Prone position | Lazy-S incision | Gastrocnemius interval | Tibial, common peroneal and popliteal vessels at risk
- Prone positioning is essential — the supine position does not allow safe access to posterior structures
- A lazy-S incision crosses the popliteal crease transversely to avoid a postoperative flexion contracture
- The deep plane between the two heads of gastrocnemius is the safe interval — both heads are supplied by the tibial nerve, so no nerve crosses it
- The tibial and common peroneal nerves lie within the fossa and are the principal dangers
- The medial sural cutaneous nerve is the key landmark — identify it first and trace it proximally to locate the tibial nerve safely
When & Why
What it exposes. The posterior approach gives direct access to the posterior aspect of the distal femoral condyles, the posterior capsule of the knee and the posterior cruciate ligament (PCL) tibial insertion, and the contents of the popliteal fossa — the tibial nerve, the common peroneal nerve (CPN) and the popliteal artery and vein. Primary indications. - Posterior coronal (Hoffa) fractures of the distal femoral condyles
- Large bony avulsions of the PCL from the posterior tibia
- Popliteal fossa masses — tumours, Baker cysts and vascular lesions
- Exploration of a tibial nerve or CPN injury, traumatic or iatrogenic
- Popliteal artery injury or aneurysm requiring direct vascular control
- Combined posterior distal femur fractures with posterior column involvement Why this approach is chosen. The posterior distal femur and popliteal fossa cannot be adequately visualised or instrumented from standard anterior or lateral approaches. Hoffa fragments displace posteriorly and need direct buttress plating from behind; anterior-to-posterior lag screws alone are biomechanically inferior. PCL avulsions are best reduced and fixed under direct vision through a posterior window. The popliteal neurovascular bundle lies in a confined space that demands a dedicated posterior exposure for safe exploration and repair. Contraindications. Medical instability precluding prone positioning; active infection in the popliteal region; severe soft-tissue compromise or scarring; and isolated anterior or lateral pathology better addressed by other approaches. Alternative approaches. A lateral approach for a lateral condyle fracture without posterior extension; a medial approach for a medial condyle fracture; a standard anterior approach for most supracondylar and intercondylar fractures; and combined medial and lateral approaches for complex bicondylar patterns. Position and landmarks. Place the patient prone on a radiolucent table after confirming cardiovascular and spinal stability. Pad the face, chest, pelvis, patellae and feet meticulously; position the arms abducted less than 90 degrees; apply a high-thigh tourniquet before turning if planned; and confirm C-arm access from both sides. Flex the knee 20-30 degrees over a radiolucent bolster to relax the neurovascular structures, and let the foot hang freely. Lateral decubitus (affected side up) is an alternative when combined anterior and posterior access is anticipated, but true prone gives superior visualisation of the fossa. Palpable landmarks are the medial and lateral femoral epicondyles, the adductor tubercle, the fibular head (for distal reference) and the joint line. The key soft-tissue landmarks are the biceps femoris tendon laterally (the CPN lies just medial to it), the semitendinosus and gracilis tendons medially, and the popliteal crease. Mark a lazy-S incision (typically 12-18 cm) with the transverse limb crossing the popliteal crease obliquely, the proximal limb along the border of biceps femoris or semitendinosus, and the distal limb following the interval between the two gastrocnemius heads.
The Exposure
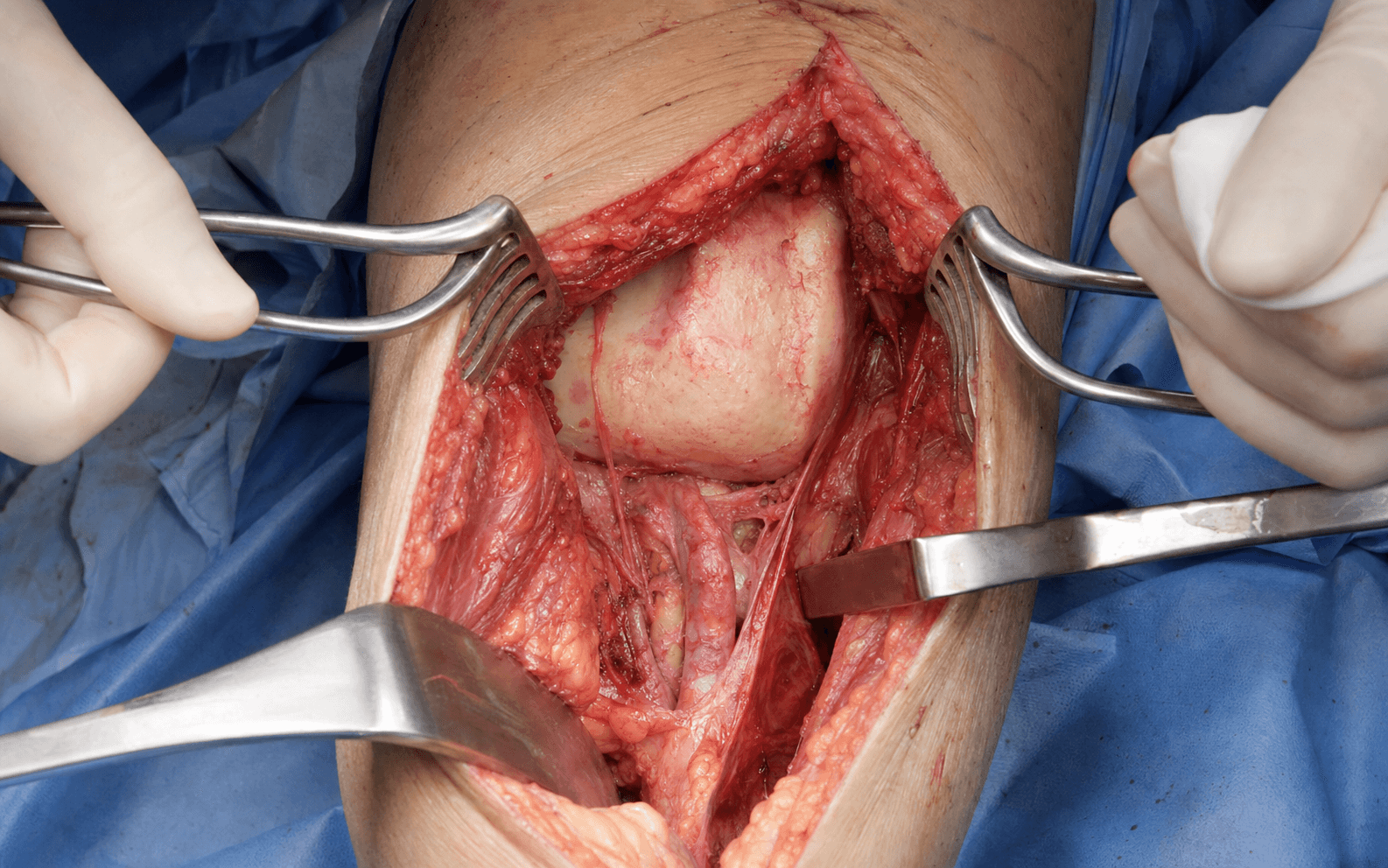
The popliteal fossa is a diamond-shaped space: superomedially bounded by semitendinosus and semimembranosus, superolaterally by biceps femoris, and inferomedially and inferolaterally by the two heads of gastrocnemius, with plantaris lying between the medial head and the tibial nerve. The tibial nerve enters from the sciatic bifurcation and courses distally in the midline, giving off the medial sural cutaneous nerve — the surgical landmark. The CPN runs laterally along the medial border of the biceps femoris tendon and winds around the fibular neck. The popliteal artery lies deep and slightly medial to the tibial nerve, with the vein between the artery and nerve. The internervous plane. There is no true internervous plane superficially. The safe deep plane is the interval between the medial and lateral heads of gastrocnemius — both supplied by the tibial nerve, so no nerve crosses it. The popliteal neurovascular bundle lies medial and deep to this interval and is protected by keeping the medial gastrocnemius head between the dissection and the bundle.
Exposure sequence
- Incise in a lazy-S with the transverse limb crossing the popliteal crease obliquely to avoid a flexion contracture.
- Run the proximal limb along the lateral border of biceps femoris (for lateral pathology) or the medial border of semitendinosus (for medial pathology).
- Bring the distal limb down the interval between the two gastrocnemius heads.
- In the distal subcutaneous fat, identify the medial sural cutaneous nerve.
- Trace it proximally — it reliably leads to the tibial nerve and is the safest way to find the main nerve without blind dissection.
- Palpate or visualise the CPN along the medial border of the biceps femoris tendon.
- Protect it with a vessel loop before any lateral retraction is applied.
- Incise the popliteal fascia in the midline.
- Identify the tibial nerve (traced from the medial sural cutaneous nerve) and sling it with a vessel loop.
- Locate the popliteal artery and vein deep and slightly medial to the nerve and retract them gently.
- Develop the interval between the medial and lateral heads of gastrocnemius bluntly.
- Retract both heads gently; divide the plantaris tendon if it limits exposure.
- The posterior capsule of the knee comes into view.
- The popliteal vessels lie deep to the tibial nerve — protect them by staying in the midline interval and using broad, gentle retraction.
- Retract the medial gastrocnemius head medially to keep the bundle safe on the far side of the interval.
- If intra-articular access is required, incise the posterior capsule transversely, just above the femoral condyles, under direct vision.
- Visualise the PCL tibial insertion for avulsion fractures and the posterior femoral condyles for Hoffa-fragment reduction.
The tibial nerve, the common peroneal nerve and the popliteal vessels are all within the operative field. Identify the medial sural cutaneous nerve first and trace it to the tibial nerve, loop the CPN along the biceps tendon before any lateral retraction, and keep strictly between the two gastrocnemius heads so the medial head guards the popliteal bundle. Never place metal retractors directly on a nerve, and never dissect medial to the medial gastrocnemius head without proximal and distal vascular control.
The medial sural cutaneous nerve is the single most reliable landmark in this approach. Find it in the distal subcutaneous fat and follow it proximally — it leads directly to the tibial nerve, sparing you blind dissection in a neurovascularly crowded fossa.
Dangers & Extensions
The danger structures live in three layers — subcutaneous, fascial and deep muscular — and each is protected by a specific manoeuvre.
- Structure at risk
- Medial sural cutaneous nerve
- How to protect it
- Identify early in the distal subcutaneous fat and preserve; trace proximally to reach the tibial nerve. Division leaves tolerable posteromedial calf numbness.
- Structure at risk
- Tibial nerve
- How to protect it
- Approach from its medial side using the sural nerve as a guide, and protect with a soft vessel loop before any deep retraction. Injury loses plantarflexion, inversion and sole sensation.
- Structure at risk
- Common peroneal nerve
- How to protect it
- Find along the medial border of the biceps femoris tendon and loop before any lateral retraction. Injury causes a foot drop.
- Structure at risk
- Popliteal artery and vein
- How to protect it
- Stay strictly between the two gastrocnemius heads and retract gently and broadly, keeping the medial head between you and the bundle. Never dissect medial to the medial head without vascular control.
- Structure at risk
- Posterior capsule and PCL
- How to protect it
- Incise under direct vision only after nerves and vessels are protected, and repair the capsule after PCL fixation.
- Structure at risk
- Geniculate vessels (middle geniculate)
- How to protect it
- Ligate or coagulate as encountered during capsulotomy.
Extensile options. Extend proximally along the lateral or medial intermuscular septum to expose the posterior femur up to the mid-diaphysis, protecting the sciatic nerve in the proximal wound. Extend distally along the chosen gastrocnemius head into the calf to reach the proximal tibia and the soleus and flexor hallucis longus origins for more extensive vascular or nerve work. For complex distal femur fractures, combine a posterior approach for the Hoffa fragment with a lateral approach for the supracondylar component and a medial approach for the medial condyle — this may need staged turning or a lateral decubitus position. Closure. Irrigate copiously and secure meticulous haemostasis, especially around the geniculate vessels. Place a suction drain in the popliteal fossa through a separate stab incision away from the main wound. Close the posterior capsule with absorbable suture if it was opened, allow the gastrocnemius interval to fall together, close the popliteal fascia loosely, and close the subcutaneous tissue and skin in layers — taking particular care at the corners of the transverse lazy-S limb to avoid skin necrosis. Obtain AP and lateral radiographs of the distal femur and knee, and a CT if articular reduction quality is uncertain. Complications. Intra-operative risks are tibial or CPN injury from excessive retraction, popliteal vessel injury during deep dissection, an inadvertent capsular tear or PCL damage, and inadequate exposure leading to malreduction of a Hoffa fragment. Post-operative risks are wound dehiscence or necrosis at the transverse limb, infection (higher risk in popliteal fossa surgery), stiffness or flexion contracture from a poorly designed incision, transient neurovascular deficit, and deep vein thrombosis related to prone positioning and popliteal manipulation. Meticulous padding, early nerve identification with vessel-loop protection, staying in the correct gastrocnemius interval and careful layered closure reduce all of these. Aftercare. Perform neurovascular observations hourly for the first 6 hours then 2-hourly, documenting ankle dorsiflexion, plantarflexion and sensation on the sole and dorsum of the foot. Immobilise the knee in extension in a brace, elevate the limb above heart level and start DVT prophylaxis in theatre. Protect with touch or non-weight-bearing for 6-12 weeks depending on fixation stability, begin early passive range of motion once the wound is stable, and review at 2 weeks (wound check), 6 weeks (radiographs), 3 months (CT if articular healing is uncertain) and 6-12 months (final functional assessment).
Procedures Through This Approach
- Hoffa fragment fixation — reduce the posterior coronal fragment under direct vision and apply a buttress plate (a 3.5 mm T-plate or anatomic posterior distal femur plate) to the posterior surface with screws directed anteriorly; bone-graft any metaphyseal void.
- Distal femur ORIF — when a Hoffa fragment coexists with supracondylar or intercondylar fractures, fix the posterior fragment through this approach first, then add standard lateral or medial plating through separate incisions.
- PCL bony avulsion — reduce the avulsed tibial fragment anatomically and fix with one or two cannulated screws with washers, a small buttress plate for a large fragment, or suture anchors; repair the posterior capsule afterwards.
- Popliteal fossa exploration — expose and control the popliteal artery proximally and distally for vascular injury; decompress or repair the tibial or CPN under magnification for nerve injury; and dissect a mass free while protecting all neurovascular structures, excising a Baker cyst completely including its joint communication.
Viva & Exam Focus
POSTERIORPOSTERIOR — the prone popliteal exposure
DANGERDANGER — structures at risk, layer by layer
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 35-year-old motorcyclist has a coronal plane fracture of the posterior medial femoral condyle (Hoffa fragment) with 4 mm displacement. Describe your surgical approach and fixation strategy.”
“A 28-year-old footballer has a displaced bony avulsion of the PCL from the posterior tibia. The fragment is 2 cm in size. How would you approach this injury?”
“A 45-year-old patient presents with a large Baker cyst causing tibial nerve compression symptoms. Describe your surgical plan for excision.”
Positioning
- Prone position is mandatory for adequate exposure
- Knee flexed 20-30 degrees over a radiolucent bolster
- All pressure points padded, including face and chest
- Tourniquet applied before turning if used
- C-arm access confirmed from both sides
Incision
- Lazy-S with the transverse limb crossing the popliteal crease
- Proximal limb along biceps femoris or semitendinosus
- Distal limb follows the gastrocnemius-head interval
- Prevents a postoperative flexion contracture
- Typical length 12-18 cm
Landmark nerve
- Medial sural cutaneous nerve identified first in the subcutaneous plane
- Traced proximally to locate the tibial nerve reliably
- CPN along the medial border of biceps femoris
- Both nerves protected with vessel loops before retraction
- Never place metal retractors directly on nerves
Internervous plane
- Interval between the medial and lateral gastrocnemius heads
- Both heads innervated by the tibial nerve — a safe plane
- Popliteal vessels lie deep and medial to the interval
- Stay strictly between the heads to protect the vessels
- Plantaris may be divided to improve exposure
Danger structures
- Tibial nerve — central, approached via the sural cutaneous nerve
- Common peroneal nerve — lateral, along biceps femoris
- Popliteal artery and vein — deep and medial
- Posterior capsule and PCL insertion — protect during capsulotomy
- Multiple geniculate vessels — ligate as encountered
Key procedures
- Hoffa-fragment buttress plating from the posterior surface
- PCL bony avulsion — anatomic reduction and screw fixation
- Popliteal vessel exploration and repair
- Tibial or CPN decompression or repair
- Combined with lateral or medial approaches for complex fractures
Closure and aftercare
- Layered closure with careful attention to the transverse limb
- Drain placed away from the main incision
- Neurovascular observations hourly initially
- Touch or non-weight-bearing for 6-12 weeks
- Early motion in a hinged brace to prevent stiffness
References
Posterior Approach for Single-stage Fixation of Medial Hoffa with Posterior Cruciate Ligament Avulsion: A Rare Case Report.
- The posterior approach allows single-stage anatomic fixation of a combined medial Hoffa fracture and PCL avulsion under direct vision while protecting the neurovascular structures.
Novel approach of plate assisted buttressing in Hoffa fracture.
- Plate-assisted buttressing through a posterior approach provides stable fixation for Hoffa fractures of the distal femur.
Busch-Hoffa fracture: A systematic review.
- A systematic review supports the use of posterior approaches for complex Hoffa fractures requiring direct visualisation and buttress plating.
Posterior open approach combined with suture bridge technique for tibial insertion avulsion fractures of posterior cruciate ligament.
- A posterior open approach with a suture-bridge technique achieves stable fixation for PCL tibial avulsion fractures with direct neurovascular protection.