Volar approach to the median nerve at the elbow and proximal forearm · four potential compression sites
- Pronator syndrome is a CLINICAL diagnosis — EMG/NCS is often normal, so the diagnosis rests on characteristic volar forearm pain aggravated by pronation, median nerve distribution paraesthesia, and tenderness over the pronator teres.
- Four potential compression sites, proximal to distal (SLAP): ligament of Struthers (rare, 1–3%), lacertus fibrosus, between the heads of pronator teres (most common), and the FDS arch — ALL must be systematically assessed and released.
- Differentiate from carpal tunnel syndrome: forearm pain is prominent (not just hand), pain comes with activity/pronation (not nocturnal), Tinel's at the wrist is negative, and the palmar cutaneous branch may be involved; the two can coexist (double crush).
- The anterior interosseous nerve (AIN) is a pure motor branch arising within the pronator region — it MUST be identified and preserved; injury loses FPL, FDP to index/middle and pronator quadratus (an abnormal OK pinch sign) with no sensory loss.
- A 3–6 month conservative trial is mandatory before surgery; success is 80–90% with a correct diagnosis and complete release — failure is usually misdiagnosis or a missed compression site.
When & Why
Indication. Pronator syndrome — volar forearm pain worse with repetitive pronation and gripping, median nerve distribution paraesthesia (thumb, index, middle, radial half of the ring finger), and tenderness over the pronator teres muscle belly (4–6 cm distal to the elbow crease) — that has failed a minimum 3–6 month conservative trial (rest from provocative activities, NSAIDs, activity modification, and a night splint holding the forearm in supination). The diagnosis is made on history and examination, supported by provocative tests: - Pronator compression test — sustained pronation for 30–60 seconds reproduces symptoms.
- Resisted pronation test — active pronation against resistance causes pain (implicates pronator teres).
- Resisted FDS middle-finger test — isolated FDS contraction reproduces symptoms (implicates the FDS arch).
- Resisted elbow flexion with supination — implicates the lacertus fibrosus.
- Tinel's over the pronator — percussion over the pronator teres elicits paraesthesia. Differentiate pronator syndrome from carpal tunnel syndrome — the single most important preoperative decision, because operating for the wrong diagnosis is the commonest cause of failure:
- Pronator syndrome
- Volar forearm pain prominent
- Carpal tunnel syndrome
- Hand and wrist predominant
- Pronator syndrome
- Worse with activity / pronation
- Carpal tunnel syndrome
- Worse at night and at rest
- Pronator syndrome
- Over pronator teres; wrist Tinel's negative
- Carpal tunnel syndrome
- At the wrist, strongly positive
- Pronator syndrome
- Negative or equivocal
- Carpal tunnel syndrome
- Positive
- Pronator syndrome
- May be involved
- Carpal tunnel syndrome
- Spared (it branches proximal to the carpal tunnel)
- Pronator syndrome
- Often normal (clinical diagnosis)
- Carpal tunnel syndrome
- Typically abnormal, localises to the wrist
- Pronator syndrome
- Pronator compression / resisted pronation / resisted FDS middle finger
- Carpal tunnel syndrome
- Phalen's and Tinel's at the wrist
Electrodiagnostic studies. EMG/NCS is often normal — pronator syndrome remains a clinical diagnosis. When abnormal, it shows slowing of median nerve conduction at the forearm level; its main value is ruling out mimics (cervical radiculopathy C6/C7, brachial plexopathy) and assessing the AIN if isolated motor symptoms are present. The three conditions that must hold before you operate:
A normal EMG does not exclude pronator syndrome. The diagnosis rests on the characteristic history, pronator tenderness and positive provocative tests, with mimics excluded.
A documented 3–6 month trial of rest, NSAIDs, activity modification and a supination splint is mandatory. Operating too early is a classic surgeon trap.
Incomplete release of any one site causes failure. Explore every potential level (SLAP) and confirm the nerve glides freely at the end.
Contraindications. Absolute — an incorrect or unaddressed alternative diagnosis, active infection over the surgical site, or medical unfitness for elective surgery. Relative — an inadequate conservative trial (less than 3 months), chronic severe compression with established muscle atrophy (poor prognosis), coexisting carpal tunnel requiring release (address simultaneously or stage it), and cervical radiculopathy as the primary pathology (double crush — treat the cervical spine first). Preoperative imaging. Plain AP and lateral elbow radiographs to look for a supracondylar process (the bony origin of the ligament of Struthers). MRI of the forearm and ultrasound are optional — they may show muscle oedema, nerve calibre change, or a persistent median artery, and ultrasound allows dynamic assessment during pronation. Consent specifically for persistent or recurrent symptoms (10–20%), medial antebrachial cutaneous nerve injury with volar forearm numbness or a painful neuroma, median nerve or AIN injury (motor loss), brachial artery injury, infection, haematoma, and CRPS. Counsel the patient that recovery is gradual — sensory improvement over weeks to months, motor recovery over 3–6 months, and pain relief potentially taking 6–12 months. Setup. Supine, arm on a hand table, shoulder abducted 90 degrees, elbow extended and forearm fully supinated. General or regional (supraclavicular/axillary) anaesthesia; local alone is inadequate for a complete exploration. Upper-arm tourniquet at 250 mmHg (about 100 mmHg above systolic), exsanguinated with an Esmarch bandage. Loupe magnification is mandatory — nerve and vessel identification is the whole operation.
The Operation
The goal is a systematic decompression of the median nerve at every potential compression site through a single volar exposure, while protecting the brachial artery, the AIN, the motor branches to pronator teres and FCR, and the medial antebrachial cutaneous nerve. The exposure — incision, subcutaneous dissection, identification of the nerve, and release of the lacertus — is the foundation: laid out in full below as the first steps.
Operative sequence
- Supine, hand table, shoulder abducted 90 degrees, elbow extended, forearm fully supinated so the whole volar forearm is exposed from 5 cm proximal to the elbow to mid-forearm.
- Mark the landmarks: the medial epicondyle, the biceps tendon (lateral structure in the antecubital fossa), the pronator teres bulk on the medial forearm, and the palmaris longus tendon distally (it guides the distal incision line).
- Mark a lazy-S / curving incision: starting 2 cm proximal to the elbow flexion crease in the medial antecubital fossa, curving across the crease medial to the biceps tendon, then extending 8–10 cm distally along the medial border of pronator teres toward palmaris longus (total 10–12 cm). The curve avoids a linear scar across the flexion crease (which contractures) and allows proximal extension for a Struthers ligament or distal extension for further FDS exposure.
- Infiltrate along the line with local anaesthetic and epinephrine for haemostasis; incise the skin with a No. 15 blade.
- Careful subcutaneous dissection with tenotomy scissors. Identify and preserve the medial antebrachial cutaneous nerve branches — they arborise throughout the subcutaneous layer (not a single trunk), and injury causes permanent volar forearm dysaesthesia. Preserve the larger branches; some tiny ones are unavoidable, so warn the patient preoperatively about possible numbness.
- Ligate crossing superficial veins (median cubital and forearm veins).
- Incise the antebrachial fascia longitudinally.
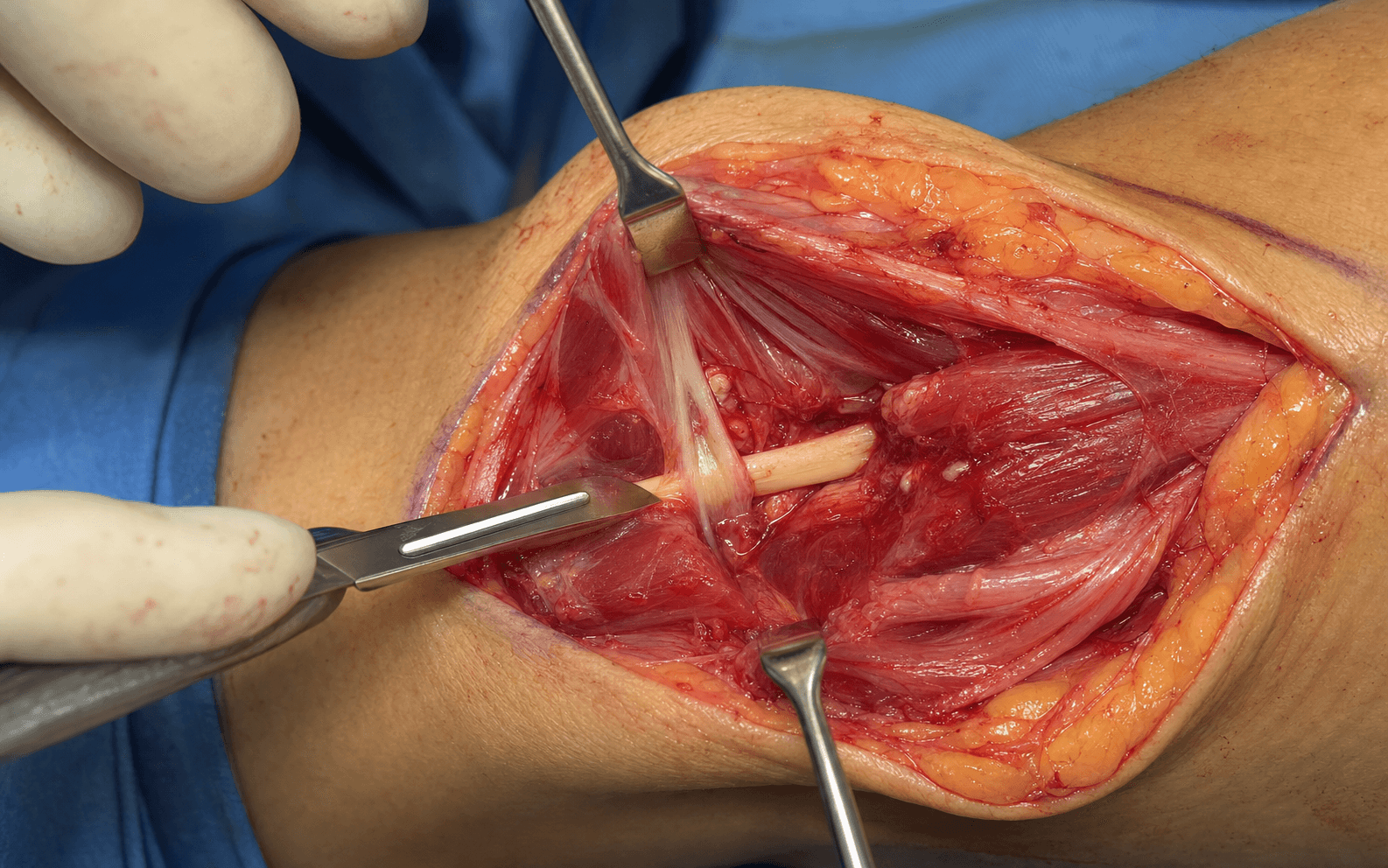
- Identify the brachial artery — pulsatile, the lateral structure in the antecubital fossa. The median nerve lies immediately MEDIAL to the brachial artery (remember: "median nerve is medial to artery"). This relationship is constant even with anatomic variation. If you find the artery, you find the nerve.
- Palpate the nerve — it feels like a firm cord, distinct from soft muscle. Pass a vessel loop around it proximally for identification and gentle retraction, and trace it distally through the field.
- Identify the lacertus fibrosus — a white, shiny fascial band (the bicipital aponeurosis) expanding from the biceps tendon and crossing medially over the nerve. Present in about 90% of people, it acts as a fascial "roof" compressing the nerve.
- Release it with scissors or knife along its MEDIAL edge — stay away from the biceps tendon laterally to avoid cutting the tendon.
- Divide it longitudinally and completely; the nerve should be visibly freed from the overlying band. Inspect for aberrant crossing vessels and ligate any that are compressive.
- If the preoperative X-ray showed a supracondylar process, extend the exposure proximally.
- Palpate for the bony spur on the anteromedial distal humerus about 5 cm proximal to the medial epicondyle, and identify the ligament running from the spur to the medial epicondyle — together they form an osteo-fibrous tunnel carrying the median nerve and brachial artery.
- Release the ligament sharply from its epicondylar insertion; remove a prominent bony spur with a rongeur if needed. Rare (1–3% of the population) but if present and not released, the operation is guaranteed to fail.
- Identify the pronator teres with its two heads: the humeral head (superficial, larger, from the medial epicondyle) and the ulnar head (deep, smaller, from the coronoid process).
- The median nerve passes between the two heads in 80% of people (anterior to both in 20%). Gently separate the heads along their natural intermuscular plane with blunt dissection — do NOT divide the muscle bellies.
- Follow the nerve through the "pronator tunnel" between the heads and release any constricting fibrous bands. This is the single most common compression site.
- As the nerve is traced through the pronator region, identify the AIN branching from the median nerve, typically 4–8 cm distal to the lateral epicondyle. The AIN is a pure motor branch — it dives deep (dorsally) toward the interosseous membrane to supply FPL, FDP to index/middle, and pronator quadratus.
- Pass a vessel loop around the AIN for identification, and mark its course before releasing the FDS arch distally. Test AIN function at the end with the OK pinch sign and index-finger DIP flexion.
- Follow the median nerve distally beyond the pronator teres to the FDS. Identify the FDS arch — the fibrous arch at the FDS origin from the anterior oblique line of the radius, 4–5 cm distal to the elbow crease. The nerve passes UNDER this arch.
- Release the arch completely with scissors through a longitudinal incision, with the AIN under direct vision and protected.
- Do not under-estimate it: although classic teaching (Johnson, 1979) ranks the pronator teres first, the Olehnik series found the FDS arch was the single most frequent intraoperative compression site (22 of 39 limbs), so it must never be omitted.
- Systematically confirm all sites are released — Struthers (if present), lacertus divided, pronator heads separated with the nerve mobile, FDS arch released.
- Dynamic test: passively pronate/supinate the forearm and flex/extend the elbow while watching the nerve — it should glide smoothly without catching or kinking at any site. If it catches, the release is incomplete.
- Assess nerve appearance: normal is pink and pliable; pale suggests chronic ischaemia, dusky suggests venous congestion, indurated suggests fibrosis (poorer recovery prognosis). For severe scarring, a gentle external neurolysis is acceptable; avoid internal neurolysis (opening the epineurium), which risks further injury.
- Inspect for a persistent median artery accompanying the nerve — an anatomic variant present in 10–20% of the population (a remnant of the embryonic vascular system that normally regresses).
- If it is enlarged or thrombosed and compressing the nerve, ligate it proximally and distally and excise the segment; then check hand perfusion (Allen test, pulse oximetry), which should be normal via the radial and ulnar collaterals.
- Release the tourniquet, allow reperfusion, and obtain meticulous haemostasis with bipolar cautery — a haematoma compresses the nerve and causes adhesions.
- Copious saline irrigation. Close the antebrachial fascia loosely with 2-0 absorbable suture (Vicryl) — tight fascial closure recreates the compression; some surgeons leave it open.
- Subcutaneous layer with 3-0 absorbable suture; skin with 4-0 nylon interrupted or 4-0 Monocryl subcuticular.
- NO drain — drains cause adhesions around the nerve and risk direct injury. A posterior splint is optional for comfort only (elbow at 90 degrees, forearm neutral), removed at 3–7 days.
The brachial artery is the key to finding the nerve and the structure most at risk in the proximal dissection. It is always pulsatile and always lateral in the antecubital fossa, with the median nerve immediately medial. Identify it early, place a vessel loop, and maintain gentle retraction. Avoid blind cautery near it. If injured: direct pressure, primary repair of a clean laceration (or a vein graft for extensive injury), vascular surgery help, and postoperative compartment monitoring with fasciotomy if a compartment syndrome develops.
The AIN branches from the median nerve within the pronator region (4–8 cm distal to the lateral epicondyle) and dives deep toward the interosseous membrane. It is a pure motor nerve, so an injury may not be noticed by the patient immediately but causes permanent loss of FPL and FDP function. Identify it with a vessel loop and keep it under direct vision during all distal (FDS arch) dissection. Test the OK pinch sign at the end.
"Median nerve is Medial to the artery." The brachial-artery–median-nerve relationship in the antecubital fossa is constant regardless of anatomic variation. The artery is always pulsatile and always lateral — identify it first and the nerve lies immediately medial.
The curved lazy-S incision avoids a straight scar crossing the flexion crease (which contractures) and gives access to all four compression sites with extension in either direction. Never place a drain — it causes adhesions around the decompressed nerve and risks direct nerve injury. Haemostasis after tourniquet release and a loose (or open) fascial closure are what prevent a recurrent compressive haematoma.
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 | 0–1 week | Bulky compressive dressing; optional posterior splint (elbow 90 degrees, forearm neutral) removed at 3–7 days | Elevation; finger active range of motion only | | 2 | 1–6 weeks | No splint (or for comfort only) | Gentle active ROM of elbow, forearm pronation/supination, wrist and fingers; no strengthening; no lifting greater than 1 lb; scar massage once sutures are out | | 3 | 6–12 weeks | — | Progressive strengthening (Theraputty, grippers); full ADLs; return to desk work; no heavy lifting greater than 5–10 lb | | 4 | 3–12 months | — | Full unrestricted activity by 3 months; heavy manual work or overhead athletes may need 4–6 months; maximal medical improvement around 12 months | Sensory symptoms (paraesthesia) usually improve first over weeks to months, motor recovery (if weakness was present) over 3–6 months, and forearm pain resolves gradually, sometimes taking 6–12 months for complete relief. Around 80–90% report good to excellent results with a correct diagnosis and complete release; sensory recovery is the most reliable, and motor recovery is excellent if the AIN is preserved. Red flags requiring urgent review: increasing wound drainage, erythema or fever (infection); a new or worsening median nerve deficit (surgical complication); severe pain out of proportion (CRPS, compartment syndrome, or haematoma); and no improvement by 3–6 months (reconsider the diagnosis or an incomplete release). Complications
- Recognition
- No improvement in forearm pain or paraesthesia at 3–6 months; the commonest complication, usually a diagnostic error or missed site
- Prevention
- Thorough preoperative workup, confirm the clinical diagnosis, rule out cervical and carpal tunnel pathology, adequate conservative trial
- Management
- Reassess the diagnosis; EMG/NCS; consider double crush (concomitant CTS); revision only if objective incomplete release is shown
- Recognition
- New or worsened median motor (APB, FPL, thenar) or sensory loss, recognised in recovery
- Prevention
- Gentle handling, avoid excessive traction, vessel-loop identification, sharp dissection under direct vision, no cautery near the nerve
- Management
- Grade the injury; immediate complete deficit may warrant re-exploration; observe partial/delayed deficits with serial exams and EMG at 3–4 weeks; tendon transfers if no recovery
- Recognition
- Loss of thumb IP flexion (FPL), weak index/middle DIP flexion (FDP), weak pronation (PQ); cannot make the OK sign; no sensory loss
- Prevention
- Identify and mark the AIN with a vessel loop before FDS arch release; maintain visualisation and protect it during distal dissection
- Management
- Intraoperative laceration: repair; postoperative deficit: observe (neurapraxia may recover over 3–6 months), EMG at 6–12 weeks; tendon transfers rarely needed
- Recognition
- Dysesthesia or numbness over the volar/medial forearm; Tinel's over the incision; possible painful neuroma
- Prevention
- Meticulous subcutaneous dissection, identify and preserve all visible branches, loupe magnification, gentle tissue handling
- Management
- Mostly neurapraxia resolving over weeks–months; desensitisation and gabapentin/pregabalin for neuroma pain; refractory cases: neuroma excision and burial
- Recognition
- Pulsatile bleeding intraoperatively; postop hand ischaemia (pale, cool, no radial pulse) or compartment syndrome
- Prevention
- Identify and protect the artery early, gentle retraction, sharp dissection under vision, bipolar near vessels, no blind cautery
- Management
- Intraoperative: primary repair or vein graft, vascular help; postop: immediate re-exploration, heparin, monitor compartments and fasciotomy if needed
- Recognition
- Erythema, swelling, warmth, purulent drainage, fever, raised inflammatory markers; usually 3–14 days postop
- Prevention
- Preoperative cefazolin, sterile technique, haemostasis, gentle handling, sound closure
- Management
- Superficial: oral cephalexin; deep: IV antibiotics, surgical debridement and cultures; add MRSA cover if risk factors
- Recognition
- Postop swelling, ecchymosis, tense forearm; a large haematoma can recompress the median nerve
- Prevention
- Meticulous haemostasis after tourniquet release, ligate vessels, bipolar cautery, manage anticoagulants perioperatively, compressive dressing
- Management
- Small: observe, elevate, ice; large or expanding with compression/infection risk: surgical evacuation; restart anticoagulation when safe
Additional complications. Motor weakness — pronator teres (from dividing rather than separating the muscle), FCR (proximal motor branch injury), or the flexor mass (over-aggressive FDS arch release); manage with hand therapy and strengthening, usually recovers. Forearm and elbow stiffness from excessive immobilisation or scar adhesions — prevent with early motion within 3–7 days; treat with aggressive therapy, dynamic splinting, and occasionally manipulation under anaesthetic. CRPS (rare, 2–5%) — disproportionate pain, swelling and vasomotor changes; early recognition and treatment with hand therapy, gabapentin/pregabalin, sympathetic blocks and vitamin C. Recurrent compression from incomplete initial release or scar around the nerve — re-exploration with complete release and possible nerve transposition, accepting that revision surgery has a worse prognosis.
Viva & Exam Focus
SLAPFour compression sites — SLAP
OKAIN function — the OK sign
Critical structures to protect
Lateral in the antecubital fossa, median nerve immediately medial. Identify the pulsatile vessel early, place a vessel loop, maintain gentle retraction. Laceration during lacertus release or nerve dissection causes major bleeding.
Branches from the median nerve 4–8 cm distal to the lateral epicondyle within the pronator region, diving deep dorsally. Identify with a vessel loop and mark its course before releasing the FDS arch. Injury causes permanent motor loss (FPL, FDP index/middle, PQ).
Multiple arborising branches throughout the subcutaneous layer, especially medially. Meticulous subcutaneous dissection; preserve all visible branches. Injury causes permanent dysaesthesia or a painful neuroma over the volar forearm.
Arise from the median nerve proximal to the pronator heads and enter the muscles from the deep surface. Avoid aggressive lateral dissection; separate the pronator heads gently along their natural plane. Injury causes pronator or FCR weakness.
Lateral structure in the antecubital fossa; the lacertus fibrosus arises from its medial edge. Release the lacertus along its MEDIAL border and stay off the tendon proper. Division during lacertus release causes biceps weakness or rupture.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 42-year-old carpenter presents with 6 months of volar forearm pain worse with repetitive pronation. EMG is normal. How do you differentiate pronator syndrome from carpal tunnel syndrome, and what is your management?”
“During pronator syndrome release, you are about to release the FDS arch. Describe the four compression sites, the anatomy of pronator teres, and how you identify and protect the anterior interosseous nerve.”
“You perform a pronator syndrome release and at 6 months the patient has no improvement. What are your differentials and how do you approach this failure?”
Indications
- Clinical diagnosis: volar forearm pain + median paraesthesia + pronator tenderness + failed 3–6 month conservative trial
- Positive provocative tests: pronator compression, resisted pronation, resisted FDS middle finger
- EMG often NORMAL (unlike CTS) — diagnosis is clinical
- Differentiate from CTS: forearm pain prominent, worse with activity, Tinel's at wrist negative
Key anatomy & four sites
- SLAP: Struthers (rare 1–3%), Lacertus fibrosus, pronator teres between heads, Proximal FDS arch
- Median nerve MEDIAL to the brachial artery in the antecubital fossa (constant landmark)
- Pronator teres: humeral (medial epicondyle) + ulnar (coronoid) heads; nerve between in 80%
- AIN (pure motor) branches 4–8 cm distal to the lateral epicondyle: FPL + FDP index/middle + PQ
- Persistent median artery (10–20%) can compress the nerve if thrombosed
Critical steps
- Lazy-S incision 2 cm proximal to the elbow crease, 8–10 cm distally along the medial pronator border
- Identify the brachial artery (pulsatile, lateral); median nerve immediately medial; vessel loop
- Release the lacertus along its MEDIAL edge (avoid the biceps tendon)
- Check the X-ray for Struthers; release if present
- Separate the pronator heads gently (don't divide muscle)
- Identify the AIN with a vessel loop BEFORE releasing the FDS arch
- Release the FDS arch completely; verify the nerve glides with pronation/supination
- LOOSE fascial closure (don't recreate compression); NO drain
Danger structures
- Brachial artery: lateral; protect with gentle retraction
- AIN: branches within the pronator region, dives deep — vessel loop, protect during FDS release
- Medial antebrachial cutaneous nerve: arborising subcutaneous branches — preserve
- Motor branches to pronator/FCR: arise proximally — preserve during lacertus release
- Biceps tendon: lateral; release the lacertus medially only
Complications
- Persistent symptoms (10–20%): usually diagnostic error or incomplete release
- AIN injury: loss of FPL, FDP index/middle, PQ — abnormal OK sign, no sensory loss
- Median nerve injury, MABC injury, brachial artery injury, infection, haematoma, CRPS (2–5%)
- Double crush: coexisting CTS or cervical pathology — treat both sites
Post-op & outcomes
- Splint optional 3–7 days; early ROM encouraged
- Weeks 1–2 gentle active ROM, no strengthening; weeks 3–6 progressive strengthening and desk work
- Recovery: sensory first (weeks–months), motor 3–6 months, pain gradual up to 6–12 months
- 80–90% good–excellent with correct diagnosis and complete release
- No improvement by 3–6 months: reconsider diagnosis or incomplete release
Background & Evidence
Relevant anatomy. The median nerve enters the antecubital fossa medial to the brachial artery, passes beneath the lacertus fibrosus, then between the two heads of pronator teres (humeral head from the medial epicondyle, ulnar head from the coronoid) in 80% of people (anterior to both in 20%), and finally beneath the FDS arch at the radial origin of FDS, 4–5 cm distal to the elbow crease. Within the pronator region it gives off the anterior interosseous nerve — a pure motor branch that dives dorsally to supply FPL, FDP to index/middle and pronator quadratus, with no cutaneous supply. Motor branches to pronator teres (entering from the deep surface), FCR, palmaris longus and FDS arise along this course. The persistent median artery, an embryonic remnant present in 10–20% of people, accompanies the nerve into the forearm and can compress it when enlarged or thrombosed. The four potential compression sites — the anatomical framework of the disease and the checklist for a complete release:
- Anatomy
- Supracondylar process to medial epicondyle; an osteo-fibrous tunnel carrying the median nerve and brachial artery
- Frequency / notes
- Rare (1–3%); check the preoperative elbow X-ray for the supracondylar process
- Anatomy
- Bicipital aponeurosis from the biceps tendon crossing medially over the nerve
- Frequency / notes
- Present in about 90%; the proximal fascial 'roof'
- Anatomy
- Humeral head (medial epicondyle) + ulnar head (coronoid); nerve passes between in 80%
- Frequency / notes
- Most common site by classic teaching (Johnson, 1979)
- Anatomy
- Fibrous arch at the FDS origin from the anterior oblique line of the radius, 4–5 cm distal to the elbow
- Frequency / notes
- Most frequent intraoperative site in the Olehnik series (22 of 39 limbs)
Epidemiology. Pronator syndrome is far less common than carpal tunnel syndrome and is a diagnosis of exclusion. It affects adults in the working decades, often those whose activities involve repetitive pronation and gripping, and bilateral or double-crush presentations (with carpal tunnel syndrome or cervical radiculopathy) are well recognised. Key evidence. The landmark Hartz (1981) Mayo Clinic series of 39 patients (36 forearms explored) defined the clinical picture — pronator tenderness aggravated by resisted pronation — and showed electrophysiology was abnormal in only a few and rarely localised the lesion (a clinical diagnosis); 28 of 36 operations gave good or excellent results, with failure driven by inadequate decompression or misdiagnosis. Johnson (1979) established the framework of multiple discrete compression levels (in descending frequency pronator teres, FDS arch, lacertus fibrosus) and the level-specific provocative tests, with only 4 of 51 surgical cases failing at up to 19 years. Olehnik (1994) found the FDS tendon arch was the single most frequent intraoperative site (22 of 39 limbs), and that 19 limbs had a prior failed ipsilateral carpal tunnel release (the double-crush cohort), 14 of whom improved — so the FDS arch must never be omitted. Ahmad (2023) showed that an isolated lacertus release through a 2 cm incision under WALANT dropped mean QuickDASH from 53 to 7.8, supporting a tailored, level-specific decompression. Lee and LaStayo (2004) anchored the mandatory conservative trial and structured differentiation from carpal tunnel syndrome before committing to surgery.
References
The pronator teres syndrome: compressive neuropathy of the median nerve
- Landmark Mayo Clinic series of 39 patients; 36 forearms surgically explored over a seven-year period
- Distinctive finding was tenderness over the proximal pronator teres, aggravated by resisted pronation, resisted elbow flexion and occasionally resisted FDS contraction to the long finger
- Electrophysiology was abnormal in only a few patients and rarely localised the lesion, reinforcing that this is a clinical diagnosis
- 28 of 36 operations gave good or excellent results, 5 fair, 3 unchanged; the cause of failure was inadequate decompression or misdiagnosis
Median nerve entrapment syndrome in the proximal forearm
- Series of 71 cases over 20 years, 51 treated surgically, describing the foundational provocative stress tests for each compression level
- In every surgically treated limb the median nerve was compressed at one of three levels, in descending frequency: pronator teres, FDS (sublimis) arch, then lacertus fibrosus
- Three provocative stress tests localise the level: resisted pronation (pronator teres), resisted long-finger FDS (FDS arch), and resisted elbow flexion with supination (lacertus fibrosus)
- Only four of 51 surgical cases were considered failures with follow-up to 19 years
Median nerve compression in the proximal forearm
- 39 limbs in 36 patients decompressed; 19 limbs had a prior failed ipsilateral carpal tunnel release (double-crush cohort)
- Most common physical finding was a positive pronator compression test; elbow-to-wrist conduction was abnormal in only 12 of 37 tested limbs
- Intraoperative compression was at the FDS tendon arch in 22 limbs, pronator teres in 13, and both in 4 — the FDS arch was the single most frequent site in this cohort
- 30 of 39 limbs had complete or partial relief; 14 of 19 limbs with prior failed carpal tunnel release improved
Lacertus syndrome: an outcome analysis after lacertus release
- 93 patients with isolated lacertus syndrome (a proximal subset of pronator syndrome) released through a 2 cm incision under WALANT
- Mean QuickDASH fell from 53 preoperatively to 7.8 immediately and 10.6 at six months (p less than 0.001)
- Mean grip strength rose from 16 kg to 24 kg and pinch from 9 kg to 13 kg (both p less than 0.001)
- Demonstrates reproducible, durable relief from a focused, minimally invasive release of a single proximal compression point
Pronator syndrome and other nerve compressions that mimic carpal tunnel syndrome
- Comprehensive clinical commentary differentiating proximal median nerve compressions (pronator and anterior interosseous syndromes) from carpal tunnel syndrome
- Diagnosis rests on symptom pattern, distribution of paraesthesia and specific patterns of muscle weakness rather than electrodiagnostics
- Recommends a conservative trial — rest/immobilisation, modalities and nerve-gliding — before considering surgical release
- Emphasises suspecting proximal compression when a presumed carpal tunnel fails conservative or surgical treatment
Further reading 1. Andreisek G, Crook DW, Burg D, Marincek B, Weishaupt D. Peripheral neuropathies of the median, radial, and ulnar nerves: MR imaging features. Radiographics. 2006;26(5):1267-1287. doi:10.1148/rg.265055712 2. Bridgeman C, Naidu S, Kothari MJ. Clinical and electrophysiological presentation of pronator syndrome. Electromyogr Clin Neurophysiol. 2007;47(2):89-92. 3. Dang AC, Rodner CM. Unusual compression neuropathies of the forearm, part I: radial nerve. J Hand Surg Am. 2009;34(10):1906-1914. doi:10.1016/j.jhsa.2009.10.016 4. Mackinnon SE, Novak CB. Compression neuropathies. In: Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH, Cohen MS, eds. Green's Operative Hand Surgery. 7th ed. Elsevier; 2017:903-962. 5. Spinner M. The arcade of Struthers. J Bone Joint Surg Br. 1968;50(4):809-812. 6. Tsai P, Steinberg DR. Median and radial nerve compression about the elbow. Instr Course Lect. 2008;57:177-185.