Posterior midline approach to the lumbosacral thecal sac, single-level L1 laminectomy · advanced
- Indicated for SPASTIC diplegia cerebral palsy (GMFCS II-III), age 3-8 years, where spasticity predominates over weakness. SDR is NOT for dystonia, athetosis or severe weakness.
- Intraoperative EMG is essential. Abnormal rootlets show sustained, spreading, bilateral responses (Grade 3-4) and are divided; normal rootlets (Grade 0-1) are preserved for sensation.
- Divide 30-50 percent of dorsal rootlets per level from L2 to S2. S1 is treated most aggressively (40-60 percent) because gastrocnemius spasticity drives equinus; L3 is most conservative (25-40 percent) to avoid quadriceps weakness and crouch.
- Distinguish dorsal roots (POSTERIOR, thinner, sensory — the target) from ventral roots (ANTERIOR, thicker, motor — never divide). Ventral root injury causes permanent weakness.
- A modern single-level L1 laminectomy exposes the entire cauda equina while reducing the kyphosis risk to 10-15 percent versus 20-25 percent with a traditional multi-level laminectomy.
When & Why
Indication. Selective dorsal rhizotomy is indicated for spastic diplegia cerebral palsy (bilateral lower-limb spasticity) in ambulatory children (GMFCS level II-III), typically aged 3-8 years, in whom spasticity predominates over weakness (Modified Ashworth Scale 2 or more) and conservative management has failed. The procedure interrupts the sensory limb of the exaggerated stretch reflex by dividing a proportion of the lumbosacral dorsal rootlets, permanently reducing spasticity while preserving useful motor control and sensation. The right child. Beyond the diagnosis, the candidate must have: - Predominant spasticity over weakness, with good selective motor control and dynamic spasticity that improves with nerve blocks or sleep.
- Adequate trunk control and upper-limb function, and a motivated child and family able to commit to intensive post-operative rehabilitation.
- No fixed contractures requiring extensive orthopaedic surgery first (small, flexible contractures may be addressed later). Failed conservative management must be documented — intensive physiotherapy (at least 12 months), appropriate orthoses (AFOs or KAFOs), multiple cycles of botulinum toxin, and oral anti-spasmodics (baclofen, diazepam).
Spastic diplegia, GMFCS II-III, age 3-8, Ashworth 2 or more, good selective motor control, motivated family, and failed conservative care.
Carefully selected spastic quadriplegia with good upper-limb function; older children (8-12 years) with preserved motor control; combined SDR with orthopaedic procedures for mild contractures.
Dystonia or athetosis (will not improve and may worsen), severe weakness predominating over spasticity, fixed contractures needing orthopaedic surgery first, poor trunk control (GMFCS IV-V), severe spinal deformity, or cognitive impairment preventing rehabilitation.
Pre-operative assessment. Confirm the movement disorder is spasticity, not dystonia. Document the GMFCS level and selective motor control, grade spasticity (Modified Ashworth) and strength (MRC), and assess range of motion. Perform 3D gait analysis to quantify the spasticity distribution and overactive muscle groups — it directly guides the level-by-level intra-operative plan. Image the spine with MRI to exclude a tethered cord, syrinx or Chiari malformation, and obtain hip radiographs to assess the migration percentage. Consent specifically for transient sensory change or dysesthesia (5-10 percent), CSF leak or pseudomeningocele (5-8 percent), post-laminectomy spinal deformity (10-15 percent kyphosis), a small risk of new motor weakness from ventral root injury (less than 2 percent), temporary bladder dysfunction, and the need for prolonged intensive physiotherapy and possible later orthopaedic surgery. Set realistic expectations: SDR reduces spasticity durably but does not cure cerebral palsy, does not prevent fixed contractures, and the added gross-motor benefit over high-quality physiotherapy alone is modest. Setup. Prone on a radiolucent Jackson table with the abdomen hanging free and the hips flexed 30-45 degrees (table break) to open the interspinous spaces and reduce epidural venous engorgement. Comprehensive neuromonitoring — SSEPs, MEPs and multi-channel EMG — is essential, and baselines are recorded before draping.
The Operation
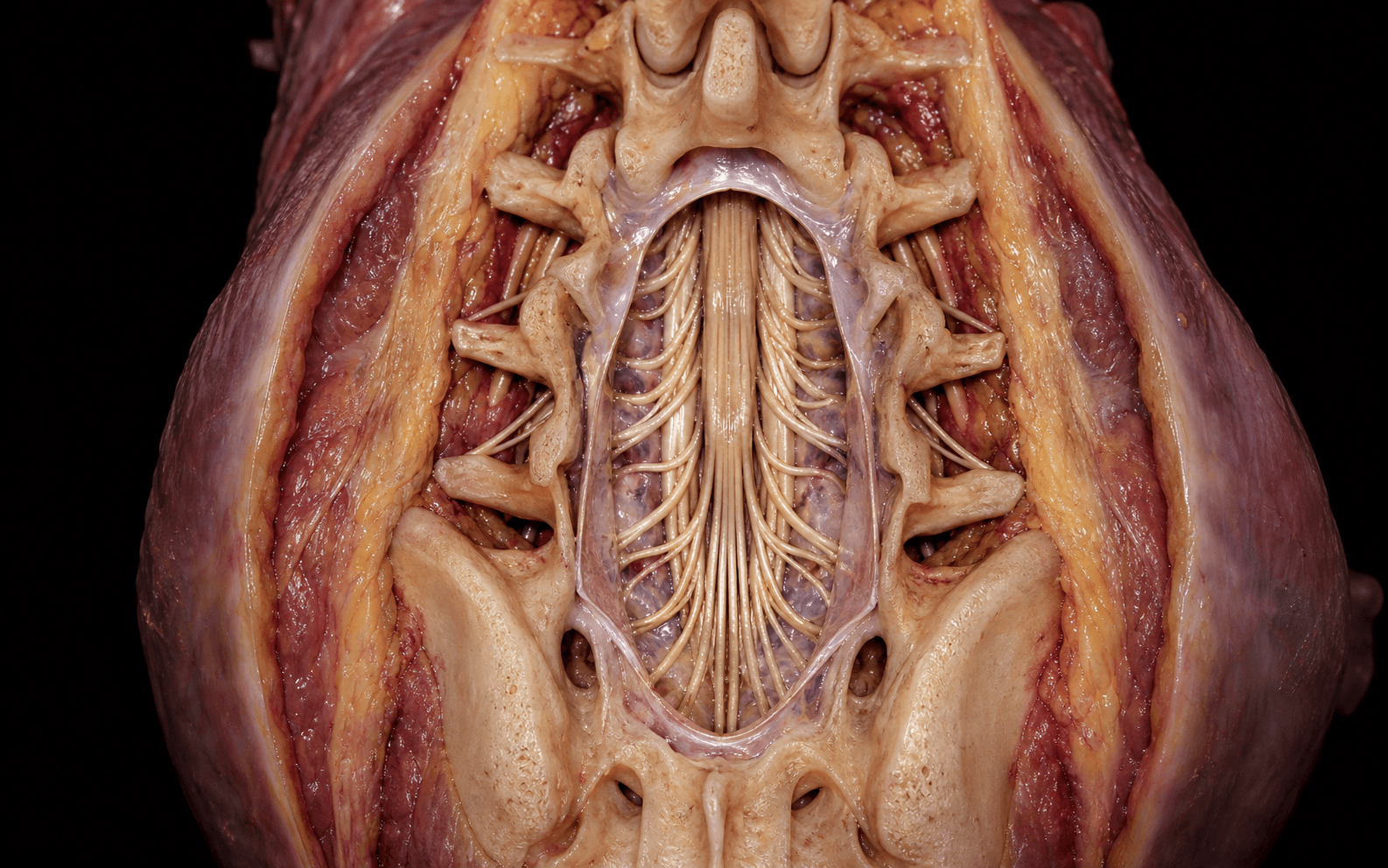
The goal is to expose the lumbosacral thecal sac through a posterior midline approach, open the dura in strict midline, identify each dorsal root from L2 to S2 and separate it into rootlets, then use intra-operative EMG to select and divide the abnormal (spasticity-generating) rootlets while preserving motor function and sensation. The exposure — positioning, incision, muscle elevation, the bone-sparing single-level L1 laminectomy and the dural opening — is laid out in full as the first steps below, because safe access to the cauda equina is the foundation of the whole operation.
Operative sequence
- Prone on a radiolucent Jackson table, abdomen hanging free to reduce epidural venous engorgement.
- Hips flexed 30-45 degrees (table break) to open the interspinous spaces — critical for an easier laminectomy.
- Arms abducted and padded; head neutral on a horseshoe or Mayfield; all pressure points protected.
- Neuromonitoring: SSEPs (posterior tibial nerve), MEPs (transcranial), and EMG electrodes in hip adductors (L2-3), quadriceps (L3-4), tibialis anterior (L4-5), extensor hallucis longus (L5), gastrocnemius (S1), hamstrings (L5-S1) and anal sphincter (S2-4). Baselines recorded before draping.
- Midline posterior incision from L1 to S1 (12-15 cm), confirmed against the spinous processes and fluoroscopy.
- Incise the thoracolumbar fascia in the strict midline (avascular) plane and elevate the paraspinal muscles subperiosteally off the spinous processes and laminae, out to the facet joints — preserving the joint capsules to protect stability.
- Meticulous bipolar haemostasis; bone wax on exposed cancellous edges. Strict midline avoids entering the canal prematurely.
- The modern approach removes the L1 lamina and the cranial third of L2, exposing the entire cauda equina in the thecal sac at this single level — every lumbosacral root is reachable through one window.
- This minimises bone removal, lowering the kyphosis risk to 10-15 percent versus 20-25 percent for a traditional multi-level laminectomy.
- Use a Leksell rongeur or high-speed drill with a footplate. Remove the ligamentum flavum with a Kerrison rongeur from the superior edge downward, taking care not to plunge into the epidural space.
- Control engorged epidural veins with bipolar cautery and irrigation, and haemostatic agents (Gelfoam, Floseal).
- Confirm the conus level (intra-operative ultrasound or fluoroscopy) before opening — the conus usually ends at L1-L2 but may extend to L3 in young children.
- Pick up the dura in the strict midline (the avascular raphe), confirm CSF pulsation, and create a 2-3 mm opening with a 15-blade, extending cranially and caudally with microscissors to give an 8-12 cm window (L1 to S1).
- Place 4-0 or 5-0 silk tacking sutures to the dural edges and secure them to the drapes to hold the sac open. Move to the operating microscope for all intradural work and maintain a CSF pool with warm saline irrigation.
- Identify the conus and filum terminale, then follow each root from conus to exit foramen, counting L2, L3, L4, L5, S1, S2 using anatomical landmarks and fluoroscopy.
- The critical skill: separate the dorsal root (POSTERIOR in the sac, THINNER, 1-2 mm, sensory) from the ventral root (ANTERIOR, THICKER, 2-3 mm, motor). The two merge 5-15 mm lateral to the midline; the dorsal root ganglion is palpable just proximal to the merger. Never divide a ventral root.
- Under the microscope, separate each dorsal root into 3-5 individual rootlets using fine forceps and microscissors, placing a coloured background for contrast.
- Place a hook electrode under each individual rootlet and stimulate at 50 Hz (tetanic), starting at 0.5 mA up to a 2 mA maximum.
- Grade the response 0-4: Grade 0 no response; Grade 1 a brief, localised, fatiguing twitch (normal); Grade 2 a sustained single-muscle contraction (borderline); Grade 3 sustained contraction spreading to multiple muscles (abnormal); Grade 4 sustained bilateral response recruiting distant muscles (most abnormal).
- Divide the Grade 3-4 rootlets preferentially, targeting 30-50 percent of rootlets per level; preserve enough Grade 0-1 rootlets to retain sensation. (The full grading table and per-level targets are in Background & Evidence.)
- Work systematically from L2 to S2, dividing 30-50 percent of the abnormal rootlets at each level guided by the pre-operative gait analysis and the EMG.
- S1 — most aggressive (40-60 percent). Gastrocnemius-soleus spasticity is the primary driver of equinus (toe-walking) in diplegic CP; under-treating S1 is the commonest cause of inadequate improvement. Divide 2-3 of the 4-5 rootlets.
- L3 — most conservative (25-40 percent). Over-division weakens the quadriceps and worsens crouch gait — the commonest technical error. Divide only 1-2 rootlets.
- L2 (adductors, scissoring): 30-40 percent. L4 (quadriceps and tibialis anterior): 30-50 percent balanced. L5 (EHL, peroneals, hamstrings): 30-50 percent by gait analysis. S2 (intrinsic foot): 30-40 percent, conservative.
- Irrigate the thecal sac thoroughly; gently coagulate any bleeding rootlet stumps on low bipolar power, avoiding intact roots.
- Remove the tacking sutures and close the dura with a running 4-0 or 5-0 braided non-absorbable suture (Tevdek or Ethibond), small 1-2 mm bites, watertight.
- Leak test: ask the anaesthetist to perform a Valsalva to 30-40 cm water; reinforce any leak with interrupted sutures and overlay a dural sealant (DuraSeal, Tisseel).
- Re-approximate the paraspinal muscles and close the thoracolumbar fascia robustly with heavy absorbable suture (0 or 1 PDS or Vicryl) to withstand CSF pressure, then layered closure (2-0 Vicryl to Scarpa layer, 3-0 or 4-0 subcuticular Monocryl, skin adhesive). A drain is generally avoided.
- Examine the child awake: tone should be dramatically reduced; motor power preserved or better (reduced co-contraction); sensation intact (some dysesthesia acceptable). Any new focal weakness suggests ventral root injury.
The whole operation turns on correctly separating the dorsal (sensory) from the ventral (motor) roots. Dorsal roots are POSTERIOR and THINNER; ventral roots are ANTERIOR and THICKER. Use anatomical position, the palpable root morphology and EMG confirmation together before any division. Dividing a ventral root causes permanent weakness in its muscle territory and should occur in fewer than 2 percent of cases.
The single-level L1 laminectomy exposes the entire cauda equina in the thecal sac at one window — all lumbosacral roots are accessible here — while removing far less bone than a classic L1-S1 multi-level laminectomy. That is why the modern technique cuts the kyphosis risk from 20-25 percent down to 10-15 percent.
S1 is treated most aggressively (40-60 percent division) because gastrocnemius spasticity is the primary driver of equinus — under-treatment here is the commonest cause of a poor outcome. L3 is treated most conservatively (25-40 percent) because over-division weakens the quadriceps and worsens crouch — the commonest technical error.
Aftercare & Complications
Rehabilitation — the operation creates a window of opportunity by removing spasticity; intensive therapy is what converts that into functional gain. | Phase | Timing | Focus | |-------|--------|-------| | 1 | 0-2 days | ICU or HDU, neuro observations every 2 hours, flat bed rest 24-48 hours, Foley catheter, multimodal analgesia | | 2 | Day 2-5 | Sit, stand and begin gentle range of motion; early mobilisation capitalises on the tone reduction; AFO review | | 3 | Week 1 to month 6 | Intensive physiotherapy 3-5 sessions per week: quadriceps and dorsiflexor strengthening, balance and proprioception, gait re-education | | 4 | Month 6 to year 2 | Repeat 3D gait analysis at 3 and 6 months; orthopaedic review for residual fixed contractures; annual spine radiographs | Bladder retention is common and usually temporary; a persistent deficit beyond 48 hours warrants evaluation for a cauda equina problem. Most children return to their pre-operative mobility level within weeks, with durable tone reduction and gradual functional gains over the first 1-3 years. Complications
- Recognition
- Clear glucose-positive fluid from the wound, fluctuant collection, upright headache
- Prevention
- Watertight 4-0 continuous dural closure, Valsalva test, sealant, robust fascial closure, flat bed rest 24-48 hours
- Management
- Conservative first: flat rest, pressure dressing, acetazolamide. Persistent leak over 7 days: surgical re-closure. Asymptomatic pseudomeningocele: observe
- Recognition
- Progressive thoracolumbar roundback and back pain on serial radiographs over 2-5 years
- Prevention
- Single-level L1 laminectomy, preserve facet joints and paraspinal attachments
- Management
- Under 40 degrees: observe, core strengthening, brace. Over 40-50 degrees or symptomatic: posterior spinal fusion
- Recognition
- Altered lower-limb sensation, burning or tingling, proprioceptive loss with gait instability
- Prevention
- Limit division to 30-50 percent per level, preserve Grade 0-1 rootlets, avoid over 60 percent
- Management
- Usually transient, resolves in 4-12 weeks; gabapentin or amitriptyline if severe; balance training and AFO if persistent
- Recognition
- New weakness in a root distribution (quadriceps, dorsiflexors, plantarflexors), foot drop
- Prevention
- Meticulous dorsal versus ventral identification, EMG confirmation, microsurgical no-traction technique
- Management
- Physiotherapy strengthening, AFO for foot drop, tendon transfer if permanent after 12 months
- Recognition
- Temporary retention in first 48 hours; ongoing retention or incontinence beyond 1 week if permanent
- Prevention
- Only divide dorsal roots (sphincter function is ventral and parasympathetic), gentle sacral technique, avoid excess cautery
- Management
- Temporary: Foley, trial of voiding at 48 hours. Permanent: urology referral, intermittent catheterisation, bowel regimen
- Recognition
- Persistent spasticity, often gastrocnemius if S1 under-treated, Ashworth improvement under 2 points
- Prevention
- Adequate division per level (30-50 percent, S1 40-60 percent), systematic EMG, divide Grade 3-4
- Management
- Physiotherapy, optimise orthoses, botulinum toxin; revision SDR (high risk) or intrathecal baclofen if refractory
- Recognition
- Calcaneus: excessive dorsiflexion, heel-only weight bearing. Crouch: excessive stance knee flexion
- Prevention
- Balanced division, conservative L3 (25-40 percent), S1 not over 60 percent, pre-operative gait analysis
- Management
- Calcaneus: AFO with plantarflexion stop, FDL or FHL transfer. Crouch: quadriceps strengthening, extension osteotomy or patellar tendon advancement
Viva & Exam Focus
SPASTICSPASTIC — is this child a candidate?
BRIEFBRIEF — the EMG response grades
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 5-year-old with spastic diplegic cerebral palsy is referred for consideration of SDR. Walk me through your assessment and selection criteria.”
“Intra-operatively you stimulate a rootlet and get a sustained bilateral response in both gastrocnemius muscles lasting 5 seconds. What is your interpretation and management?”
“Six months after SDR in a 6-year-old the tone reduction is excellent, but the parents report progressive roundback deformity and back pain. What is your concern and your management?”
Indication
- Spastic diplegia CP, GMFCS II-III, age 3-8, spasticity over weakness
- Failed physio, orthoses and botulinum toxin over 12 months
- NOT for dystonia, athetosis, severe weakness, fixed contractures or poor trunk control
Anatomy at risk
- Conus ends L1-L2 (L3 in children) — identify before laminectomy
- Dorsal roots: posterior, thinner, sensory — the target
- Ventral roots: anterior, thicker, motor — never divide
- Artery of Adamkiewicz enters T9-L2, usually left — feeds the lumbar cord
Critical steps
- Prone, hips flexed 30-45 degrees, abdomen free, full neuromonitoring
- Single-level L1 laminectomy exposes the whole cauda equina (kyphosis 10-15 percent)
- Midline dural opening, tacking sutures, microscope
- EMG each rootlet at 50 Hz, grade 0-4, divide Grade 3-4
- Divide 30-50 percent per level; watertight closure with Valsalva test
Level-specific
- S1 most aggressive 40-60 percent — gastrocnemius drives equinus
- L3 most conservative 25-40 percent — over-division causes crouch
- L2 30-40 percent, L4 30-50 percent, L5 30-50 percent, S2 30-40 percent
Aftercare
- Flat bed rest 24-48 hours, early mobilisation day 2-3
- Intensive physio 3-5 sessions per week for 6-12 months
- Repeat gait analysis at 3 and 6 months
- Annual spine radiographs for 5 years; orthopaedic surgery for residual contractures
Complications
- CSF leak and pseudomeningocele 5-8 percent
- Post-laminectomy kyphosis 10-15 percent
- Sensory change and dysesthesia 5-10 percent
- Ventral root motor injury less than 2 percent
- Bladder dysfunction temporary 5 percent, permanent less than 1 percent
Background & Evidence
Rationale and history. Spasticity is velocity-dependent increased tone driven by an exaggerated stretch reflex. SDR reduces it by dividing a proportion of the lumbosacral dorsal (sensory) rootlets, interrupting the sensory afferent limb of that reflex at the spinal cord while sparing the motor (ventral) roots. The technique was developed by Fasano and refined by Peacock and Arens (Cape Town, 1982), then evolved into the modern bone-sparing single-level conus laminectomy described by Park and Johnston. The spinal cord and cauda equina. The conus medullaris terminates at L1-L2 in adults but may extend to L3 in young children (and to L3-L4 in neonates) — its level must be confirmed before laminectomy so the bone window sits at or below the conus. Below the conus, the L1-S5 nerve roots descend within the thecal sac as the cauda equina, becoming progressively more oblique (the L2 root runs at about 30 degrees, the S1 root at about 60 degrees to the horizontal). Each dorsal root divides into 3-7 rootlets (average 4-5), which are the units tested and divided. Blood supply. A single midline anterior spinal artery supplies the anterior two-thirds of the cord (including the motor tracts) and is fed by 6-10 radicular arteries along its length, including the dominant artery of Adamkiewicz (entering T9-L2, usually on the left) which supplies the lumbar enlargement — its injury causes anterior cord syndrome. Paired posterior spinal arteries supply the posterior third. Radicular arteries accompany the roots through the foramina and can bleed during rootlet division, usually controlled with bipolar cautery.
- Response pattern
- No response
- Interpretation
- Normal
- Action
- Preserve
- Response pattern
- Brief twitch in the appropriate muscle, unilateral, fatigues rapidly
- Interpretation
- Normal
- Action
- Preserve
- Response pattern
- Sustained contraction in a single muscle territory
- Interpretation
- Borderline
- Action
- May divide to reach target
- Response pattern
- Sustained contraction spreading to multiple muscles
- Interpretation
- Abnormal
- Action
- Divide
- Response pattern
- Sustained bilateral response recruiting distant muscles
- Interpretation
- Most abnormal
- Action
- Divide
- Key muscles
- Hip flexors, adductors
- Clinical driver
- Scissoring gait from adductor spasticity
- Division target
- 30-40%
- Key muscles
- Quadriceps, adductors
- Clinical driver
- Stiff-knee gait (over-division worsens crouch)
- Division target
- 25-40% (most conservative)
- Key muscles
- Quadriceps, tibialis anterior
- Clinical driver
- Knee and ankle spasticity, preserve dorsiflexion
- Division target
- 30-50% (balanced)
- Key muscles
- EHL, peroneals, gluteus medius, hamstrings
- Clinical driver
- Hamstring tightness, gait instability
- Division target
- 30-50% (gait-guided)
- Key muscles
- Gastrocnemius-soleus, hamstrings, gluteus maximus
- Clinical driver
- Equinus (toe-walking) — primary driver in diplegia
- Division target
- 40-60% (most aggressive)
- Key muscles
- Intrinsic foot, minor hamstring
- Clinical driver
- Foot posturing
- Division target
- 30-40% (conservative)
Anatomy at risk
Ends at L1-L2 but can extend to L3 in children. Identify with ultrasound or fluoroscopy before laminectomy and keep the bone window at or below the conus. Injury causes bladder, bowel and lower-limb dysfunction.
Dorsal (sensory) roots are posterior and thinner (1-2 mm) — the target. Ventral (motor) roots are anterior and thicker (2-3 mm) — never divide. EMG and morphology confirm each root before division.
The anterior spinal artery lies in the anterior median sulcus supplying the motor tracts; the artery of Adamkiewicz (T9-L2, usually left) is its dominant lumbar feeder. Stay posterior, avoid ventral dissection and excess cautery near radicular vessels.
Key evidence. The highest-level evidence is the individual-patient meta-analysis of the three published RCTs (McLaughlin, 2002, PMID 11811645): SDR plus physiotherapy reduced spasticity significantly more than physiotherapy alone, with a small but real additive gross-motor benefit (about 4 GMFM points) and a dose-response between the percentage of root tissue transected and functional gain. Wright (1998, PMID 9593495) showed that spasticity reduction translates into measurable gait improvement at one year. Selection remains the single most important determinant of outcome and is non-standardised worldwide (Grunt, 2014, PMID 24106928). Long-term, the tone reduction is durable for decades but gross motor function peaks around 3 years then gradually declines, and SDR does not prevent contractures (Tedroff, 2015, PMID 25523506). Spinal deformity after modern single-level SDR is driven mainly by baseline patient factors rather than the laminectomy itself (Ravindra, 2017, PMID 28885083).
References
Selective dorsal rhizotomy: meta-analysis of three randomized controlled trials
- Individual-patient meta-analysis pooling the three published RCTs of SDR plus physiotherapy versus physiotherapy alone in spastic diplegia (n=90; 82 children under 8 years, 65 at GMFCS II-III)
- SDR plus physiotherapy reduced spasticity significantly more than physiotherapy alone (pooled Ashworth mean change difference -1.2, p less than 0.001)
- Gross motor function (GMFM) improvement was greater with SDR but the effect was small (difference in change score +4.0 points, p=0.008)
- A direct dose-response relationship was found between the percentage of dorsal root tissue transected and functional improvement
Evaluation of selective dorsal rhizotomy for the reduction of spasticity in cerebral palsy: a randomized controlled trial
- Single-centre RCT of 24 children (mean age 58 months) with mild-to-moderate spastic diplegia randomised to SDR plus therapy versus therapy alone
- GMFM improved 12.1 percentage points in the SDR group versus 4.4 points in controls at 1 year (p less than 0.02)
- Knee and ankle tone were significantly reduced (p less than 0.005) with increased passive ankle dorsiflexion range (p less than 0.001) and reduced soleus stretch-reflex EMG activity (p less than 0.008)
- Foot-floor contact pattern during gait improved relative to controls (p less than 0.05)
Selection criteria for selective dorsal rhizotomy in children with spastic cerebral palsy: a systematic review of the literature
- Systematic review of 52 studies mapping reported SDR selection criteria across ICF domains
- Spasticity was documented in 94% of studies, other movement abnormalities (eg dystonia) in 62% and strength in 54% as selection variables
- Age (44%), diagnosis (50%) and gross motor function (27%) were inconsistently applied, and most criteria were not based on standardised measurements
- Authors call for international consensus guidelines because selection criteria vary considerably between centres
Risk factors for progressive neuromuscular scoliosis requiring posterior spinal fusion after selective dorsal rhizotomy
- Retrospective cohort of 134 children undergoing SDR via limited laminectomy (82% single-level), mean 53% of L1-S1 rootlets sectioned, mean follow-up 65 months
- 15 patients (11.2%) subsequently required posterior spinal fusion for progressive deformity
- Pre-operative non-ambulatory status (p less than 0.001) and a pre-operative Cobb angle over 30 degrees (p=0.003) were the significant risk factors on univariate analysis
- These are well-recognised deformity risk factors in spastic CP generally; SDR via limited laminectomy did not appear to significantly accelerate neuromuscular scoliosis
A prospective cohort study investigating gross motor function, pain, and health-related quality of life 17 years after selective dorsal rhizotomy in cerebral palsy
- Prospective cohort of 18 children with bilateral spastic CP followed a median of 17 years (15-20 years) after SDR
- The reduction in lower-limb muscle tone was sustained at long-term follow-up
- Peak gross motor function (GMFM) occurred at 3 years, followed by a gradual decline; SDR did not improve long-term function or prevent contractures
- Half of the cohort reported low-intensity pain; the durable tone reduction may help reduce CP-related pain over the long term
Surgical techniques of selective dorsal rhizotomy for spastic cerebral palsy (technical note)
- Describes the single-level laminectomy SDR performed at the level of the conus, exposing all dorsal roots without an L1-S1 multi-level laminectomy
- Single-level exposure reduces operating time, postoperative pain and the risk of progressive lumbar instability compared with the classic multi-level approach
- Reports only one CSF leak requiring operative repair in more than 1500 patients treated since 1991
- Confirms intraoperative electrophysiological rootlet testing as integral to the modern technique
Selective posterior rhizotomy for the relief of spasticity in cerebral palsy
- Landmark paper establishing the modern selective posterior rhizotomy technique and the patient selection criteria later adopted worldwide
A prospective gait analysis study in patients with diplegic cerebral palsy 20 years after selective dorsal rhizotomy
- 20-year follow-up gait analysis demonstrating maintained improvements in spasticity and function after SDR
Long-term outcome after selective dorsal rhizotomy in children with spastic cerebral palsy
- Multi-centre study of long-term outcomes including complications such as kyphosis and sensory changes
Changes in hip spasticity and strength following selective dorsal rhizotomy and physical therapy for spastic cerebral palsy
- Examines the relationship between spasticity reduction and strength gains after SDR
Selective dorsal rhizotomies in the treatment of spasticity related to cerebral palsy
- Comprehensive review of SDR indications, techniques and outcomes with emphasis on neurophysiological monitoring
Long-term functional benefits of selective dorsal rhizotomy for spastic cerebral palsy
- Long-term functional outcome study demonstrating GMFCS improvements and quality-of-life benefits