Posterior approach | advanced
- Classify instability correctly: traumatic vs atraumatic; unidirectional vs multidirectional (MDI); voluntary vs involuntary — management is fundamentally different (MDI rehabilitation first, voluntary dislocation needs psychosocial workup before surgery)
- Posterior bone loss threshold: greater than 25% glenoid diameter — proceed to bone block (Eden-Hybinette / Mead-Bain). Less than 25% — soft tissue procedure (posterior Bankart repair or capsulorrhaphy)
- Kim lesion: incomplete, concealed avulsion of the posteroinferior labrum — the superficial labral attachment looks intact, so it is missed unless the arthroscopist PROBES and elevates the labrum. High-yield advanced orthopaedic practice topic. Original description: Kim SH 2004, Arthroscopy (PMID 15346113)
- Axillary nerve is the primary danger in the posterior approach — it lies roughly 5–6 cm distal to the posterolateral acromion corner in the deltoid-splitting interval; never place a retractor more than approximately 5 cm distal when working posteriorly
- “Glenoid track is an ANTERIOR-instability concept (Di Giacomo 2014, PMID 24384275). Its extrapolation to posterior instability is biomechanically logical but not formally validated — a large engaging reverse Hill-Sachs lesion with posterior glenoid loss is best described as a bipolar lesion that may justify bony augmentation
- “Voluntary dislocation is a red flag: NEVER operate without thorough psychosocial evaluation. Surgery has very poor outcomes in voluntary dislocators with underlying psychiatric or personality disorder
- “Post-operative loss of external rotation after posterior capsulorrhaphy equals overtightening. Complications include functional limitation, pain with ER activities, and secondary anterior impingement
- “Counsel realistically: open posterior bone block is salvage surgery with substantial graft resorption and recurrence rates at long-term follow-up (Villefort/Gerber 2022, PMID 36911764) — it is NOT a high-reliability operation like an anterior Latarjet
When & Why
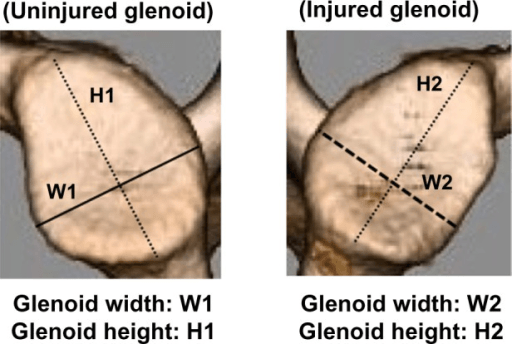
Posterior shoulder instability is far less common than anterior instability and is frequently missed — the operation you choose depends entirely on two things: the instability pattern (traumatic vs atraumatic, unidirectional vs multidirectional, voluntary vs involuntary) and the amount of posterior glenoid bone loss. Get the pattern wrong and you operate on the wrong patient; get the bone loss wrong and you do the wrong operation on the right patient. The decision that drives everything — the 25% bone-loss threshold. Quantify posterior glenoid bone loss on a CT with 3D reconstruction (Pico method or best-fit circle, expressed as a percentage of the inferior glenoid diameter). Plain films are insufficient.
Traumatic unidirectional posterior instability with a posterior labral tear (Bankart or Kim lesion), no significant bone loss. Operation: arthroscopic posterior Bankart repair ± capsular plication. Reserve for patients who have failed 3–6 months of physiotherapy or athletes with functionally limiting instability.
Posterior glenoid bone loss greater than 25% by CT, an engaging off-track reverse Hill-Sachs lesion, or recurrence after a previous soft-tissue posterior stabilisation. Operation: posterior bone block (Eden-Hybinette iliac-crest autograft, or Mead-Bain coracoid transfer).
Multidirectional instability (capsular laxity, sulcus sign greater than 2 cm persisting with external rotation) has NO bone loss. Structured physiotherapy for at least 6 months first (80–85% improve). If surgery is ever needed it is an inferior capsular shift — NOT a bone block, NOT an isolated Bankart repair.
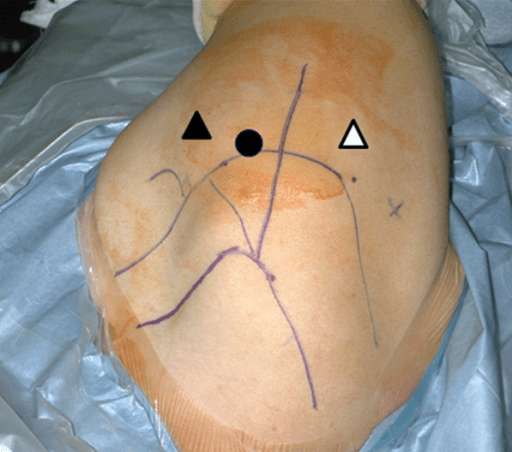
Two red flags before you ever offer surgery. First, voluntary dislocation: a patient who can deliberately dislocate using muscular contraction needs a formal psychosocial or psychiatric evaluation before any surgical consideration — surgery in voluntary dislocators with underlying psychopathology has uniformly poor outcomes. Second, multidirectional instability: never operate before an adequate rehabilitation trial, and never perform a bone block where there is no bone loss. Consent realistically. Counsel the patient that the open posterior bone block is salvage surgery, not a high-reliability operation like an anterior Latarjet: long-term data show tested recurrent instability in around 30%, major graft resorption in around 62%, and degenerative progression in about two-thirds at median 9-year follow-up (Villefort/Gerber 2022, PMID 36911764). Specific risks to consent: axillary nerve injury (deltoid paralysis), loss of external rotation from overtightening, graft prominence or resorption, recurrent instability, and iliac-crest donor-site morbidity (pain, lateral femoral cutaneous nerve injury, haematoma, infection). Setup. Lateral decubitus is preferred for posterior access (beach chair is an alternative). General anaesthesia plus an interscalene block. Before draping, mark the posterolateral acromion corner and measure and mark the 5–6 cm axillary nerve safe zone inferiorly — this single landmark governs the whole posterior dissection.
The Operation
The goal is to restore a posterior bony and/or soft-tissue restraint to the humeral head. Two operations sit under this page: the open posterior bone block (Eden-Hybinette) for the bony-deficient shoulder, and the arthroscopic posterior Bankart repair for the soft-tissue shoulder. Both share the same critical safety principle — protect the axillary nerve, which lies about 5–6 cm below the posterolateral acromion corner. The exposure is laid out in full below (and in depth on the posterior approach to the shoulder page).
Open posterior bone block (Eden-Hybinette) — the exposure first
- Lateral decubitus (preferred for posterior access) or beach chair; general anaesthesia plus interscalene block.
- Before draping, mark the posterolateral acromion corner and measure 5–6 cm inferiorly — the axillary nerve boundary. The entire posterior dissection is organised around this one landmark.
- Horizontal or oblique posterior incision starting at the posterolateral acromion corner, extending 6–8 cm medially and inferiorly. A longitudinal incision in line with the posterior deltoid fibres is an alternative.
- Re-confirm the 5 cm safe zone on the skin before any deep dissection.
- Split the posterior third of deltoid in the line of its fibres to expose the posterior rotator cuff.
- Stay proximal: do not extend the split, and do not place retractors more than about 5 cm below the acromion — that is the axillary nerve boundary.
- The functional internervous plane is between infraspinatus (suprascapular nerve, C5–C6) above and teres minor (axillary nerve, C5–C6) below.
- The interval is narrow and the inferior dissection brings the axillary nerve into the field, so most surgeons split infraspinatus in line with its fibres rather than developing the interval. Either way the axillary nerve below teres minor is the limiting structure.
- Divide infraspinatus longitudinally (in line with its fibres), NEVER transversely — a transverse split denervates the lateral portion.
- Open the capsule via a capsulotomy or an H-shaped capsular flap to expose the posterior glenoid and the bony defect.
- Palpate the axillary nerve (strap-like, taut) at the inferior capsular margin before placing any inferior retractor; blunt dissection only; never use a self-retaining retractor beyond 5 cm from the acromion.
- Confirm the bone-loss indication: posterior glenoid loss greater than 25% or an off-track reverse Hill-Sachs lesion (templated on the pre-operative CT).
- Burr the posterior glenoid surface to a bleeding bony bed, sized to the defect dimensions.
- Tricortical iliac crest graft, approximately 2.5 × 1.5 × 1 cm, matched to the defect on CT templating, harvested from the ipsilateral or contralateral crest via an anterior approach.
- Alternative: Mead-Bain modification — coracoid process with attached conjoint tendon transferred to the posterior glenoid for a dynamic stabilisation component (limited evidence vs Eden-Hybinette).
- Anticipate donor-site morbidity: 10–15% persistent pain, lateral femoral cutaneous nerve injury around 10%, haematoma 5%, infection 2%.
- Place the graft extra-articular, flush with the posterior glenoid articular surface — NOT proud (causes direct impingement on the humeral head and accelerated arthritis), NOT recessed (provides inadequate articular arc extension).
- Fix with two 3.5 mm cortical screws or cannulated screws over guide wires.
- Confirm position by direct visualisation and fluoroscopy before closing.
- Repair the capsule OVER the graft so the graft lies extra-articular beneath the repaired capsule.
- Repair infraspinatus anatomically to its tendon margins; repair deltoid to the fascial margin.
- Layered closure.
- Immobilise in an abduction/neutral-rotation orthosis for 4–6 weeks to protect the posterior capsule and graft while early healing occurs.
Arthroscopic posterior Bankart repair (less than 25% bone loss)
- Lateral decubitus or beach chair. Posterior viewing portal; anterolateral working portal (inflow/instruments); accessory posteroinferior (7 o'clock) portal for inferior anchor placement.
- Inspect the articular surfaces, biceps root, and anterior labrum.
- Critically examine the posteroinferior labrum: use a blunt probe to elevate the labral edge and look for a concealed Kim lesion (incomplete tear visible only with probing). Never rely on visual inspection alone.
- Using an arthroscopic elevator, fully mobilise the posterior labrum from the glenoid neck (6 to 10 o'clock posteriorly) to create an adequate tissue cuff for repair.
- Freshen the glenoid neck with a rasp or burr to a bleeding bone bed for healing.
- Place suture anchors at the 7, 8, and 9 o'clock positions on the posterior glenoid rim (right shoulder). Start inferiorly and work superiorly. Bio-composite or all-suture anchors.
- Pass sutures through the posterior labrum and advance the labrum superiorly (shift) to restore the posterior bumper.
- Tie knots sequentially inferior to superior, alternating half hitches with a reversed post.
- Add plication sutures to the posterior capsule to reduce volume, but preserve a minimum of 30° external rotation. Excessive plication limits ER, reduces infraspinatus efficiency, and may cause anterior impingement.
- With the arm in forward flexion and internal rotation, confirm no posterior subluxation under direct vision and that posterior apprehension has resolved.

Before any inferior retractor is placed, identify and palpate the axillary nerve. It exits the quadrilateral space (bounded by teres major inferiorly, teres minor superiorly, the long head of triceps medially, and the humeral surgical neck laterally), winds anteriorly around the surgical neck, and in the posterior approach lies an average of 5.6 cm (range 4.9–6.3 cm) from the posterolateral acromion corner. Mark the 5 cm boundary before draping; place no inferior retractor beyond it; use blunt dissection inferiorly; and avoid self-retaining retractors in the inferior position. Injury causes devastating deltoid paralysis and a circumflex shoulder numbness patch.
The posterior capsule is the primary restraint to internal rotation. Excessive plication shortens it and limits external rotation — the reverse of GIRD. Target tension preserves a minimum of 30° ER; a loss of ER greater than 30° from the pre-operative baseline represents overtightening. Assess ER incrementally after each plication pass so you do not over-plicate.
A proud graft (lateral to the articular surface) impinges directly on the humeral head and causes glenohumeral arthritis; a recessed graft provides inadequate articular arc extension and fails to neutralise the engaging reverse Hill-Sachs. The graft must sit flush with the posterior glenoid face, confirmed on fluoroscopy before closure.
Aftercare & Complications
Rehabilitation — posterior Bankart repair vs posterior bone block
- Posterior Bankart (soft tissue)
- Sling in neutral rotation (NOT internal rotation — IR stresses the posterior capsule). Pendulums and passive ROM only. No active elevation or rotation.
- Posterior bone block (Eden-Hybinette)
- Sling immobilisation. Passive pendulum exercises only. Wound check at 2 weeks. Radiograph at 6 weeks to confirm graft position and early union.
- Posterior Bankart (soft tissue)
- Active-assisted ROM; sling discarded progressively; rotator cuff isometrics. No passive ER stretch until week 8.
- Posterior bone block (Eden-Hybinette)
- Active-assisted ROM; posterior cuff and periscapular strengthening. Avoid extremes of internal rotation (graft stress) until 12 weeks.
- Posterior Bankart (soft tissue)
- Progressive active ROM; ER strengthening; periscapular stabilisers; proprioception.
- Posterior bone block (Eden-Hybinette)
- Progressive strengthening. CT at 3 months to confirm graft incorporation before progressive return to activity.
- Posterior Bankart (soft tissue)
- Contact sport minimum 6 months. Overhead athletes 4–6 months on sport-specific criteria.
- Posterior bone block (Eden-Hybinette)
- Contact sport minimum 6 months, and only once graft incorporation is confirmed on CT.
Expected outcomes. Arthroscopic posterior capsulolabral repair is a reliable first-line operation for unidirectional posterior instability without significant bone loss: Bradley et al. 2006 (PMID 16567458) reported mean ASES improving from 50 to 86 with 89% returning to sport at mean 27 months in 100 shoulders, though recurrence and failure to return to the same level are higher in contact athletes. Posterior bone block outcomes are mixed — arthroscopic iliac-crest bone block achieved Rowe 18 to 82 with union in all 19 shoulders at short follow-up (Schwartz/Lafosse 2013, PMID 23337111), but long-term open data are sobering: Villefort/Gerber 2022 (PMID 36911764) reported only modest score gains, around 30% tested recurrent instability, 62% major graft resorption, and degenerative progression in two-thirds at median 9 years. Frame the bone block as salvage for failed soft-tissue surgery or significant posterior glenoid deficiency, not a first-line high-reliability procedure. MDI after inferior capsular shift or arthroscopic plication does well in roughly 80–90% of well-selected patients who have failed rehabilitation, with worse outcomes in hyperlax and voluntary patients. Complications — recognition, prevention, management
- Recognition & prevention
- Arthroscopic Bankart 5–15% recurrence; higher in contact athletes and unrecognised bone loss. Bone block up to about 30% long-term (Villefort/Gerber 2022). Prevent by probing for a Kim lesion, achieving an adequate labral shift, and obtaining a CT to quantify bone loss.
- Management
- CT to reassess bone loss and glenoid track. If bone loss has progressed beyond 25% or the graft has resorbed, revise to a bone block or revision graft.
- Recognition & prevention
- 1–2% of posterior approaches; most are neuropraxias recovering at 3–6 months, permanent palsy less than 0.5%. Prevent with the 5 cm rule: mark the boundary, palpate the nerve before inferior retraction, blunt dissection only.
- Management
- Neuropraxia — observe, EMG at 6 weeks, expect recovery. Complete division — immediate microsurgical repair or nerve grafting.
- Recognition & prevention
- 10–30% have some limitation; significant loss (greater than 30°) in 5–10%. Mechanism is overtightening. Prevent by preserving a minimum 30° ER and assessing tension incrementally.
- Management
- Physiotherapy and posterior capsular stretching first. If severe and functional, arthroscopic posterior capsular release (protect the axillary nerve inferiorly).
- Recognition & prevention
- Major resorption (Zhu grade II) in around 60% long-term (Villefort/Gerber 2022), contributing to recurrence and arthrosis. Counsel patients the graft frequently remodels or partly resorbs.
- Management
- Monitor; manage recurrence on its merits. Limited revision evidence.
- Recognition & prevention
- Graft lateral to the articular surface causes direct impingement and accelerated glenohumeral arthritis. Prevent with flush positioning confirmed fluoroscopically.
- Management
- Symptomatic prominence — hardware or graft revision.
- Recognition & prevention
- Persistent pain 10–15%, lateral femoral cutaneous nerve injury around 10%, haematoma 5%, infection 2%.
- Management
- Usually settles; manage haematoma or infection on its merits; LFCN injury is predominantly neuropraxia.
Viva & Exam Focus
POSTERIORPOSTERIOR — Assessment of Posterior Instability
BONEBONE — Posterior Bone Block Technique (Eden-Hybinette)
Soft tissue procedures (less than 25% posterior glenoid bone loss): - Posterior Bankart repair (arthroscopic or open) - Posterior capsulorrhaphy Bone block required (greater than 25% bone loss or engaging reverse Hill-Sachs): - Eden-Hybinette (iliac crest autograft to posterior glenoid) - Mead-Bain modification (coracoid transfer to posterior glenoid) - Glenoid track concept: an off-track reverse Hill-Sachs lesion combined with bone loss mandates bony augmentation Quantify bone loss on CT (3D reconstruction): Pico method or best-fit circle method. Express as a percentage of the inferior glenoid diameter.
Location: exits the quadrilateral space, winds around the surgical neck of the humerus from posterior to anterior. In the posterior approach it lies 5–6 cm from the posterolateral corner of the acromion. At risk when: placing inferior retractors aggressively, working too far distally on the posterior capsule, or rough retraction of deltoid. Protection: stay within 5 cm of the acromion edge when placing retractors, palpate the nerve before dividing any posterior capsule inferiorly, use blunt dissection inferiorly, and do NOT use self-retaining retractors beyond 5 cm. Consequence of injury: deltoid paralysis (catastrophic for shoulder function) and circumflex shoulder numbness.
Definition: an incomplete and concealed avulsion of the posteroinferior labrum. The superficial labral attachment looks intact (often only a shallow surface crack at the chondrolabral junction), but probing reveals detachment of the DEEP portion of the labrum, with loss of normal labral height and consequent chondrolabral retroversion (Kim SH et al. 2004, Arthroscopy, PMID 15346113). Clinical significance: first described in a case series of 15 shoulders with posterior or multidirectional posteroinferior instability — it is a distinct lesion, not a prevalence figure. Missed on routine arthroscopy unless the labrum is probed carefully and elevated. Exam relevance: examiners test whether you would PROBE the posteroinferior labrum during arthroscopy — do NOT rely on visual inspection alone. Treatment: convert the concealed incomplete lesion to a complete tear, then labroplasty to restore labral height plus capsular shift. Failure to address the lesion causes persistent posterior instability.
Definition: glenohumeral instability in multiple planes with global capsular laxity, often bilateral. Classic demographic: young hypermobile patients, overhead athletes. Cardinal sign: sulcus sign greater than 2 cm with the arm in neutral rotation that does NOT reduce with external rotation (in unidirectional inferior instability, ER tightens the rotator interval and reduces the sulcus; in MDI it persists due to rotator interval laxity). Management first-line: structured physiotherapy minimum 6 months (rotator cuff strengthening, periscapular stabilisation, proprioception). 80–85% improve with rehabilitation alone. Surgery only if: failed 6 months supervised rehabilitation. Procedure: inferior capsular shift (Neer's open or arthroscopic plication). Do NOT perform a bone block for MDI without bone loss.
Definition: the patient deliberately dislocates the shoulder using muscular contraction. May be a learned behaviour, secondary gain, or a symptom of underlying psychiatric disorder. Screening: ask directly whether the patient can dislocate the shoulder themselves; observe for active muscular contraction versus passive apprehension. Workup before any surgical consideration: formal psychiatric or psychological evaluation. Assess for factitious disorder, somatisation, Munchausen syndrome, and secondary gain. Rule out a benign trick shoulder in athletes without psychological overlay. Key principle: surgery in voluntary dislocators with underlying psychopathology has uniformly poor outcomes (high recurrence, non-compliance, chronic pain, litigation). Defer surgery until psychiatric clearance.
Origin (anterior instability): the glenoid track and on-track vs off-track paradigm was defined for ANTERIOR instability and the Hill-Sachs lesion (Di Giacomo, Itoi and Burkhart 2014, PMID 24384275). Anterior calculation: glenoid track width = 0.83 × D − d, where D = glenoid diameter and d = anterior glenoid bone-loss width. If the Hill-Sachs interval exceeds the track, the lesion is OFF-track. Posterior extrapolation (use cautiously in the viva): by analogy a reverse Hill-Sachs lesion (anteromedial humeral head impaction) may engage the posterior rim during the posterior apprehension arc. This posterior application is biomechanically plausible but NOT formally validated — describe it as a bipolar bone-loss assessment rather than quoting a validated posterior track number. Practical message: a large engaging reverse Hill-Sachs combined with posterior glenoid loss is a bipolar problem that may require addressing both sides (posterior bone block plus a humeral-side or capsular procedure).
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 20-year-old female gymnast presents with bilateral shoulder instability affecting her performance and daily activities. Examination reveals a Beighton score of 7/9, bilateral sulcus sign of 2.5 cm (persisting with external rotation), positive anterior and posterior load-and-shift tests bilaterally, and diffuse shoulder apprehension in multiple planes. Plain radiographs are normal. How do you manage this patient?”
“A 28-year-old rugby player has a 3-year history of recurrent posterior shoulder instability after an initial tackle injury, one ED reduction and multiple subluxation episodes. CT shows 30% posterior glenoid bone loss and a large anteromedial humeral head impaction (reverse Hill-Sachs). Arthroscopic posterior Bankart repair 18 months ago failed. What is your operative plan?”
“A 25-year-old competitive swimmer underwent arthroscopic posterior capsulolabral repair 4 months ago for posterior instability. She now returns with persistent posterior shoulder pain and inability to externally rotate beyond neutral (0°). Pre-operatively she had 60° ER bilaterally. What is your diagnosis, its mechanism, and management?”
Classification
- Traumatic vs atraumatic: traumatic = discrete event, labral tear likely; atraumatic = insidious, capsular laxity.
- Unidirectional vs multidirectional (MDI): a sulcus sign persisting with ER equals MDI. MDI is rehabilitation first.
- Voluntary vs involuntary: voluntary dislocators need a psychosocial workup BEFORE any surgery.
- Kim lesion: concealed incomplete posteroinferior labral tear — missed without probing.
Bone Block Threshold
- Less than 25% posterior glenoid bone loss: soft tissue procedure (posterior Bankart repair or capsulorrhaphy).
- Greater than 25% bone loss OR an off-track reverse Hill-Sachs: posterior bone block (Eden-Hybinette iliac crest autograft).
- Measure bone loss on CT 3D reconstruction — Pico method or best-fit circle. Plain films are insufficient.
- Glenoid track: track width = 0.83 × glenoid diameter minus bone loss; compare to the reverse Hill-Sachs width on CT.
Danger Zones — Posterior Approach
- Axillary nerve: 5–6 cm from the posterolateral acromion corner. Mark before any retractor. No inferior retractors beyond 5 cm.
- Suprascapular nerve: about 2 cm medial to the superior glenoid margin in the suprascapular notch — at risk during medial dissection.
- Posterior humeral circumflex vessels: accompany the axillary nerve in the quadrilateral space.
- Infraspinatus tendon: divide longitudinally (in line with fibres), NEVER transversely, to avoid denervating the lateral portion.
Key Anatomy
- Posterior approach interval: infraspinatus (suprascapular nerve) to teres minor (axillary nerve) — a functional, not true, internervous plane.
- Infraspinatus: external rotation and posterosuperior dynamic stabilisation; denervation weakens ER.
- Kim lesion: a posteroinferior concealed incomplete labral tear — probe is mandatory, never rely on visual inspection alone.
- Posterior capsule: the primary constraint to internal rotation; overtightening limits ER.
Bone Block Technique (Eden-Hybinette)
- Harvest: tricortical iliac crest autograft, size templated on pre-operative CT.
- Position: flush with the posterior glenoid articular surface — NOT proud (impingement), NOT recessed (inadequate arc).
- Fixation: two 3.5 mm cortical screws; confirm position with fluoroscopy.
- The graft is extra-articular: repair the capsule and infraspinatus over it.
- Confirm graft incorporation at 3 months CT before return to contact sport.
MDI — Key Points
- Diagnosis: bilateral instability, sulcus sign greater than 2 cm persisting with ER, instability in more than two planes, Beighton hypermobility.
- Treatment: structured physiotherapy minimum 6 months FIRST; 80–85% improve without surgery.
- Surgical option if rehab fails: inferior capsular shift (Neer's open or arthroscopic plication). NOT a bone block. NOT an isolated Bankart repair.
- Voluntary dislocation: never operate without formal psychosocial evaluation — surgery in psychopathological voluntary dislocators has uniformly poor outcomes.
Complications
- Recurrent instability (Bankart repair): 5–15% arthroscopic; higher in contact athletes and unrecognised bone loss.
- Axillary nerve injury: 1–2% incidence; most neuropraxia recovering at 3–6 months; permanent palsy less than 0.5%. Prevention is the 5 cm rule.
- Loss of ER after capsulorrhaphy: 5–10% significant. Mechanism is overtightening. Management is physiotherapy then arthroscopic release.
- Graft proud: direct humeral impingement and glenohumeral arthritis. Prevention is flush placement confirmed fluoroscopically.
- Donor-site morbidity (iliac crest): 10–15% persistent pain, 10% lateral femoral cutaneous nerve injury.
Evidence Base
- Kim SH et al. 2004 (PMID 15346113): Kim lesion defined — concealed incomplete posteroinferior labral avulsion; 15 shoulders, labroplasty plus capsular shift.
- Bradley JP et al. 2006 (PMID 16567458): arthroscopic posterior capsulolabral reconstruction, 100 shoulders — mean ASES 50 to 86, 89% return to sport at mean 27 months.
- Schwartz DG / Lafosse L et al. 2013 (PMID 23337111): arthroscopic posterior bone block, 19 shoulders — Rowe 18 to 82, union in all.
- Villefort / Gerber et al. 2022 (PMID 36911764): open posterior bone block, median 9-year follow-up — about 30% recurrence, 62% major graft resorption, arthrosis in 67% (cautionary).
- Burkhead WZ and Rockwood CA 1992 (PMID 1634579): exercise programme — 80% (53/66) good or excellent in ATRAUMATIC instability vs only 16% in traumatic.
- Glenoid track: Di Giacomo et al. 2014 (PMID 24384275) — validated for ANTERIOR instability; posterior application is by analogy only.
Exam Pearls
- The Kim lesion is the highest-yield hidden diagnosis in posterior instability — always probe the posteroinferior labrum.
- Bone loss threshold 25%: below this a soft-tissue repair; above this a bone block. Memorise this number.
- MDI: never operate before 6 months rehabilitation. Voluntary dislocation: never operate without psychosocial clearance.
- Axillary nerve: 5 cm from the posterolateral acromion — this single number prevents the most feared complication.
- Post-capsulorrhaphy loss of ER: overtightening. A minimum of 30° ER must be preserved during posterior plication.
Background & Evidence
Epidemiology. Posterior instability constitutes only 2–10% of all shoulder instability — far less common than anterior — and is underdiagnosed, with posterior dislocation missed in up to 60% of cases on initial presentation. Natural history. Traumatic posterior instability with a labral tear has a low spontaneous healing rate. Atraumatic instability with capsular laxity may respond to rehabilitation (up to 80–85% in MDI). Untreated engaging lesions progress to symptomatic instability. Classification framework. Four axes determine management:
- Traumatic vs atraumatic: a single traumatic event (axial load to a forward-flexed, internally rotated arm — a football tackle or a fall) produces a posterior labral tear (posterior Bankart) or Kim lesion; atraumatic instability is insidious, from repetitive microtrauma (bench pressing, swimming) or generalised ligamentous laxity, with capsular redundancy rather than a discrete labral tear.
- Unidirectional vs multidirectional: pure unidirectional posterior instability responds better to surgery; MDI requires rehabilitation first.
- Voluntary vs involuntary: voluntary dislocation (deliberate dislocation by muscular contraction) demands a psychosocial workup before any surgery. Posterior glenoid and soft-tissue anatomy. The normal glenoid is pear-shaped and slightly retroverted (average 2–7°); the posterior glenoid rim is the critical stabilising structure for posterior instability, so posterior bone loss must be quantified on CT. The posterior labrum is a fibrocartilaginous thickening deepening the socket — a posterior labral tear (posterior Bankart) is a detachment from the posterior rim, while the Kim lesion is a concealed incomplete tear within the labral substance without surface disruption. The posterior capsule reinforces the joint; a tight posterior capsule paradoxically causes anterosuperior humeral head migration (GIRD — glenohumeral internal rotation deficit) and is associated with superior labral pathology in overhead athletes. Infraspinatus originates in the infraspinous fossa, inserts on the middle facet of the greater tuberosity, provides external rotation and posterior dynamic stabilisation, and is supplied by the suprascapular nerve (C5–C6). Teres minor originates on the lateral border of the scapula, inserts on the inferior facet of the greater tuberosity, provides external rotation and posteroinferior dynamic stabilisation, and is supplied by an axillary nerve branch — placing it at risk inferiorly. Key evidence. Kim SH et al. 2004 (PMID 15346113) defined the Kim lesion (concealed incomplete posteroinferior labral avulsion) in 15 shoulders. Bradley et al. 2006 (PMID 16567458) reported arthroscopic posterior capsulolabral reconstruction in 100 shoulders with mean ASES improving from 50 to 86 and 89% returning to sport at mean 27 months. Schwartz/Lafosse et al. 2013 (PMID 23337111) reported arthroscopic posterior bone block in 19 shoulders with Rowe improving from 18 to 82 and radiographic union in all. Villefort/Gerber et al. 2022 (PMID 36911764) provided the cautionary long-term open data: at median 9-year follow-up, around 30% tested recurrent instability, 62% major graft resorption, and degenerative progression in 67%. Burkhead and Rockwood 1992 (PMID 1634579) showed an exercise programme gave 80% good or excellent results in atraumatic instability but only 16% in traumatic — selection matters. The glenoid track / on-track-off-track concept (Di Giacomo, Itoi and Burkhart 2014, PMID 24384275) is validated for anterior instability; its posterior application is by analogy only.
References
References 1. Kim SH, Ha KI, Yoo JC, Noh KC (2004). Kim's lesion: an incomplete and concealed avulsion of the posteroinferior labrum in posterior or multidirectional posteroinferior instability of the shoulder. Arthroscopy. 20(7):712–720. PMID: 15346113. DOI: 10.1016/j.arthro.2004.06.012 2. Bradley JP, Baker CL 3rd, Kline AJ, Armfield DR, Chhabra A (2006). Arthroscopic capsulolabral reconstruction for posterior instability of the shoulder: a prospective study of 100 shoulders. Am J Sports Med. 34(7):1061–1071. PMID: 16567458. DOI: 10.1177/0363546505285585 3. Schwartz DG, Goebel S, Piper K, Kordasiewicz B, Boyle S, Lafosse L (2013). Arthroscopic posterior bone block augmentation in posterior shoulder instability. J Shoulder Elbow Surg. 22(8):1092–1101. PMID: 23337111. DOI: 10.1016/j.jse.2012.09.011 4. Villefort C, Stern C, Gerber C, Wyss S, Ernstbrunner L, Wieser K (2022). Mid-term to long-term results of open posterior bone block grafting in recurrent posterior shoulder instability: a clinical and CT-based analysis. JSES Int. 7(2):211–217. PMID: 36911764. DOI: 10.1016/j.jseint.2022.12.008 5. Di Giacomo G, Itoi E, Burkhart SS (2014). Evolving concept of bipolar bone loss and the Hill-Sachs lesion: from "engaging/non-engaging" lesion to "on-track/off-track" lesion. Arthroscopy. 30(1):90–98. PMID: 24384275. DOI: 10.1016/j.arthro.2013.10.004 6. Burkhead WZ Jr, Rockwood CA Jr (1992). Treatment of instability of the shoulder with an exercise program. J Bone Joint Surg Am. 74(6):890–896. PMID: 1634579 7. Neer CS 2nd, Foster CR (1980). Inferior capsular shift for involuntary inferior and multidirectional instability of the shoulder. J Bone Joint Surg Am. 62(6):897–908.
Kim's lesion — original description of the concealed posteroinferior labral avulsion
- Case series of 15 shoulders with posterior or multidirectional posteroinferior instability.
- The labrum appeared intact superficially (often only a shallow chondrolabral crack), but probing revealed detachment of the DEEP labrum with loss of labral height and chondrolabral retroversion.
- Treated by converting the concealed lesion to a complete tear, labroplasty to restore height, and capsular shift; 14 of 15 satisfactory at minimum 2 years.
Arthroscopic capsulolabral reconstruction for posterior instability — 100 shoulders
- Prospective cohort: 91 athletes / 100 shoulders with unidirectional recurrent posterior instability, mean follow-up 27 months.
- Mean ASE score improved from 50.4 to 85.7, with significant gains in stability, pain and function.
- 89% returned to sport and 67% to the same level; instability shoulders had significantly greater chondrolabral and osseous retroversion than controls.
Arthroscopic posterior bone block augmentation with iliac crest graft
- 19 arthroscopic posterior iliac-crest bone blocks in 18 patients (trauma, glenoid dysplasia, Ehlers-Danlos, posterior erosion).
- Rowe score improved from 18.4 to 82.1 and Walch-Duplay from 37.4 to 82.9; radiographic bone healing in all cases.
- 9 excellent, 6 satisfied, 3 persistently painful — symptomatic screw prominence resolved with hardware removal in two of these.
Mid-to-long-term results of open posterior bone block — the cautionary data
- 14 patients, open posterior bone block, median 9-year follow-up (range 4–20 years).
- Tested recurrent posterior instability in 31% overall — 50% in atraumatic vs 14% in traumatic cases; major graft resorption (Zhu grade II) in 62%.
- Degenerative joint change progressed by at least one Samilson-Prieto grade in 67%; clinical score improvements were only modest.
Glenoid track and on-track / off-track concept (anterior instability)
- Defines the glenoid track: track width = 0.83 × D minus d (D = glenoid diameter, d = anterior glenoid bone-loss width).
- A Hill-Sachs interval exceeding the track is off-track (will engage) and warrants treating both poles of bipolar bone loss.
- For anterior glenoid loss of 25% or more, glenoid bone grafting is recommended.