and converts the distractive force into articular compression. This works only when the implants are anterior and the wire is tensioned with the knee in extension before flexion is tested. The exposure is the standard midline anterior approach, laid out step by step below (and in depth on the medial parapatellar approach to the knee page).
Operative sequence
- Supine, radiolucent table, ipsilateral hip bump, knee flexed 30 to 40 degrees over a triangle; tourniquet ready but not routinely inflated.
- Mark the landmarks — the superior and inferior poles of the patella and the tibial tubercle — before incision, because swelling distorts the surface anatomy.
- Make a longitudinal midline incision centred over the patella from the superior pole to the tibial tubercle; curve it slightly medially or laterally to avoid an open wound or skin contusion.
- Raise full-thickness skin flaps medially and laterally to expose the fracture and the extensor retinaculum — thin flaps devascularise the skin edges and necrose.
- Identify and protect the infrapatellar branch of the saphenous nerve when it is encountered; injury leaves a permanent numb patch lateral to the incision.
- Expose the fracture line, the quadriceps tendon proximally and the patellar tendon distally; palpate for gaps or discontinuity.
- If a concomitant tendon rupture is suspected, extend the exposure proximally or distally to visualise the entire extensor mechanism — a missed quadriceps or patellar tendon rupture causes early fixation failure.
- Evacuate the fracture haematoma. For a transverse fracture the two main fragments can often be hinged open to visualise the retropatellar surface directly.
- If visualisation is inadequate, make a small medial or lateral arthrotomy to allow direct inspection and palpation of the articular surface; remove loose osteochondral fragments that cannot be reconstructed.
- Use pointed (Weber) reduction clamps on the superior and inferior poles; for a transverse fracture a clamp placed across the fracture in the coronal plane gives excellent control.
- Confirm reduction by direct palpation of the articular surface (a finger or Freer elevator on the retropatellar cartilage) and with fluoroscopy — never rely on fluoroscopy alone.
- Place two parallel 1.6 mm or 2.0 mm K-wires longitudinally from superior to inferior pole, positioned in the anterior half of the patella.
- The wires must be parallel in both planes and spaced about one-third of the patellar width apart; confirm the position with fluoroscopy before tension-banding.
- Pass an 18-gauge stainless-steel wire in a figure-of-eight around the K-wires, through the quadriceps tendon proximally and the patellar tendon distally (or through drill holes in the poles if the tendon attachments are tenuous).
- Tighten the wire with the knee in extension, then gently flex the knee to 90 degrees while watching the fracture — the wire should tighten and compress the articular surface, never gap.
- For thin soft-tissue envelopes or high functional demand, use 4.0 mm or 4.5 mm cannulated screws instead of K-wires: drill over the provisional K-wires, measure and insert partially threaded screws.
- Pass the tension-band wire through the screw heads (or around the screws) in a figure-of-eight — a lower-profile construct with a lower re-operation rate for hardware removal.
- When the inferior (or superior) pole is severely comminuted and cannot be reconstructed, excise the comminuted fragments.
- Reattach the patellar (or quadriceps) tendon to the remaining patella with heavy non-absorbable transosseous sutures through drill holes or with suture anchors; ensure at least 50 percent of the original patellar height remains to preserve the extensor lever arm.
- Obtain AP, lateral and sunrise fluoroscopic views; confirm anatomic articular reduction, appropriate implant position and no gapping with flexion.
- Irrigate, achieve haemostasis, close the retinaculum with absorbable suture and close the skin in layers; apply a sterile dressing and a hinged knee brace locked in extension.
Mark the patellar poles and the tibial tubercle before incision so the landmarks remain identifiable even after swelling distorts the surface anatomy. Raise full-thickness skin flaps to preserve the blood supply to the skin edges — thin flaps necrose and lead to wound complications.
Inadvertent injury to the infrapatellar branch of the saphenous nerve causes a permanent numb patch lateral to the incision — counsel patients pre-operatively. Thin skin flaps in a contused knee lead to marginal necrosis, and extending the incision too far distally in a swollen knee risks the patellar tendon insertion.
Keep a finger or a Freer elevator on the retropatellar surface while reducing the fracture so you can feel that the articular cartilage is flush before placing any hardware. If the surfaces cannot be matched, accept that partial patellectomy may be the better option.
Pass the tension-band wire through the substance of the quadriceps and patellar tendons rather than drilling extra holes — this preserves bone stock and avoids stress risers. Tighten the wire with the knee extended, then test flexion to 90 degrees; if the fracture gapes, re-tension or reposition the wire.
Placing the longitudinal implants too posteriorly — in the articular half of the patella — abolishes the tension-band effect and the construct fails in flexion. Over-tightening the wire with the knee already flexed leaves the construct too tight in extension, and leaving sharp K-wire ends or wire knots prominent under thin skin drives the high re-operation rate.
Tighten the wire with the knee in extension and then flex to 90 degrees before final tightening — the wire should compress the articular surface, not allow gapping. If you tighten only in flexion the construct will be too tight in extension and may fail.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | Immediate | 0 to 2 weeks | Hinged brace locked in extension; touch or partial weight-bearing | Isometric quadriceps setting and straight-leg raises from day 1 | | Early | 2 to 6 weeks | Removable brace locked in extension for weight-bearing | Gentle passive flexion to 30 to 40 degrees once healed; advance to full weight-bearing in the brace | | Intermediate | 6 to 12 weeks | Radiograph at 6 weeks; unlock if bridging callus | Active-assisted motion, advance flexion toward 90 degrees by 8 to 10 weeks; stationary cycling | | Late | 3 to 6 months | Wean brace once quadriceps control is adequate | Progressive resistance and proprioception; return to sport or heavy labour at 4 to 6 months | Special considerations. After partial patellectomy, protect weight-bearing for 8 to 12 weeks because the tendon-to-bone healing interface is weaker than bone-to-bone fixation. Diabetic or immunocompromised patients progress more slowly with extended bracing and closer wound surveillance. In bilateral injuries, stagger the rehabilitation so one leg can support the other during recovery. Most patients regain full active and passive range of motion by 3 months and return to sport or heavy labour at 4 to 6 months when strength reaches at least 80 percent of the contralateral side and radiographic union is confirmed. Complications
- Incidence
- 20-50%
- Recognition
- Pain and tenderness over prominent K-wire ends or wire knots; skin breakdown; patient requests removal
- Prevention and management
- Prevention: bury K-wire ends in tendon, use low-profile cannulated screw constructs in thin patients, cut wires short. Management: hardware removal after radiographic union (usually greater than 6 months); consider screws at the index procedure if soft tissue is marginal
- Incidence
- 3-8%
- Recognition
- Increasing displacement on serial radiographs; loss of active extension; palpable gap at the fracture site
- Prevention and management
- Prevention: anatomic articular reduction, stable construct tested in flexion, protected weight-bearing in an extension brace. Management: revision ORIF if early; partial patellectomy or salvage if late failure with arthritis
- Incidence
- less than 5%
- Recognition
- Persistent fracture line at 6 months; pain with activity; loss of extension strength
- Prevention and management
- Prevention: anatomic reduction, stable fixation, bone grafting of comminuted fractures, protected mobilisation. Management: revision ORIF with bone graft; consider patellectomy if non-union with arthritis and poor bone stock
- Incidence
- 5-15%
- Recognition
- Inability to actively extend the knee fully despite full passive extension; quadriceps weakness
- Prevention and management
- Prevention: preserve patellar height (greater than 50% after partial patellectomy), protect the repair with a brace, early quadriceps activation. Management: intensive physiotherapy; consider vastus medialis advancement or tendon reconstruction if refractory
- Incidence
- 20-40% at 5-10 years
- Recognition
- Anterior knee pain, crepitus, stiffness, radiographic joint-space narrowing and osteophytes
- Prevention and management
- Prevention: anatomic articular reduction (step-off less than 2 mm), stable fixation, early mobilisation. Management: activity modification, injections, patellofemoral or total knee arthroplasty in end-stage disease
- Incidence
- 1-3%
- Recognition
- Erythema, warmth, drainage, elevated CRP/ESR, positive cultures
- Prevention and management
- Prevention: sterile technique, prophylactic antibiotics, careful soft-tissue handling in open injuries. Management: debridement, culture-directed antibiotics, implant retention or removal depending on time since surgery and union status
- Incidence
- rare (less than 2%)
- Recognition
- Sudden loss of active extension, palpable gap below the patella, high-riding patella on the lateral radiograph
- Prevention and management
- Prevention: secure tendon reattachment with transosseous sutures or anchors, protect with a brace, gradual loading. Management: acute repair with augmentation (cerclage wire or suture) and protected mobilisation
Viva & Exam Focus
TENSIONTENSION — the modified anterior tension-band principle
PATELLAPATELLA — operative decision algorithm
- The trap
- Malreduction greater than 2 mm raises contact pressure and accelerates post-traumatic arthritis; fluoroscopy alone misses subtle steps
- How to avoid it
- Confirm the retropatellar surface under direct vision; fix any step-off greater than 2 mm or gap greater than 3 mm
- The trap
- Radiographic displacement alone does not dictate surgery — a minimally displaced fracture with loss of extension still needs exploration and repair
- How to avoid it
- Assess active knee extension against gravity (straight-leg raise) before deciding operative versus non-operative care
- The trap
- The most common cause of re-operation — up to 50 percent of tension-band cases
- How to avoid it
- Cut K-wires short and bend the ends into tendon; use cannulated screw constructs in thin patients; consider low-profile plates
- The trap
- Small fragments will not hold hardware, with a risk of fixation failure or patellar tendon avulsion
- How to avoid it
- Partial patellectomy with transosseous sutures or suture anchors; preserve at least 50 percent of patellar height
- The trap
- A concomitant tendon rupture that is missed leads to early fixation failure when the patient loads the extensor mechanism
- How to avoid it
- Palpate the entire extensor mechanism for gaps before theatre and repair any tendon rupture at the same sitting
- The trap
- Up to 10 percent are open; even closed fractures can have significant contusion or degloving given the subcutaneous patella
- How to avoid it
- Urgent irrigation and debridement within 6 hours; delay definitive hardware until the soft-tissue envelope is healthy
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old labourer sustains a displaced transverse patellar fracture after a fall from scaffolding. He is unable to perform a straight-leg raise. Radiographs show 4 mm of articular step-off. How do you manage this patient?”
“A 35-year-old female athlete presents with a comminuted inferior pole patellar fracture after a dashboard injury. The inferior pole is in multiple small fragments and she has loss of active extension. Describe your operative plan.”
“A 28-year-old man underwent patellar ORIF with a K-wire tension band for a transverse fracture 9 months ago. He has united but complains of severe anterior knee pain when kneeling and a palpable prominence over the superior pole. Radiographs show the fracture is healed. How do you manage him?”
Indications for surgery
- Articular step-off greater than 2 mm or gap greater than 3 mm — absolute indication
- Loss of active knee extension (cannot perform a straight-leg raise)
- Open fracture or associated injuries requiring stabilisation
- Minimally displaced fractures with intact extension can be treated non-operatively in an extension brace for 4 to 6 weeks
Surgical anatomy
- Patella is a sesamoid within the extensor mechanism — quadriceps tendon proximal, patellar tendon distal
- The retropatellar articular surface must be visualised directly to confirm anatomic reduction
- The modified anterior tension band converts quadriceps distractive force into articular compression during flexion
- Longitudinal implants (K-wires or screws) must sit in the anterior half of the patella to act as a fulcrum
Approach and reduction
- Midline anterior longitudinal incision with full-thickness flaps
- Identify and protect the infrapatellar branch of the saphenous nerve
- Evacuate the haematoma and inspect the retropatellar surface through the fracture or a small arthrotomy
- Use pointed reduction clamps; confirm articular congruity by direct palpation before placing hardware
Fixation techniques
- Modified anterior tension-band wiring: parallel anterior K-wires plus a figure-of-eight wire through the tendons
- Cannulated screw tension band: 4.0 to 4.5 mm screws with the wire through the screw heads — lower profile, less hardware removal
- Partial patellectomy for comminuted poles: excise fragments, reattach the tendon with transosseous sutures or anchors, preserve greater than 50 percent patellar height
- Always test the construct with knee flexion to 90 degrees before final tightening — the wire should compress, not gap
Danger zones
- Placing implants too posteriorly — the tension-band effect is lost
- Leaving prominent K-wire ends or wire knots under thin skin — 20 to 50 percent re-operation rate
- Missing a concomitant quadriceps or patellar tendon rupture — leads to early fixation failure
- Over-tightening the wire with the knee already flexed — construct too tight in extension
Complications
- Hardware prominence requiring removal: 20 to 50 percent
- Loss of reduction: 3 to 8 percent — revision ORIF or salvage
- Non-union: less than 5 percent — revision with bone graft
- Extensor lag: 5 to 15 percent — physiotherapy, consider tendon advancement
- Post-traumatic arthritis: 20 to 40 percent at 5 to 10 years — related to residual step-off
Rehabilitation
- Brace locked in extension, touch weight-bearing for 2 weeks
- Immediate quadriceps setting and straight-leg raises
- Unlock the brace at 6 weeks if radiographic healing is progressing
- Full range of motion and strengthening by 3 months; return to sport at 4 to 6 months
- Partial patellectomy patients need 8 to 12 weeks of protected loading
Background & Evidence
Surgical anatomy. The patella is the largest sesamoid bone in the body, embedded within the quadriceps tendon, with the thickest hyaline cartilage in the human body (up to 7 mm). Its articular surface is divided into medial and lateral facets by a central ridge, and the medial facet has an odd facet that articulates only in deep flexion. The blood supply enters via the anterior surface and the inferior pole (inferior geniculate artery); the superior pole is relatively avascular. The quadriceps tendon (rectus femoris, vastus medialis, lateralis and intermedius) inserts into the superior pole, and the medial and lateral patellar retinacula reinforce the extensor mechanism on either side. The patellar tendon runs from the inferior pole to the tibial tubercle, enveloped by the deep infrapatellar bursa with the prepatellar bursa anteriorly. Vascular and nerve considerations. The geniculate arteries form a rich anastomosis around the patella; the superior lateral and medial geniculates are at risk during the approach. The infrapatellar branch of the saphenous nerve crosses the anterior knee and is frequently injured, leaving a numb patch lateral to the incision — counsel patients pre-operatively. The common peroneal nerve is not at risk in the standard midline approach but must be protected if a lateral incision or extensive dissection is required. Biomechanics of the modified anterior tension band. During knee flexion the quadriceps exerts a distractive force across a transverse patellar fracture. The modified anterior tension-band construct places the longitudinal implants (K-wires or screws) in the anterior half of the patella as a fulcrum; the figure-of-eight wire lies anterior to this fulcrum, so as the knee flexes the wire tightens and converts the distractive force into articular compression. This principle works only when the implants are placed anteriorly and the wire is tensioned correctly with the knee in extension before testing flexion. It is biomechanically superior to cerclage wiring alone. Outcomes. Anatomic reduction and stable fixation allow early mobilisation and reduce post-traumatic arthritis. Modified anterior tension-band wiring achieves union rates greater than 90 percent in transverse fractures; cannulated screw tension-band constructs show lower rates of hardware prominence and re-operation in several series; and partial patellectomy for comminuted poles restores extension with acceptable functional scores when at least 50 percent of patellar height is preserved. These benchmarks underpin the operative indications and fixation choices summarised above.
References
Long-term results after operative treatment of patellar fractures
- Classic long-term follow-up of 422 patellar fractures treated operatively
- Anatomic reduction correlated with better functional outcomes and lower rates of post-traumatic arthritis
- Established the importance of restoring articular congruity in patellar fractures
Biomechanical comparison of tension-band wiring versus cannulated screw fixation for transverse patellar fractures
- Cadaveric study comparing modified anterior tension-band wiring with cannulated screw tension-band constructs
- Both constructs provided stable fixation; screw constructs showed less displacement under cyclic loading in some models
- The anterior tension-band principle is critical regardless of implant type
Partial patellectomy for comminuted patellar fractures
- Retrospective review of partial patellectomy for comminuted inferior or superior pole fractures
- Preservation of at least 50 percent of patellar height maintained acceptable extensor mechanism function
- Patient satisfaction and functional scores were comparable to ORIF when reduction was not achievable
Hardware removal after patellar tension-band fixation
- Retrospective series documenting hardware removal rates after patellar ORIF
- Symptomatic hardware requiring removal in 20 to 50 percent of tension-band wiring cases
- Lower removal rates observed with cannulated screw constructs and buried K-wire techniques