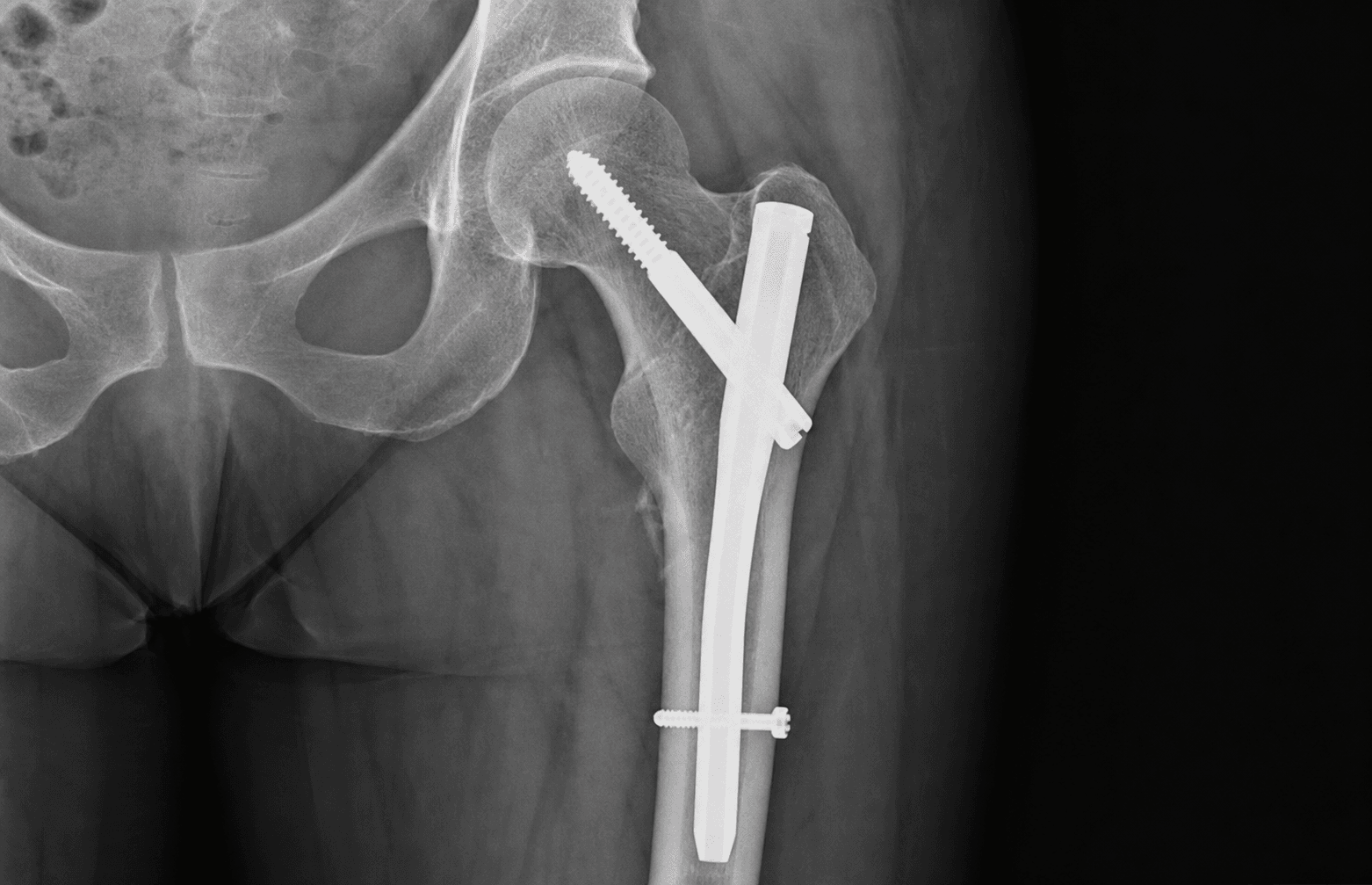
Percutaneous greater-trochanter entry on a fracture table · AO/OTA 31-A2–A3
- Tip-apex distance (TAD) must be less than 25mm — the sum of the screw-tip-to-head-apex distances on the AP and lateral radiographs — and is the single most important predictor of cut-out (Baumgaertner).
- Place the cephalic screw center-center or inferior-center on BOTH views; superior placement has the highest cut-out risk. Aim 5–10mm from subchondral bone.
- Lateral wall thickness less than about 20mm (the Hsu threshold is 20.5mm) means an unstable pattern — use a LONG nail, not an isolated sliding hip screw.
- Accept anatomic or slight valgus reduction with medial cortical support restored; varus is NOT acceptable and drives cut-out.
- Entry point is at or just medial to the greater trochanter tip on AP, and ALIGNED WITH THE FEMORAL CANAL on lateral — confirm on both views before reaming.
- Leave the nail flush or 5–10mm proud of the greater trochanter tip — never bury it below the tip, as this makes later removal extremely difficult.
When & Why
Indication. A cephalomedullary nail (CMN) is the implant of choice for the unstable intertrochanteric (peritrochanteric) fracture — patterns where the lateral wall is deficient, where the fracture line runs in reverse obliquity, or where it extends into the subtrochanteric region. For a simple, stable two-part trochanteric fracture with an intact lateral wall, the sliding hip screw (SHS) remains an excellent, lower-complication option (Parker and Handoll, Cochrane). The nail wins once medial or lateral cortical support is lost.
Unstable intertrochanteric fractures (AO 31-A2.2, A2.3, A3), reverse obliquity patterns (medial cortex proximal), intertrochanteric fractures with subtrochanteric extension, pathological intertrochanteric fractures, and ipsilateral femoral neck and shaft fractures.
Stable intertrochanteric fractures (AO 31-A1, A2.1) in younger patients, failed dynamic hip screw requiring conversion, lateral wall thickness less than 20mm, and severely osteoporotic bone requiring better load sharing.
Absolute: active infection at the surgical site, inadequate bone stock precluding screw fixation (consider arthroplasty), and severe medical comorbidities precluding surgery. Relative: previous ipsilateral femoral instrumentation, severe deformity preventing nail passage, and a very narrow canal (less than 8mm).
Pre-operative imaging. An AP pelvis (fracture pattern, lateral wall thickness, pelvic ring injury), AP and lateral hip (AO classification, comminution, neck-shaft angle), the contralateral hip (template nail size, normal anatomy for comparison) and a full-length femur (rule out shaft extension, plan nail length). The four measurements that change the operation are lateral wall thickness, neck-shaft angle (normal 125–135°), femoral canal diameter at the isthmus (selects nail diameter), and femoral length (compared with the contralateral side). The one decision that matters — short or long nail. Everything else follows the fracture pattern:
- Typical length
- 170–240mm (typically 220–240mm), terminating in the metaphysis
- Use when
- Isolated intertrochanteric fracture, stable AO 31-A1 or A2.1, intact lateral wall more than 20mm, no subtrochanteric extension
- Avoid when
- Lateral wall comminution, reverse obliquity, subtrochanteric extension, pathological fracture
- Typical length
- 340–420mm (typically 360–380mm), terminating 3–4cm above the knee
- Use when
- Lateral wall less than 20mm, subtrochanteric extension, reverse obliquity, pathological fractures, ipsilateral neck-shaft fractures
- Avoid when
- A genuinely stable pattern with an intact wall, where a short nail suffices and saves distal locking time
The Operation
The goal: reduce the fracture closed on the table, enter through the greater trochanter percutaneously, pass a nail down the canal, and lock a cephalic screw or blade into the femoral head with a tip-apex distance less than 25mm — restoring length, rotation and medial support so the patient can bear weight immediately. The exposure is a percutaneous greater-trochanter entry with a minimal 5cm incision.
Operative sequence
- Position supine on the fracture table with a well-padded perineal post, affected leg in the traction boot, unaffected leg in hemilithotomy or extended.
- Apply gentle longitudinal traction (typically 10–20kg) and internally rotate the leg 10–15° to correct the typical external rotation deformity of the distal fragment.
- Assess reduction on AP and lateral fluoroscopy. Acceptable reduction: anatomic or slight valgus (5–10° valgus acceptable, varus is NOT), restoration of medial cortical continuity, no posterior sag on the lateral view, and rotation corrected.
- If closed reduction fails, use a percutaneous Schanz-pin joystick in the greater trochanter or a small incision for a pointed reduction clamp on the medial cortex; accept an imperfect reduction only if medial support is achieved.
- Pitfalls: over-distraction (non-union risk), persistent varus (the major cut-out risk), posterior sag causing an apex-posterior deformity, pudendal nerve compression from a poorly padded post, and iatrogenic femoral neck or sciatic injury from forceful manipulation.
- Palpate the greater trochanter tip — the most prominent lateral point — and make a 5cm longitudinal incision centered over it, extending proximally.
- Incise subcutaneous tissue and the fascia lata (iliotibial band) in line, then split the gluteus medius and minimus fibers bluntly in line with their fibers, avoiding excessive splitting.
- Entry point is critical. For a trochanteric-entry nail (most modern nails) aim for the tip of the greater trochanter or 2–3mm medial to it; for a piriformis-entry nail, enter the piriformis fossa about 1cm medial to the tip.
- On AP, entry is at the tip or just medial — too lateral causes varus, too medial risks medial cortex perforation or valgus. On the LATERAL view the entry MUST be in line with the center of the femoral canal — too anterior perforates the anterior cortex, too posterior the posterior cortex.
- Pitfalls: a lateral entry (varus, the common error), a medial entry (valgus or medial perforation), superior gluteal nerve injury if dissection extends more than 3cm proximal to the tip, and splitting the trochanter and disrupting the abductor insertion.
- Create the entry portal with a T-handle awl or powered entry reamer: for trochanteric entry open the cancellous bone of the tip; for piriformis entry find the fossa medial to the tip.
- Hold the instrument perpendicular to the lateral cortex and advance with controlled force through the cortex into the medullary canal, using gentle rotational movements — do not force it.
- Confirm on lateral fluoroscopy that the trajectory is toward the center of the canal, and feel for cortical breakthrough indicating entry into the canal.
- Pitfalls: anterior or posterior cortex perforation from a wrong trajectory, creating a false passage outside the canal, splitting or fracturing the greater trochanter, damage to the abductor insertion, and propagating the fracture pattern.
- Select a ball-tipped guidewire (typically 3mm) and insert it through the portal into the canal, advancing with gentle rotational movements to cross the fracture into the distal fragment.
- Aim for the CENTER of the canal on both AP and lateral — an eccentric wire leads to an eccentric nail and malalignment.
- Check the wire is central at entry, central at the fracture site, and central distally, parallel to the cortices, terminating 3–4cm above the knee joint to allow length measurement.
- Confirm reduction is maintained after wire passage; if it is lost, remove the wire, re-reduce and re-pass — do not proceed with a poor reduction.
- Pitfalls: the wire taking a false passage, eccentric placement, loss of reduction during passage, distal anterior cortex perforation, advancing the wire into the knee joint, and fracture distraction.
- With the guidewire in final position, measure nail length from entry point to distal extent using a measuring device or a fluoroscopic ruler with magnification correction.
- Short nail 170–240mm terminating in the metaphysis; long nail 340–420mm terminating 3–4cm above the knee joint.
- Choose SHORT for stable patterns (A1, A2.1) with an intact lateral wall more than 20mm and no subtrochanteric extension; choose LONG for unstable patterns, lateral wall comminution less than 20mm, subtrochanteric extension, reverse obliquity and pathological fractures.
- Select diameter from the isthmus (typically 10–11mm) and mark insertion depth on the guidewire.
- Pitfalls: a nail too short (stress riser and risk of distal femur fracture), too long (knee impingement and anterior knee pain), the wrong type for the pattern, or a diameter too large (intraoperative fracture) or too small (inadequate stability).
- Most intertrochanteric fractures are REAMED for better cortical contact and rotational stability; reaming is reserved against only for severe chest injury (fat-embolism concern), very comminuted fractures or bleeding disorders.
- Use sequential flexible reamers over the guidewire, starting about 1mm larger than the isthmus and increasing in 0.5mm increments to a final diameter 1–1.5mm larger than the nail.
- Ream to cortical chatter (the vibration of cortical contact) with copious irrigation to prevent heat necrosis, and monitor the guidewire continuously so it does not advance.
- Pitfalls: fat embolism (more common with long nails and bilateral procedures), heat necrosis without irrigation, guidewire advancement or loss of position, cortical perforation, distal fracture propagation and intraoperative fracture if reaming is too aggressive.
- Mount the nail on the insertion jig with the anteroposterior curvature matching the femoral bow (apex anterior) and the nail fully seated on the jig.
- Insert over the guidewire with gentle rotational movements and controlled mallet blows — never excessive force.
- Advance to the predetermined depth: the nail should be flush with the greater trochanter tip or 5–10mm proud. NEVER bury it below the tip — removal later becomes extremely difficult.
- Confirm on AP and lateral that the nail is centered in the canal, crosses the fracture centrally with reduction maintained, and shows no cortical perforation.
- Pitfalls: inserting the nail backwards (wrong orientation, malalignment), burying it too deep, leaving it too proud (prominence, abductor irritation), anterior cortex perforation where curvature does not match the bow, fracture distraction, and loss of reduction or splitting of the proximal fragment during insertion.
- Using the targeting jig attached to the nail, insert the guidewire for the cephalic screw at the nail's CCD angle (typically 130–135°).
- Target position: center-center or inferior-center in the femoral head on BOTH AP and lateral. Use the 3x3 grid (superior/center/inferior on AP; anterior/center/posterior on lateral). Center-center is optimal, inferior-center is acceptable, and superior placement is AVOIDED (highest cut-out risk).
- Aim for DEEP placement, 5–10mm from subchondral bone on all views; too shallow gives inadequate purchase, too deep penetrates the joint.
- Tip-apex distance (TAD). Measure the distance from the screw tip to the apex of the femoral head on AP, and again on lateral, correct for magnification, and SUM them. TAD MUST be less than 25mm. In Baumgaertner's series NONE of the 120 screws with a TAD of 25mm or less cut out, and the cut-out rate rose steeply as TAD increased (mean 24mm in healed fractures versus 38mm in cut-outs).
- Ream over the guidewire to the measured depth; insert the helical blade (compress if the system allows) or lag screw (typically 85–95mm), confirm final position on both views, recheck TAD, and confirm no joint penetration.
- Pitfalls: superior or superior-posterior placement (the highest-risk quadrant), a TAD greater than 25mm (exponentially more cut-out), joint penetration, anterior or posterior neck perforation (check lateral), a screw too short or too long, iatrogenic neck fracture from multiple attempts, and Z-effect or reverse Z-effect (the screw backing out with loading).
- Distal locking controls rotation and length. Decide between static and dynamic locking.
- Short nail: typically one or two static distal locking screws through the targeting jig, inserted through stab incisions, with bicortical purchase confirmed on fluoroscopy.
- Long nail: STATIC locking with two screws (distal and middle holes) for subtrochanteric involvement or unstable patterns needing rigid fixation; DYNAMIC locking with one distal screw only for a pure intertrochanteric fracture, allowing axial compression at the fracture site.
- Confirm screw trajectory through the jig or freehand with fluoroscopy, drill both cortices, measure length, and insert screws to engage both cortices, confirming they pass through the nail.
- Pitfalls: screws missing the nail holes (no rotational control), unicortical purchase, screws too long (far-cortex prominence, soft-tissue or possible vascular injury) or too short, the wrong locking mode for the pattern (dynamic for an unstable fracture loses fixation), thermal necrosis from drilling without irrigation, and fracture at the screw sites.
- Remove the guidewire; if a helical blade system with compression is used, apply compression with the set screw.
- Run a systematic final fluoroscopy check: (1) reduction maintained (anatomic or slight valgus, medial support, no posterior sag); (2) nail centered on AP and lateral at the correct depth (flush or 5–10mm proud); (3) cephalic screw center-center or inferior-center with TAD less than 25mm, 5–10mm from subchondral bone and no joint penetration; (4) distal screws through the nail with bicortical engagement; (5) no cortical perforation along the nail; (6) leg length within 1cm of the contralateral side; (7) rotation matched (patella forward with the leg neutral).
- Release traction gradually and recheck stability and alignment — some settling is acceptable. Irrigate copiously, close the fascia lata and subcutaneous layer with absorbable sutures, close the skin with staples or sutures, and apply a sterile dressing. Save final AP and lateral images showing all implants (including the TAD measurement) for the record.
- Pitfalls: unrecognized joint penetration, malrotation or leg-length discrepancy, loss of reduction on traction release (instability), persistent varus, unrecognized cortical perforation and inadequate documentation.
Exits the sciatic notch 3–5cm proximal to the greater trochanter tip and runs between gluteus medius and minimus. Keep the entry point at or below the tip, avoid dissection more than 3cm above it, and split the gluteal muscles only in line with their fibers.
Exits the pelvis through the greater sciatic notch about 5cm posterior to the trochanter at the hip joint level. Avoid posterior dissection and posterior retractors, handle fracture manipulation carefully in external rotation, and monitor nerve function post-operatively.
Lies on the medial neck and gives the retinacular vessels supplying the femoral head (the posterior-superior branch is most important). Minimize soft-tissue stripping around the fracture, keep the guidewire and cephalic screw intraosseous, and avoid multiple screw attempts.
Crosses the ASIS and runs lateral to sartorius with a variable course anterior to the hip. Use a percutaneous technique with a small incision centered over the greater trochanter (not anterior) and blunt dissection only when necessary.
Inserts on the greater trochanter (medius on the lateral facet, minimus on the anterior facet). Split the muscles in line with their fibers, avoid excessive lateral dissection, keep the entry at the tip or just medial to avoid splitting the trochanter, and repair any significant tear.
Compressed against a poorly padded perineal post on the fracture table, causing post-operative numbness or pain. Pad the post well with gel, limit traction time, and check pressure areas after positioning.
Cut-out is the most common mechanical failure (2–6%) and is almost always avoidable. It is prevented by an acceptable (non-varus) reduction with medial support, a correct entry point confirmed on the lateral view, and a cephalic screw that is center-center or inferior-center on both views with a tip-apex distance less than 25mm. A TAD greater than 25mm, a superiorly placed screw or a varus reduction each multiply the risk — never accept any of them.
Surgeons check the AP entry but forget the lateral. The entry point must be aligned with the CENTER of the femoral canal on the lateral view — too anterior perforates the anterior cortex, too posterior the posterior cortex, and a malaligned entry propagates into a malaligned nail. Confirm the entry on BOTH views before creating the portal; this single check prevents most malalignment.
Leave the nail flush with the greater trochanter tip or 5–10mm proud. A nail buried below the tip sits beneath soft tissue and bone and becomes extremely difficult to remove at any future re-operation. A nail left too proud irritates the abductors and iliotibial band. The 5–10mm-proud position is the sweet spot — confirm it on the lateral before locking.
Aftercare & Complications
Rehabilitation | Phase | Timing | Weight bearing | Therapy & follow-up | |-------|--------|----------------|---------------------| | 1 | Day 0–1 | Mobilize day 1, weight bearing as tolerated for stable fixation (protected only if severe osteoporosis) | Neurovascular check, multimodal analgesia (minimize opioids), thromboprophylaxis, gait training | | 2 | Week 1–6 | Weight bearing as tolerated; progress frame/walker to crutches | Hip range of motion, quadriceps strengthening; wound check and staple removal at 2 weeks | | 3 | Week 6–12 | Increase weight bearing, wean aids | X-rays at 6 and 12 weeks — check for cut-out (progressive superior screw migration), callus and trabeculation across the fracture | | 4 | Month 3–6 | Full as tolerated | X-ray at 6 months to confirm union (bridging callus on 3 of 4 cortices, no pain with weight bearing) | Thromboprophylaxis is mandatory in this high-risk elderly population (a 40–60% deep-vein thrombosis rate without prophylaxis): mechanical prophylaxis (TED stockings, pneumatic compression) plus chemical prophylaxis (LMWH such as enoxaparin 40mg subcutaneously daily, or a NOAC per local protocol) for a minimum of 35 days or until fully mobile, balancing bleeding against thrombosis risk. Orthogeriatric co-management — a multidisciplinary team managing comorbidities, bone health (calcium, vitamin D, bisphosphonates or denosumab), nutrition, cognition, falls prevention and discharge planning — reduces mortality, complications and length of stay, and is the standard of care. Implant removal is NOT routine — only for symptomatic prominent hardware, anterior thigh pain from the nail, or patient request after confirmed union (minimum 12 months). Complications
- Recognition
- Hip pain, limb shortening, loss of fixation on X-ray; the screw migrates superiorly through the head, typically at 6–12 weeks and progressive on serial films
- Prevention
- TAD less than 25mm (critical), center-center or inferior-center position (never superior), screw depth 5–10mm from subchondral bone, avoid varus, restore medial support
- Management
- Symptomatic: revision to total hip arthroplasty or hemiarthroplasty; minimal displacement with healing progressing may be managed protected and monitored
- Recognition
- Leg-length discrepancy, external rotation deformity, varus on X-ray, altered gait and reduced function
- Prevention
- Adequate fracture-table reduction (accept valgus, not varus), restore medial cortical support, correct rotation, avoid over-distraction, check alignment before closure
- Management
- Mild and functional: accept and monitor; severe with functional impairment: corrective osteotomy or conversion to THA if symptomatic arthritis develops
- Recognition
- Persistent pain, inability to weight bear, no healing progression on serial X-rays at 6 months with sclerotic fracture edges
- Prevention
- Adequate reduction with medial support, an appropriate (long) nail for unstable patterns, avoid over-distraction, dynamic locking, early weight bearing
- Management
- Asymptomatic in the elderly: may accept; symptomatic: revision to THA or exchange nailing with bone graft, blade plate or revision cephalomedullary nail
- Recognition
- Wound drainage, erythema, fever, raised inflammatory markers; deep infection may present late with pain and loosening
- Prevention
- IV antibiotics within 60 minutes of incision, minimize operative time, percutaneous technique, aseptic technique, orthogeriatric optimization
- Management
- Superficial: antibiotics and local care; deep early (less than 3 weeks): irrigation and debridement with implant retention if stable and prolonged antibiotics; deep late: implant removal, debridement, arthroplasty or external fixator
- Recognition
- Intraoperative: sudden loss of resistance, change in alignment on fluoroscopy; postoperative: sudden pain with a fall, a new fracture line at the nail tip
- Prevention
- Gentle entry-portal technique, ream appropriately (not too aggressively), correct nail size, recognize osteoporotic bone, long nail for poor bone quality
- Management
- Intraoperative: extend to a long nail, cerclage if at the entry, ensure fixation spans the fracture; postoperative: revision to a longer nail, ORIF with a plate and cerclage, bone-health optimization
- Recognition
- Anterior thigh pain with hip flexion, a palpable prominence, pain on direct pressure, worse sitting; fluoroscopy shows the nail proud or anterior
- Prevention
- Correct entry point in line with the canal on lateral, nail flush or only slightly proud, ensure curvature matches the femoral bow
- Management
- Conservative: activity modification, NSAIDs, physiotherapy; persistent and symptomatic: removal after union (12+ months)
- Recognition
- Intraoperative: change in alignment on fluoroscopy, visible propagation; postoperative: loss of reduction and varus collapse on early X-rays
- Prevention
- Pre-operative lateral wall thickness assessment (less than 20mm — use a long nail or alternative), gentle technique, consider prophylactic cerclage in osteoporotic bone
- Management
- Intraoperative: cerclage fixation, convert to a long nail or change to a sliding hip screw with a trochanteric stabilization plate; postoperative: stable and healing — monitor; unstable — revision fixation
Z-effect and reverse Z-effect — migration of the cephalic screw within the nail (backing out laterally, or migrating medially) causing loss of fixation. Prevent with adequate screw engagement and compression with helical blade systems; revise if symptomatic. DVT/PE — high risk; incidence 40–60% without prophylaxis. Prevent with mechanical and chemical prophylaxis and early mobilization; treat with anticoagulation (an IVC filter if recurrent despite anticoagulation). Mortality — 30-day mortality 5–10%, 1-year mortality 20–30% in the elderly population. Reduce it with orthogeriatric co-management and early surgery (within 36–48 hours of admission).
Viva & Exam Focus
TAD PLUSTAD PLUS — the cephalic-screw check
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 78-year-old woman has an intertrochanteric hip fracture. Your registrar suggests a dynamic hip screw. Walk me through your decision-making for fixation choice, and specifically when you would use a cephalomedullary nail instead.”
“What is tip-apex distance, how do you measure it, and why is it the most important technical factor in cephalomedullary nailing?”
“Your registrar has inserted the nail but on final imaging the cephalic screw has a tip-apex distance of 30mm and sits in the superior third of the head on both views. What do you do, and why is this a problem?”
Indications
- Unstable intertrochanteric fractures (AO 31-A2.2, A2.3, A3), reverse obliquity, subtrochanteric extension, lateral wall less than 20mm
- For stable A1/A2.1 the DHS is an excellent, lower-complication option (Parker and Handoll Cochrane); a nail is acceptable but offers no clear advantage
- Long nail: subtrochanteric extension, lateral wall comminution, reverse obliquity, pathological fractures, ipsilateral neck-shaft fractures
- Short nail: isolated intertrochanteric with an intact lateral wall greater than 20mm, stable patterns, no distal extension
Key anatomy
- Entry point: greater trochanter tip (trochanteric entry) or piriformis fossa — confirm on AP AND lateral
- Superior gluteal neurovascular bundle 3–5cm proximal to the tip — keep the entry at or below the tip
- Femoral head blood supply: medial femoral circumflex retinacular vessels — minimize stripping, avoid multiple screw attempts
- Lateral wall: lateral cortex from trochanter to lesser trochanter — measure thickness perpendicular at the lesser-trochanter level, less than 20mm is unstable
Critical steps
- Reduction: fracture table, traction, internal rotation 10–15°; accept anatomic or valgus, restore medial support, no varus, no posterior sag
- Entry: at the tip on AP, aligned with the canal on LATERAL — too lateral means varus, too medial means valgus or medial perforation
- Cephalic screw: center-center or inferior-center on both views; TAD less than 25mm; deep, 5–10mm from subchondral bone
- Distal locking: short nail 1–2 static screws; long nail static (2 screws) for subtrochanteric or unstable, dynamic (1 screw) for pure intertrochanteric
- Final check: reduction, nail depth (flush or 5–10mm proud, not buried), TAD less than 25mm, no joint penetration, rotation and length versus the contralateral side
Structures at risk
- Superior gluteal neurovascular: keep the entry at or below the tip, no dissection more than 3cm above it
- Sciatic nerve: avoid posterior retractors, monitor function
- Medial femoral circumflex/head supply: minimize stripping, careful screw insertion
- Lateral femoral cutaneous nerve: percutaneous, small incision over the trochanter
- Abductors: split in line with fibers, do not split the trochanter, repair tears
Technique pearls
- TAD less than 25mm is the single most important technical factor (Baumgaertner 1995) — know how to calculate it: the sum of AP and lateral measurements
- The lateral view entry is as important as the AP — it must be in line with the canal centre to prevent malalignment
- Varus reduction is unacceptable — it increases cut-out exponentially; valgus (5–10°) is acceptable and medial support is critical
- Nail depth: flush or 5–10mm proud — never buried below the tip, which is extremely difficult to remove
- Superior screw position carries the highest cut-out risk (thin subchondral bone, high stress) — center-center or inferior-center is mandatory
Complications
- Cut-out (2–6%, most common mechanical failure): a TAD greater than 25mm is the main risk — prevent with TAD less than 25mm, central position, no varus, medial support
- Malunion (5–15%): varus, rotation, shortening — prevent with adequate reduction and checking rotation
- Non-union (1–2%, higher with lateral wall comminution): prevent with medial support, an appropriate nail and dynamic locking
- Infection (1–3% deep): IV antibiotics within 60 minutes, percutaneous technique
- Shaft fracture (0.5–1% intraoperative, 1–3% postoperative) at the nail tip: gentle technique, correct reaming and nail size
- Mortality: 30-day 5–10%, 1-year 20–30% — improve with orthogeriatric co-management and surgery within 48 hours
Post-op protocol
- Thromboprophylaxis: LMWH or a NOAC for at least 35 days (40–60% DVT without prophylaxis)
- Weight bearing as tolerated immediately for stable fixation
- Mobilize day 1 with physiotherapy; aim for independent mobility by 6 weeks
- Follow-up X-rays at 6 weeks, 12 weeks and 6 months — monitor for cut-out
- Orthogeriatric co-management reduces mortality and complications
Exam tips
- Opening statement: a CMN is first-line for unstable intertrochanteric fractures; critical factors are lateral wall less than 20mm, TAD less than 25mm, center-center or inferior-center position, medial support, and varus unacceptable
- Buzz words: 'tip-apex distance less than 25mm', 'center-center or inferior-center', 'lateral wall thickness', 'medial cortical support', 'valgus acceptable, varus is not'
- Know the evidence: Baumgaertner TAD less than 25mm (1995), Parker and Handoll Cochrane (2010), lateral wall less than 20mm (Hsu 2013, Palm 2007)
- Common mistakes: accepting varus, not checking the lateral view for entry, not knowing the TAD threshold, burying the nail below the tip
- Viva strategy: classify with AO, assess the lateral wall, state reduction goals, describe the TAD calculation, then the final-check protocol
Background & Evidence
Epidemiology. Intertrochanteric (peritrochanteric) fractures are among the most common fragility fractures of the proximal femur, occurring predominantly in the elderly osteoporotic population with a strong female predominance and a peak in the eighth decade and beyond. They are a major cause of morbidity and mortality — national hip-fracture registries consistently report a 30-day mortality of roughly 7–10% and a 1-year mortality of roughly 20–30% — which is why early surgery (within 36–48 hours) and orthogeriatric co-management are repeatedly associated with better survival across registries. Classification (AO/OTA 31-A). The AO/OTA classification of peritrochanteric fractures drives implant choice through the integrity of the medial and lateral walls.
- Pattern
- Simple, two-part intertrochanteric fracture with an intact medial cortex
- Stability
- Stable
- Typical implant
- Sliding hip screw or a short nail
- Pattern
- Multi-fragmentary intertrochanteric fracture with posteromedial (lesser-trochanter) comminution
- Stability
- Unstable (worsens with A2.2, A2.3)
- Typical implant
- Cephalomedullary nail — long if the lateral wall is deficient
- Pattern
- Reverse obliquity — the medial cortex is proximal to the fracture line
- Stability
- Unstable
- Typical implant
- Long cephalomedullary nail (a DHS will fail)
Guidelines, registries and global practice. Named-society guidance converges on a pattern-based approach in which lateral-wall integrity, not just the AO subtype, drives implant choice:
- Stable trochanteric (A1/A2)
- Extramedullary device (SHS) preferred for trochanteric fractures above and outside the lesser trochanter
- Subtrochanteric / reverse obliquity / unstable
- Intramedullary nail for subtrochanteric fractures
- Care model
- Operate on the day of or after admission; orthogeriatric co-management; mobilize day 1
- Stable trochanteric (A1/A2)
- SHS acceptable for stable patterns
- Subtrochanteric / reverse obliquity / unstable
- Cephalomedullary nailing for unstable, reverse-obliquity and subtrochanteric patterns
- Care model
- Early surgery and multidisciplinary care
- Stable trochanteric (A1/A2)
- Stable A1 amenable to SHS or a short nail
- Subtrochanteric / reverse obliquity / unstable
- A3, reverse obliquity and subtrochanteric extension require a long cephalomedullary nail
- Care model
- Lateral-wall integrity, not just subtype, drives choice
References
The value of the tip-apex distance in predicting failure of fixation of peritrochanteric fractures of the hip
- 198 peritrochanteric fractures; 16 of 19 failures were lag-screw cut-out through the femoral head
- TAD is the SUM of the screw-tip-to-apex distance on AP and lateral views, corrected for magnification
- Mean TAD 24mm in healed fractures versus 38mm in cut-outs (p=0.0001)
- NONE of the 120 screws with a TAD of 25mm or less cut out; cut-out rate rose steeply with increasing TAD regardless of other variables
Gamma and other cephalocondylic intramedullary nails versus extramedullary implants for extracapsular hip fractures in adults
- 43 randomised/quasi-randomised trials; 22 trials (3749 patients) compared the Gamma nail with the sliding hip screw (SHS)
- The Gamma nail was associated with increased operative and later femoral fracture and a higher reoperation rate for trochanteric fractures
- For stable trochanteric fractures the SHS appeared superior given its lower complication rate
- Intramedullary nails showed advantages over fixed-angle plates for subtrochanteric and some unstable trochanteric fractures
Integrity of the lateral femoral wall in intertrochanteric hip fractures: an important predictor of a reoperation
- 214 intertrochanteric fractures fixed with a 135-degree sliding compression hip screw
- Reoperation in 3% with an intact lateral wall versus 22% when the lateral wall was fractured (p less than 0.001)
- 74% of lateral-wall fractures occurred intra-operatively; lateral-wall fracture was the main independent predictor of reoperation
- Lateral-wall fracture occurred in 31% of AO/OTA 31-A2.2 and A2.3 patterns versus 3% of A1/A2.1 patterns
Lateral femoral wall thickness: a reliable predictor of post-operative lateral wall fracture in intertrochanteric fractures
- 208 AO/OTA 31-A1 and A2 fractures fixed with a dynamic hip screw
- Lateral wall thickness and fracture classification were independent predictors of post-operative lateral-wall fracture (both p less than 0.001)
- The threshold lateral-wall thickness for secondary fracture was 20.5mm
- The authors concluded fractures with a lateral wall under 20.5mm should NOT be treated with a DHS alone
Hip fracture: management (NICE Clinical Guideline CG124)
- Use extramedullary implants such as the sliding hip screw in preference to an intramedullary nail for trochanteric fractures ABOVE and OUTSIDE the lesser trochanter (AO/OTA A1 and A2)
- Use an intramedullary nail for subtrochanteric fractures
- Operate on the day of, or the day after, admission and offer orthogeriatric multidisciplinary co-management
- Mobilise patients and offer physiotherapy from the day after surgery
Mechanics of the treatment of hip injuries
- Classic biomechanical analysis of the factors governing stability of hip-fracture fixation
- Defines the four variables that control fragment stability: bone quality, fragment geometry, implant design and implant placement
- Underpins why reduction and implant position dominate outcome in peritrochanteric fractures
Management of Hip Fractures in Older Adults: Evidence-Based Clinical Practice Guideline
- Cephalomedullary nailing recommended for unstable, reverse-obliquity and subtrochanteric patterns
- Strong support for early surgical intervention and multidisciplinary care in older adults
- Pattern-based implant selection aligned with lateral-wall integrity