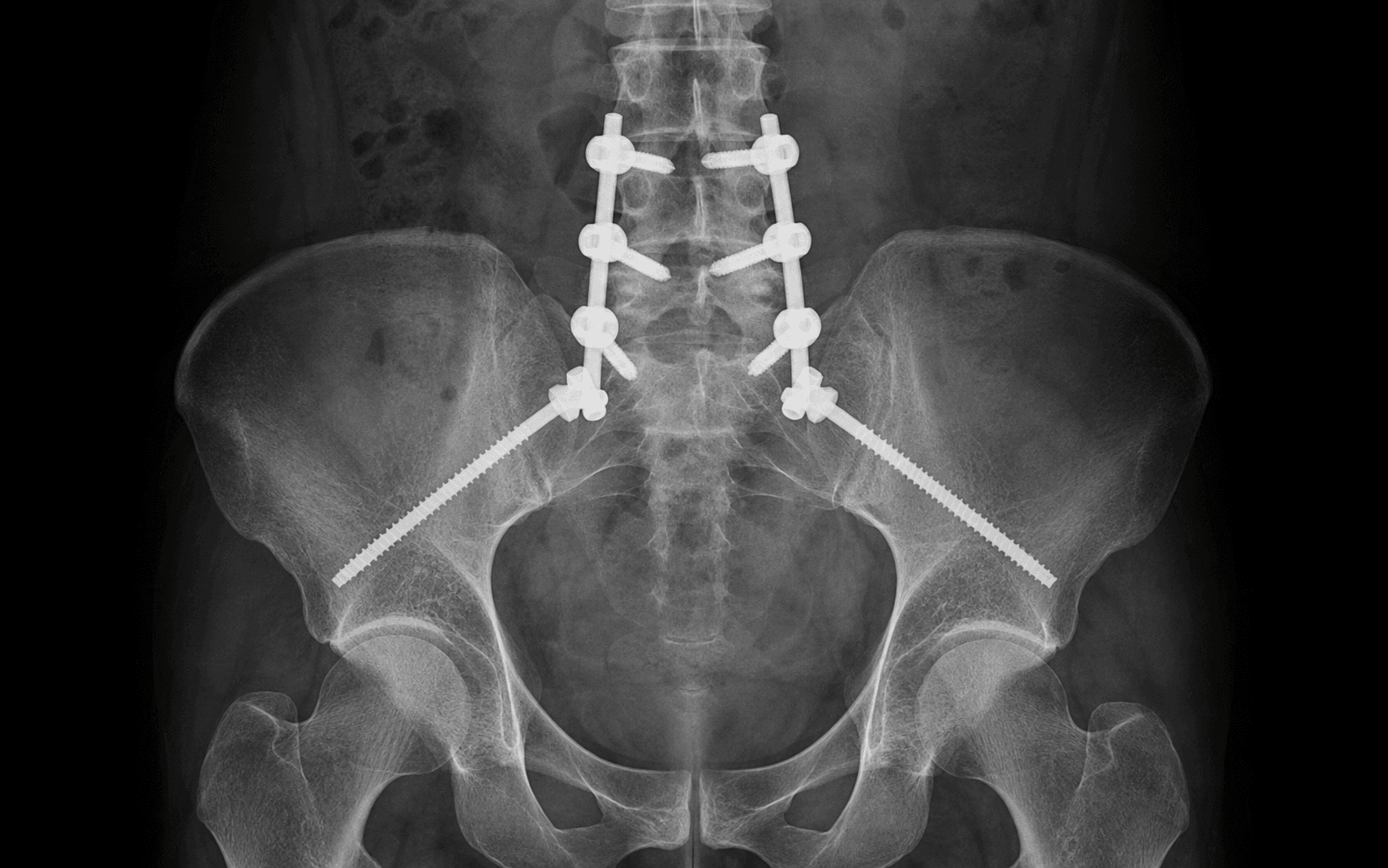
Posterior lumbopelvic fixation linking lumbar pedicle screws to iliac or S2-alar-iliac anchors for unstable U- and H-type sacral fractures
- Spinopelvic dissociation is bilateral vertical sacral fractures (often with a transverse component) that separate the spine from the pelvis — it is a longitudinal instability that needs lumbopelvic fixation, not isolated pelvic-ring fixation.
- Denis Zone III (central canal) sacral fractures carry roughly a 57 percent neurological injury rate and most often need decompression; Zone II about 28 percent; Zone I about 6 percent.
- Roy-Camille Type III transverse fractures are the comminuted pattern that produces spinopelvic dissociation.
- S2-alar-iliac (S2AI) screws give 30–40 percent greater pullout strength than traditional PSIS iliac screws, sit in line with the S1 pedicle for easy rod connection, and have far lower hardware prominence (about 5 percent versus 25 percent).
- Vertical shear injuries require lumbopelvic fixation that spans the injury, not isolated pelvic ring fixation.
- Cross-connectors are essential for rotational stability in bilateral constructs — they raise torsional rigidity by about 45 percent.
When & Why
The problem. Spinopelvic dissociation is a high-energy injury in which bilateral vertical sacral fractures (frequently joined by a transverse component through the sacral foramina, the U- or H-type pattern) disconnect the axial spine from the pelvic ring. The spine is then free to migrate cephalad on the pelvis under vertical load. It is a longitudinal and rotational instability, so the fixation must span from the lumbar spine to the ilium. Absolute indications
- U-type sacral fractures (bilateral vertical fractures plus a horizontal component).
- H-type sacral fractures (bilateral vertical fractures through the sacral foramina).
- Spinopelvic dissociation with vertical shear instability.
- Denis Zone III bilateral fractures with neurological deficit.
- Roy-Camille Type III transverse fractures at the lumbosacral level. Relative indications
- Unilateral Denis Zone III fracture with a neurological deficit requiring decompression.
- Lumbosacral kyphotic deformity greater than 20 degrees after injury.
- Bilateral Denis Zone II fractures with vertical displacement greater than 1 cm.
- Failed non-operative management of a U- or H-type fracture.
- Polytrauma patients who need early mobilisation with an unstable sacral fracture. Contraindications
- Absolute: active infection at the surgical site, medical instability precluding prolonged surgery, and severe osteoporosis preventing adequate screw purchase.
- Relative: extensive soft-tissue injury requiring delay (the Morel-Lavallée lesion or an open degloving wound), a neurologically intact patient with a minimally displaced fracture, and advanced age with low functional demand. Preoperative imaging. Characterise the fracture and plan screw corridors before scrubbing:
- AP pelvis radiograph — assess pelvic-ring disruption and vertical displacement.
- Inlet view — evaluate posterior displacement and sacral kyphosis.
- Outlet view — assess cranial-caudal displacement and the transverse fracture line.
- CT with 3D reconstruction — define the fracture pattern and canal compromise (the single most important study).
- MRI of the sacrum — evaluate neural compression, disc injury and soft-tissue injury when a deficit is present. Templating. Measure sacral alar width and the iliac corridor on axial CT, plan pedicle-screw trajectory at L4/L5 from pedicle dimensions, template the S2AI trajectory (insertion point, angulation, length), identify the safe zones avoiding the L5 and S1 nerve roots, and plan reduction manoeuvres for any kyphotic deformity. Flag sacral dysmorphism (about 25 percent prevalence) — it narrows the trans-sacral corridor and demands careful templating. Consent and setup. Consent specifically for neurological injury (5–15 percent), screw loosening or pullout (10–20 percent), wound infection (2–8 percent) and symptomatic hardware prominence (20–30 percent with traditional PSIS iliac screws, about 5 percent with S2AI screws). Plan for prone positioning on a radiolucent table, intraoperative neuromonitoring and generous cross-matched blood.
The Operation
The goal is to re-establish a continuous bony column from the lumbar spine to the pelvis, restore lumbosacral alignment (correcting the sacral kyphus), decompress the sacral roots when indicated, and rigidly stabilise the construct so the patient can be mobilised early. The operation is a midline posterior approach: expose the lumbar posterior elements, sacrum and iliac crests; instrument from L5 (± L4) down to the pelvis with iliac or S2AI screws; connect the anchors with contoured rods and cross-connectors; reduce the fracture; and decompress if there is a deficit. The exposure is laid out in full as the first steps below — it is the foundation of a safe, well-placed construct.
Operative sequence
- Prone on a radiolucent Jackson table or OSI frame with the abdomen free to reduce epidural venous pressure and blood loss; pad the chest and iliac crests, position the arms on boards or tucked, ensure the genitalia are free in males, and pad every pressure point.
- Confirm full fluoroscopic visibility (AP pelvis, inlet, outlet and lateral) before prepping, and apply intraoperative neuromonitoring (MEP/SEP).
A free abdomen reduces venous bleeding and improves the operative field. Excessive hip flexion limits sacral reduction, and an inadequate headrest risks facial or eye injury — check these before draping.
- Abdominal compression increases venous bleeding.
- Excessive hip flexion limits sacral reduction.
- Inadequate padding causes pressure ulcers.
- Eye or facial injuries come from an improper headrest.
- Midline incision from the L4 spinous process to the sacral hiatus (approximately 18–22 cm).
- Deepen through skin and subcutaneous fat with electrocautery, then incise the thoracolumbar fascia in the midline.
- Use a Cobb elevator to elevate the paraspinal muscles subperiosteally off the spinous processes bilaterally.
Stay strictly subperiosteal to avoid muscle ischaemia and denervation. Identify the L4 and L5 spinous processes by palpation — L4 intersects the iliac-crest line. Coagulate the muscular branches of the lumbar arteries close to bone.
- Superficial wound infection runs 8–12 percent in trauma cases.
- Excessive undermining causes skin necrosis.
- Injury to cutaneous nerves causes painful neuromas at the incision.
- Expose the lamina, facets and transverse processes of L4 and L5.
- Use a Penfield elevator to define the pedicle boundaries. L4 entry is 2–3 mm lateral to the midpoint of the facet line; L5 entry is at the junction of the transverse process, superior articular process and lateral pars.
The L5 transverse process is short and stubby — identify it by tracing the facet line caudally; the mamillary process marks the superior pedicle boundary. Avoid excessive lateral dissection to protect the L5 nerve root crossing the sacral ala.
- L5 nerve root injury from lateral dissection or retractor placement.
- Facet joint violation compromises future fusion options.
- Dural tear if dissection extends too far medially.
- Extend the subperiosteal dissection laterally over the sacral ala to the SI joint.
- Elevate the multifidus and erector spinae from the posterior sacrum and expose the PSIS bilaterally.
- If using S2AI screws, identify the S1 dorsal foramen (a palpable dimple about 15–20 mm from the midline) — it is the key landmark for the S2AI starting point.
Stay posterior and superior. The superior gluteal artery exits the pelvis through the greater sciatic foramen at the superior border of piriformis, hugging the bone just below the apex of the greater sciatic notch — keep the dissection subperiosteal and do not stray into the notch. Use sponge sticks to control venous ooze from fracture surfaces.
- Superior gluteal artery injury causes massive bleeding.
- Anterior cortex penetration risks the presacral vessels.
- Inadequate exposure leads to malpositioned screws.
- Palpate the sacral fracture lines and assess displacement and instability with gentle manual pressure; identify comminution.
- Use intraoperative fluoroscopy (AP pelvis, inlet, outlet) and evaluate any canal compromise requiring decompression.
Measure lumbosacral kyphosis on lateral fluoroscopy (normal 30–45 degrees), assess vertical displacement on AP and outlet views, and plan reduction manoeuvres before instrumentation. Temporary Schanz pins can aid manipulation.
- Missed injury patterns lead to inadequate fixation.
- Excessive manipulation causes neurological deterioration.
- Handling can propagate an undisplaced fracture line.
- Use anatomic landmarks or image guidance. Make the starting point with a burr or awl, palpate the pedicle with a curved probe (gear-shift technique), confirm four-wall integrity with a ball-tip probe, then tap and measure depth.
- Insert polyaxial pedicle screws (6.5–7.5 mm diameter, 40–50 mm length) and confirm position with fluoroscopy and neurophysiological monitoring.
Use a convergent medial trajectory of 25–35 degrees with 10–15 degrees of caudal angulation to follow the endplate. Deeper insertion (45–50 mm) gives better purchase; bicortical purchase is not necessary and risks anterior vessel injury.
- Nerve root injury in 1–3 percent from a medial or inferior breach.
- Dural tear with medial pedicle wall violation.
- Screw loosening if purchase is inadequate in osteoporotic bone.
- Anterior cortex penetration risks the iliac vessels.
- Entry at the PSIS, 1–2 mm lateral to its lateral edge. Trajectory is 40–45 degrees lateral in the axial plane and 20–30 degrees caudal in the sagittal plane, aiming toward the AIIS.
- Confirm the corridor between the inner and outer tables with fluoroscopy, drill with a 3.2 mm then 4.0 mm bit, measure depth (usually 70–90 mm), tap and insert a 7.5–8.5 mm screw.
The inlet view shows medial-lateral position, the outlet view shows superior-inferior position, and the oblique view visualises the full trajectory. Feel the resistance changes — hard cortex at entry, softer cancellous bone, then hard anterior cortex — and do not penetrate the anterior cortex.
- Superior gluteal artery injury if the trajectory is too inferior or medial.
- Iliac crest fracture with excessive force during tapping.
- Prominent hardware at the PSIS causes pain and needs later removal in 20–30 percent.
- Screw cutout through the outer table with an incorrect trajectory.
- Entry at the level of the S1 dorsal foramen on the sacral slope (about 1 mm lateral and inferior to it; in deformity practice the S2 starting point sits roughly 25 mm caudal and 22 mm lateral to the S1 endplate and midline per Chang et al.).
- Starting trajectory is about 40 degrees lateral in the transverse plane and 30–40 degrees caudal in the sagittal plane, aiming toward the AIIS. Palpate the S1 and S2 pedicle boundaries, pass a guidewire under fluoroscopy (the teardrop or obturator-outlet view confirms the iliac corridor), drill over the wire, measure depth (commonly 80–120 mm) and insert a cannulated 7.5–8.5 mm screw across the SI joint into the supra-acetabular ilium.
(1) The starting point is closer to the midline, so rods contour more easily and sit in line with the S1 pedicle; (2) 30–40 percent greater pullout strength; (3) lower prominence and pain; (4) a lower removal rate (about 5 percent versus 25 percent); (5) it crosses the SI joint for additional stability; (6) it can be placed percutaneously.
- L5 nerve root risk if the trajectory is too superior or medial.
- S1 nerve root risk if the starting point is too medial.
- Anterior cortex penetration risks the presacral vessels.
- Inadequate length gives suboptimal fixation.
- Measure the distance between screw heads and contour a 5.5 mm or 6.0 mm titanium or cobalt-chromium rod to restore lumbar lordosis and correct the sacral kyphus.
- Insert the rods into the screw heads, usually starting caudal and working cephalad, using rod holders and persuaders to achieve a provisional reduction.
Pre-bend the rods to restore normal lumbosacral alignment (lumbar lordosis 40–60 degrees, sacral slope 30–45 degrees). Create a smooth curve with no sharp bends (they are stress risers). S2AI screws need less rod offset than traditional iliac screws and are easier to connect.
- Excessive force during rod insertion can displace screws.
- Sharp rod bends create fatigue failure points.
- Incomplete seating prevents a solid connection.
- Use the rods as reduction tools: compress to close vertical fracture gaps and apply an extension force to correct the kyphotic deformity; temporary Schanz pins in the sacrum can aid manipulation.
- Confirm reduction with fluoroscopy — AP pelvis (vertical displacement), inlet (posterior displacement), outlet (cranial-caudal displacement) and lateral (kyphosis).
For vertical displacement, compress along the rod; for kyphosis, extend the lumbosacral junction (sometimes a prone positioning adjustment helps); for rotation, de-rotate around the bilateral fixation points. Up to 5–10 mm of residual displacement is acceptable if the patient is neurologically intact.
- Neurological deterioration from manipulation.
- Screw pullout with excessive force.
- Propagation of undisplaced fracture lines.
- Over-correction into hyperlordosis.
- Provisionally tighten all set screws, recheck reduction and alignment, then definitively tighten them sequentially (not alternating) to about 8–10 Nm of torque.
- Confirm there is no screw toggle or rod slippage.
Start at the apex of the construct (L5 or S1) and work toward the ends (L4 and the iliac or S2AI screws) so you do not lock in malalignment. Recheck reduction after each screw is tightened, and use a torque-limiting driver for the final 8–10 Nm.
- Screw head fracture with excessive torque.
- Construct failure if undertightened.
- Rod slippage if not properly seated before tightening.
- Measure the distance between the bilateral rods and apply cross-connectors at two levels (typically one proximal near L4–L5 and one distal near the sacrum).
- Tighten the cross-connector screws and confirm construct rigidity with gentle manual stress.
Cross-connectors increase torsional rigidity by about 45 percent and are essential for bilateral unstable injuries. Offset the connectors axially for maximum rigidity, and consider multiple connectors for long constructs.
- Prominent connectors cause discomfort.
- Inadequate tightening allows micromotion.
- Excessive length prevents skin closure.
- If the anterior pelvic ring is unstable or lumbopelvic fixation is inadequate, place percutaneous SI screws from a lateral sacral entry below the iliac crest.
- Trajectory is perpendicular to the fracture plane and parallel to the S1 superior endplate; confirm position in inlet, outlet and lateral views and insert a 7.3 mm or 8.0 mm cannulated screw across the SI joint into the S1 body.
(1) Unilateral fixation needing contralateral SI stabilisation; (2) a comminuted sacral ala fracture; (3) osteoporotic bone needing augmentation; (4) a vertical shear pattern needing compression across the SI joint. Place SI screws before the lumbopelvic fixation when possible for an easier trajectory.
- L5 nerve root injury if the trajectory is too superior (stay parallel to the S1 endplate).
- Anterior cortex penetration risks the iliac vessels.
- A screw that is too short gives inadequate purchase.
- A dysmorphic sacrum (25 percent prevalence) demands careful templating.
- Perform a laminectomy of the involved sacral segments using Kerrison rongeurs and a high-speed burr; remove bone fragments compressing the nerve roots and decompress the central canal and lateral recesses.
- Preserve the posterior tension band if possible, and confirm the decompression by visualising the dura and nerve roots.
Acute deficit (within 8 hours): emergent decompression. Subacute (8–72 hours): urgent decompression improves outcomes. Chronic (greater than 2 weeks): limited recovery potential; decompress for pain. An incomplete cauda equina injury has a better prognosis than a complete one.
- Dural tear needs meticulous repair (high CSF leak risk in the sacrum).
- Nerve root injury from manipulation.
- Destabilisation if excessive bone is removed.
- Persistent deficit despite adequate decompression.
- Obtain AP pelvis, inlet, outlet and lateral radiographs and confirm: screw positions within bone, adequate reduction, no hardware impingement on neural structures, and restored alignment; perform final neurophysiological checks.
- Copious irrigation (3–6 litres with bacitracin or chlorhexidine), place a drain only if there is extensive dead space, close the fascia with Number 1 absorbable suture, the subcutaneous layer with 2-0 absorbable suture, and the skin with staples or a subcuticular suture.
AP: screw trajectories, vertical displacement reduced. Inlet: posterior displacement corrected, iliac or S2AI screws in the corridor. Outlet: cranial-caudal displacement reduced, transverse sacral screws below L5-S1. Lateral: lumbosacral kyphosis corrected, no anterior screw penetration.
- A missed screw malposition causes postoperative neurological deficit.
- Incomplete reduction leads to progressive deformity.
- Wound dehiscence if the fascia is not properly closed; deep infection risk 2–8 percent in the trauma setting.
Aftercare & Complications
Immediate postoperative management (first 24–48 hours)
- ICU or a monitored bed for polytrauma patients, with neurological checks (motor, sensory, bowel and bladder) every 2 hours.
- DVT prophylaxis: chemical (enoxaparin 40 mg subcutaneously daily) plus mechanical (sequential compression devices).
- Multimodal analgesia (PCA, oral opioids, acetaminophen, gabapentin); a Foley catheter if there is bowel or bladder dysfunction, otherwise early removal.
- Remove drains when output is less than 30 mL per 8-hour shift (typically 24–48 hours), watching for excessive drainage that suggests a CSF leak.
- Postoperative AP pelvis and lateral lumbosacral radiographs in recovery; a CT scan if there is any deficit or concern for malposition. Weight-bearing and bracing | Phase | Timing | Weight-bearing | Notes | |-------|--------|----------------|-------| | 1 | 0–6 weeks | Touch-down (crutches or walker) | Protect fixation; early sacral fracture healing is slow (12–16 weeks) | | 2 | 6–12 weeks | Partial (50 percent) if radiographic healing | Gentle ROM, core stabilisation | | 3 | 12 weeks and beyond | Weight-bearing as tolerated if union is progressing | Advance to strengthening; discontinue any brace | An LSO (or a rigid TLSO with thigh extension for vertical shear injuries) is used for 12 weeks or until radiographic union in comminuted fractures, osteoporotic patients or when fixation stability is questionable — there is no high-level evidence supporting it after rigid internal fixation, but it may improve comfort and compliance. S2AI fixation with excellent purchase may advance to weight-bearing as tolerated at 8 weeks; osteoporotic patients should extend protected weight-bearing to 16 weeks. Follow-up schedule
- 2 weeks: wound check and suture or staple removal; repeat the neurological exam; AP pelvis and lateral lumbosacral radiographs.
- 6 weeks: clinical exam; radiographs to check hardware and alignment; advance to partial weight-bearing if healing appropriately.
- 12 weeks: radiographs and a CT if needed to assess healing; advance to full weight-bearing if union is evident; discontinue the brace.
- 6 months: assess functional outcome and confirm union; address persistent hardware prominence, SI pain or neurological deficit.
- 12 months: final assessment for union, alignment and functional recovery; discuss hardware removal if prominent and symptomatic after confirmed union. Complications
- Recognition
- New motor or sensory deficit, loss of bowel or bladder function, foot drop, saddle anaesthesia; intraoperative MEP or SEP change; postoperative imaging shows screw malposition or haematoma
- Prevention
- Anatomic screw placement, image guidance, neuromonitoring, pedicle probing, stay within safe zones, gentle retraction
- Management
- Immediate CT; remove an offending screw; emergent decompression for haematoma or compression; serial exams; EMG at 3–4 weeks, explore if no recovery
- Recognition
- Progressive pain after initial improvement, loss of reduction on serial radiographs, a radiolucent halo around screw threads, construct failure
- Prevention
- Maximise purchase (bicortical iliac or S2AI screws, 7.5–8.5 mm diameter, 90–120 mm length); smoking cessation, vitamin D; cement augmentation if osteoporotic
- Management
- Observe if asymptomatic in a healed fracture; revise with longer screws, cement augmentation, or extend the construct; rule out infection; bone graft for nonunion
- Recognition
- Superficial: erythema, drainage, fluctuance within 2–4 weeks. Deep: persistent pain, fever, raised inflammatory markers, purulent drainage, implant loosening
- Prevention
- Preop cefazolin 2 g within 60 min and redose every 4 h; minimise operative time and soft-tissue trauma; meticulous haemostasis; copious irrigation; normothermia and euglycaemia
- Management
- Superficial: oral antibiotics and wound care. Deep: irrigation and debridement, tissue cultures, 6 weeks of IV antibiotics; retain stable hardware within 4 weeks, remove if loose or biofilm-laden
- Recognition
- Persistent pain beyond 6 months, no healing on CT at 3–6 months, progressive deformity, screw halo or hardware failure
- Prevention
- Anatomic reduction, rigid fixation (L5 to iliac or S2AI minimum), supplemental SI screws, bone grafting for comminuted fractures, smoking cessation, vitamin D 25–40 ng/mL
- Management
- Nonunion: revise with construct extension and bone grafting. Malunion: corrective osteotomy if severe deformity causes deficit, otherwise observe
- Recognition
- Palpable PSIS screws uncomfortable with sitting or lying supine, pain with direct pressure, overlying bursa; fracture healed on imaging
- Prevention
- Use S2AI screws (primary prevention); seat iliac screws fully; low-profile tulip heads; warn patients preoperatively
- Management
- Conservative for 6–12 months (cushioning, NSAIDs); hardware removal after union (minimum 12–18 months), removing iliac or S2AI screws bilaterally; retain pedicle screws and rods if asymptomatic
- Recognition
- Buttock pain radiating to the posterior thigh, pain with prolonged sitting or standing, positive FABER, Gaenslen or sacral thrust; diagnostic injection gives temporary relief
- Prevention
- Anatomic fracture reduction; avoid SI joint violation; early mobilisation
- Management
- Conservative first (physiotherapy, NSAIDs, SI injections every 3–6 months); refractory cases: SI joint fusion or lateral-branch radiofrequency ablation
- Recognition
- Sagittal imbalance with a stooped posture and forward trunk lean, mechanical back pain; lateral radiograph shows lumbosacral kyphosis greater than 10 degrees or lumbar lordosis less than 40 degrees
- Prevention
- Intraoperative reduction of the kyphus with the rods as reduction tools; restore lumbar lordosis 40–60 degrees and sacral slope 30–45 degrees; confirm on lateral fluoroscopy before final tightening
- Management
- Mild (10–20 degrees): conservative. Moderate to severe (greater than 20 degrees) with disability: corrective osteotomy (Smith-Petersen or pedicle subtraction), extending the fusion — complex, with a 30–40 percent complication rate
Risk factors for complications
- Patient: diabetes (about 3 times the infection risk), smoking (about 2 times the nonunion risk), obesity with BMI greater than 35 (about 2.5 times the wound-complication risk), osteoporosis (more screw loosening), polytrauma with ISS greater than 25.
- Surgical: operative time greater than 4 hours, estimated blood loss greater than 1000 mL, extensive soft-tissue stripping, inadequate reduction, suboptimal screw placement.
- Injury: open fracture or degloving injury, neurological deficit at presentation, severe comminution, associated visceral injuries, delay to fixation greater than 3 weeks (scarring and malunion).
Viva & Exam Focus
SACRALSACRAL — recognising spinopelvic dissociation
Hook:Spinopelvic dissociation needs BOTH bilateral vertical sacral fractures AND disruption across the ring for complete instability — a single vertical line is not a dissociation.
ILIACILIAC — the S2-alar-iliac screw trajectory
Hook:The S2AI starting point sits about 15 mm deeper than the PSIS entry, lowering implant prominence and removal rates while keeping the anchor in line with the S1 pedicle screws for easy rod connection.
Across the whole operation the constant dangers are the cauda equina and sacral nerve roots, the L5 nerve root crossing the sacral ala, the superior gluteal artery at the greater sciatic notch, the presacral venous plexus behind the anterior sacral cortex, and the compromised posterior skin envelope. Each step below is built around protecting these.
Location: within the sacral canal, exiting through the dorsal foramina. Protection: careful dissection over the sacral ala, avoid violating the sacral canal unless decompression is indicated, and identify fracture fragments compressing neural elements.
Location: crosses the sacral ala at the S1 pedicle level, about 15–20 mm from the midline. Protection: identify the transverse process and ala junction, stay subperiosteal, and avoid aggressive lateral retraction during L5 pedicle screw and S2AI placement.
Location: exits the greater sciatic notch at the superior border of piriformis and crosses the iliac wing medially. Protection: stay posterior and superior to the notch during iliac dissection, control bleeding with bone wax or bipolar, and do not penetrate the anterior cortex with iliac screws.
Location: anterior to the sacrum between the periosteum and the presacral fascia. Protection: maintain subperiosteal dissection, avoid an anterior cortex breach during S2AI placement, have haemostatic agents ready, and consider preoperative embolisation for a displaced fracture.
Location: often compromised by the high-energy trauma, oedema and degloving. Protection: delay surgery 5–7 days if significantly swollen, use modified incisions for open wounds, avoid excessive undermining, and consider a staged approach with external fixation first.
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 28-year-old motorcyclist has sustained a U-type sacral fracture in a high-speed collision. Walk me through your surgical plan for lumbopelvic fixation — the critical steps and the potential pitfalls.”
“You are placing an S2-alar-iliac screw and encounter brisk bleeding that is difficult to control. What is your differential diagnosis and immediate management?”
“Six months postoperatively your patient with lumbopelvic fixation for spinopelvic dissociation complains of persistent buttock pain and painful hardware prominence at the PSIS. What is your assessment and management plan?”
Indications
- U-type sacral fractures (bilateral vertical plus a horizontal component)
- H-type sacral fractures (bilateral vertical through the foramina)
- Complete spinopelvic dissociation with vertical shear instability
- Denis Zone III bilateral fractures with neurological deficit (about 57 percent neuro injury in the Denis series)
- Roy-Camille Type III transverse fractures with lumbosacral involvement
- Unilateral Zone III with neurological deficit needing decompression
- Failed non-operative management or lumbosacral kyphosis greater than 20 degrees
Key anatomy at risk
- L5 nerve root crosses the sacral ala 15–20 mm from the midline at the S1 pedicle level — at risk in lateral dissection and S2AI placement
- Superior gluteal artery exits the greater sciatic notch at piriformis — injured by an inferior or medial trajectory or anterior cortex penetration
- Sacral canal contains the cauda equina — about 57 percent neurological injury in Denis Zone III fractures, often needs decompression
- Iliac corridor between the inner and outer tables is 8–15 mm wide — the S2AI target with 40–45 degrees lateral and 20–30 degrees caudal angulation
- S2AI entry is at the level of the S1 dorsal foramen on the sacral slope — safer and stronger than the traditional PSIS entry
Critical steps
- Prone on a radiolucent table with a free abdomen to reduce epidural venous pressure
- Midline exposure L4 to sacrum with subperiosteal dissection of the paraspinals
- L5 (± L4) pedicle screws: entry at the transverse process or SAP junction, 25–35 degrees medial convergence, 45–50 mm length
- S2-alar-iliac screws (preferred) or traditional iliac screws: 40–45 degrees lateral, 20–30 degrees caudal, 90–120 mm length for bicortical purchase
- Rod contouring to restore lordosis (40–60 degrees) and correct the kyphus; compression closes fracture gaps
- Cross-connectors at two levels for rotational stability (about 45 percent more torsional rigidity)
- Consider supplemental SI screws if the anterior ring is unstable, and neural decompression if a deficit is present
Danger zones
- L5 nerve root: lateral sacral ala dissection and medial or superior S2AI malposition — stay posterior and superior
- Superior gluteal artery: the sciatic notch during iliac exposure and anterior cortex penetration — subperiosteal dissection, avoid the anterior wall
- Presacral venous plexus: anterior sacral cortex breach — use a guidewire and measure screw length carefully on the preop CT
- Cauda equina and sacral roots: excessive reduction force, or inadequate decompression when indicated — gentle manipulation, wide decompression if needed
- Skin and soft tissue: high-energy trauma and swelling — delay 5–7 days if oedematous, avoid tension, consider a staged approach
Technique pearls
- S2AI screws have 30–40 percent greater pullout than PSIS iliac screws, lower prominence (5 percent versus 25 percent) and easier rod connection
- Cross-connectors are mandatory for bilateral constructs — offset placement at proximal and distal levels maximises rigidity
- Restore sagittal alignment: an uncorrected lumbosacral kyphus causes mechanical pain and progressive deformity — check lateral fluoroscopy
- Four-wall pedicle probing is essential for L5 screws — a medial wall breach risks the nerve root
- Reduce before final tightening: compression closes vertical gaps and extension corrects the kyphus — accept 5–10 mm residual displacement if neurologically intact
Complications
- Neurological injury 5–15 percent: screw malposition (immediate removal), haematoma (emergent decompression), reduction force (observe)
- Screw loosening 10–20 percent: optimise purchase (bicortical S2AI 90–120 mm), cement augmentation if osteoporotic, revise if symptomatic
- Infection 2–8 percent: preop antibiotics, minimise operative time; superficial (oral antibiotics), deep (irrigation and debridement plus 6 weeks IV)
- Hardware prominence 20–30 percent PSIS iliac, 5 percent S2AI: remove after union (12–18 months); S2AI preferred for prevention
- Nonunion 5–10 percent: anatomic reduction, rigid fixation, smoking cessation, revision with bone graft if persistent
- Lumbosacral kyphosis 15–20 percent: intraoperative reduction is mandatory; corrective osteotomy if severe postoperative deformity (greater than 20 degrees)
Post-op protocol
- Weight-bearing: touch-down 0–6 weeks, partial 50 percent 6–12 weeks, as tolerated 12 weeks and beyond if union is progressing
- Bracing: an LSO for 12 weeks if comminuted or osteoporotic (controversial; no high-level evidence)
- DVT prophylaxis: enoxaparin 40 mg subcutaneously daily plus sequential compression devices until ambulatory
- Follow-up: 2 weeks (wound), 6 weeks (advance weight-bearing if healing), 12 weeks (full weight-bearing if union), 6 months (assess outcome)
- Physical therapy: phase 1 (0–6 weeks) protection and gentle ROM, phase 2 (6–12 weeks) progressive loading, phase 3 (12–24 weeks) strengthening
- Hardware removal: minimum 18–24 months if symptomatic, confirm union on CT, remove the iliac or S2AI screws (retain the pedicle screws)
Background & Evidence
Injury pattern and epidemiology. Spinopelvic dissociation is a rare, high-energy injury — classically a suicide-jumper's fracture or a high-speed motor-vehicle or fall mechanism — in which bilateral vertical sacral fractures (joined by a transverse component) separate the spine from the pelvis. Neurological deficit is present in roughly half of U- and H-type fractures (about 56 percent in the landmark series), frequently a cauda equina syndrome with saddle anaesthesia and sphincter loss. Classification — Denis zones (sacral fracture location). The Denis three-zone system, drawn from a retrospective analysis of 236 sacral fractures, predicts neurological risk and underpins operative decision-making.
- Anatomy
- Lateral to the foramina (sacral ala)
- Neurological injury
- About 6 percent (occasionally the L5 root)
- Anatomy
- Through the foramina (transforaminal)
- Neurological injury
- About 28 percent (frequently sciatica; rarely bladder dysfunction)
- Anatomy
- Central canal involvement
- Neurological injury
- About 57 percent (saddle anaesthesia, sphincter loss) — most often needs decompression
Classification — Roy-Camille types (transverse sacral fractures). Applied to the transverse component that joins the vertical limbs in a U- or H-type pattern.
- Mechanism
- Flexion
- Distal fragment
- Flexed
- Mechanism
- Extension
- Distal fragment
- Extended
- Mechanism
- Comminuted or vertical shear
- Distal fragment
- Retropulsed — the pattern of spinopelvic dissociation
AO/OTA framing. A complete pelvic-ring disruption with sacral involvement codes as 61-C3; a posterior arch injury with spinopelvic dissociation codes as 12-C. Surgical anatomy
- Lumbar spine: the L4 pedicle is about 10–15 mm in transverse width and 15–20 mm high with 10–15 degrees of medial angulation; the L5 pedicle is 15–20 mm wide and 20–25 mm high with 25–35 degrees of medial angulation. The L5 transverse process gives attachment to the iliolumbar ligament and is the lateral boundary.
- Sacrum: the S1 pedicle is the largest sacral pedicle (20–25 mm diameter); the S1 dorsal foramen sits 15–20 mm from the midline and is the landmark for the S2AI entry; the sacral ala lies between the L5-S1 facet and the SI joint, and the sacral promontory (anterior superior edge) puts the L5 root at risk.
- Pelvis: the PSIS is the entry for traditional iliac screws and the AIIS the target; the iliac corridor between the inner and outer tables is 8–15 mm wide; the greater sciatic notch is the inferior boundary and contains the superior gluteal vessels.
- Neural: the cauda equina terminates at L1–L2 and fills the sacral canal; the L5 root exits the L5-S1 foramen and crosses the sacral ala; the sacral roots S1–S5 exit through the anterior and posterior foramina; the coccygeal plexus (S4–Co1) supplies bladder, bowel and sexual function. Biomechanics and construct choice. Vertical shear needs longitudinal fixation spanning the injury; rotational instability needs cross-connectors between the bilateral rods; and an uncorrected kyphotic deformity is a lever arm for progressive collapse.
- Role
- High sacral fractures or osteoporotic bone
- Note
- Longest lever arm, the most fixation
- Role
- Standard for most spinopelvic dissociations
- Note
- The workhorse construct
- Role
- Low-profile distal anchor
- Note
- 30–40 percent greater pullout than PSIS iliac screws; removal about 5 percent versus 25 percent
- Role
- Link the bilateral rods
- Note
- Increase torsional rigidity by about 45 percent
Key evidence. The landmark Schildhauer series of 19 patients established that decompression and lumbopelvic fixation reliably maintain reduction and correct sacral kyphosis (mean kyphosis improved from 43 to 21 degrees), with 83 percent recovery of bowel or bladder function — neurological prognosis was driven by sacral root continuity and injury completeness, not by the construct itself. The companion Bellabarba series documented the complications to anticipate: connecting-rod fracture in 31 percent (usually asymptomatic) and wound-healing problems in 26 percent. The Chang CT study defined the S2AI corridor (a roughly 40-degree lateral and 39-degree caudal trajectory, mean length 105 mm, starting point about 15 mm deeper than the PSIS), which is why S2AI is now the preferred distal anchor. Gardner and Routt described transiliac-transsacral screws as a powerful adjunct to the horizontal limb of fixation, useful in osteoporosis, obesity and bilateral posterior injuries — but mandating careful templating because the screw traverses both alar zones.
References
Decompression and lumbopelvic fixation for sacral fracture-dislocations with spino-pelvic dissociation
- 19 patients (18 with a minimum 12-month follow-up) with highly displaced, comminuted Roy-Camille type 2–4 sacral fractures and cauda equina deficits treated with open reduction, sacral decompression and lumbopelvic fixation
- All fractures healed without loss of reduction; mean sacral kyphosis improved from 43 to 21 degrees
- 15 of 18 patients (83 percent) had full or partial recovery of bowel or bladder function; 10 of 18 (56 percent) had improved Gibbons neurological scores
- Complete cauda equina recovery was far more likely with continuity of all sacral roots (86 percent versus 0 percent) and with incomplete deficits (100 percent versus 20 percent)
Complications associated with surgical stabilization of high-grade sacral fracture dislocations with spino-pelvic instability
- 19 consecutive patients (mean age 32) with sacral fracture-dislocations and cauda equina syndrome treated by lumbar pedicle-to-iliac screw segmental fixation through a midline posterior approach
- Reduction was maintained in all patients and early mobilisation without external immobilisation was achieved
- Major complications: connecting-rod fracture in 6 of 19 (31 percent) and wound-healing disturbance in 5 of 19 (26 percent); rod breakage was typically asymptomatic
- 14 of 19 (74 percent) had a traumatic dural tear or root avulsion at surgery; no chronic osteomyelitis occurred
Low profile pelvic fixation: anatomic parameters for sacral alar-iliac fixation versus traditional iliac fixation
- 3D CT analysis of 20 pelves defining the sacral alar-iliac (S2AI) corridor: mean starting point 25 mm caudal to the S1 endplate and 22 mm lateral to the sacral midline
- Mean trajectory was 40 degrees lateral in the transverse plane and 39 degrees caudal in the sagittal plane
- Maximal S2AI length averaged 105 mm; the path traversed about 35 mm of sacral ala with a narrowest iliac width of about 12 mm
- The S2AI starting point lies about 15 mm deeper than the PSIS entry, placing the anchor in line with the S1 pedicle screws
Transiliac-transsacral screws for posterior pelvic stabilization
- Transiliac-transsacral screws pass from one iliac cortex across the entire upper sacrum to exit the contralateral iliac cortex, improving holding power over standard unilateral iliosacral screws
- They can simultaneously stabilise bilateral posterior pelvic injuries that would otherwise need two separate screws
- Particularly useful in osteoporosis, obesity, anticipated non-compliance, bilateral posterior injuries, spinopelvic dissociation and nonunion procedures
- Safe insertion requires both upper sacral alar safe zones to be confirmed on inlet, outlet and lateral fluoroscopy because the screw traverses both alae
Sacral fractures: an important problem. Retrospective analysis of 236 cases
- Retrospective study of 236 sacral fractures within 776 pelvic injuries, supported by an anatomic study of 39 cadavers, defining the three-zone classification
- Zone I (ala) carried neurological injury in about 6 percent, occasionally involving the L5 root
- Zone II (transforaminal) carried roughly 28 percent neurological injury, frequently sciatica but rarely bladder dysfunction
- Zone III (central canal) carried about 57 percent neurological injury, frequently saddle anaesthesia and loss of sphincter function
Transverse fracture of the upper sacrum. Suicidal jumper's fracture
- The original description of the transverse upper sacral ('suicidal jumper's') fracture and the three-type Roy-Camille classification based on the position of the distal fragment
- Type I is a flexion injury (distal fragment flexed), Type II an extension injury (distal fragment extended), and Type III a comminuted retropulsed injury — the pattern underlying spinopelvic dissociation