Percutaneous Single Central Screw Fixation | Paediatric
- Loder classification: Stable (can weight-bear) = less than 5% AVN; Unstable (cannot weight-bear) = 20-50% AVN
- Unstable SUFE is an orthopaedic emergency requiring surgery less than 24 hours to minimise AVN risk
- Southwick angle on frog-lateral: Mild less than 30 degrees, Moderate 30-50 degrees, Severe greater than 50 degrees
- Single screw center-center position: perpendicular to physis, tip 5mm from subchondral bone
- Klein line on AP: a line along the superior femoral neck should intersect the lateral epiphysis (it fails in SUFE)
- “SUFE epidemiology: peak 10-16 years, M:F ratio 2:1, around 80% obese, 20-40% bilateral
- “Drehmann sign: obligate external rotation with passive hip flexion (pathognomonic)
- “DO NOT attempt forceful reduction of stable chronic slips - it increases AVN risk
- “Prophylactic contralateral pinning if: age less than 10, endocrine cause, or unable to follow-up
When & Why
Indication. A confirmed slipped upper femoral epiphysis (SUFE/SCFE) of any severity. The single partially-threaded cannulated screw locks the epiphysis to the metaphysis in situ and prevents further slip while the physis fuses. In situ fixation is the global standard of care for stable SUFE; unstable SUFE is an orthopaedic emergency. Absolute indications
- All SUFE regardless of severity (prevents further slip).
- Unstable SUFE (cannot weight-bear at all): emergency surgery within 24 hours.
- Stable SUFE (can weight-bear, with or without crutches): semi-urgent surgery within days. Prophylactic contralateral pinning is offered when the risk of a contralateral slip outweighs the small surgical risk:
- Age less than 10 years (up to 60% bilateral risk).
- An endocrine/metabolic cause: hypothyroidism (about 50% bilateral), renal osteodystrophy (about 60% bilateral), growth hormone deficiency (30-50% bilateral).
- Inability to reliably follow up (remote, non-compliant).
- A symptomatic contralateral hip without a visible slip. Contraindications to in situ pinning. None are absolute — even severe slips are pinned in situ by most surgeons. The relative exception is a severe slip (greater than 50 degrees) in an unstable acute presentation at an experienced centre, where a modified Dunn capital realignment may be considered. Pre-operative imaging essentials.
- AP pelvis showing BOTH hips (20-40% are bilateral).
- Frog-lateral of both hips — the best view for the posterior slip.
- Klein line on the AP (a line along the superior femoral neck should intersect the lateral epiphysis; it fails in SUFE).
- Southwick slip angle on the frog-lateral to grade severity. Timing. Unstable SUFE goes to theatre within 24 hours; stable SUFE within 3-5 days. Consent. Discuss AVN of the femoral head (0.5-5% stable, 20-50% unstable), chondrolysis (1-5%), screw penetration requiring revision (1-3%), a contralateral slip if not pinned (20-40%), slip progression (1-3%), late femoroacetabular impingement (30-70%, severity dependent), the likely need for screw removal after physeal closure, and the small risks of infection (less than 1%) and femoral nerve palsy (less than 0.5%, traction-related). Counsel on weight-bearing restriction for 6 weeks, activity restriction for 3-6 months, and long-term monitoring until skeletal maturity.
The Operation
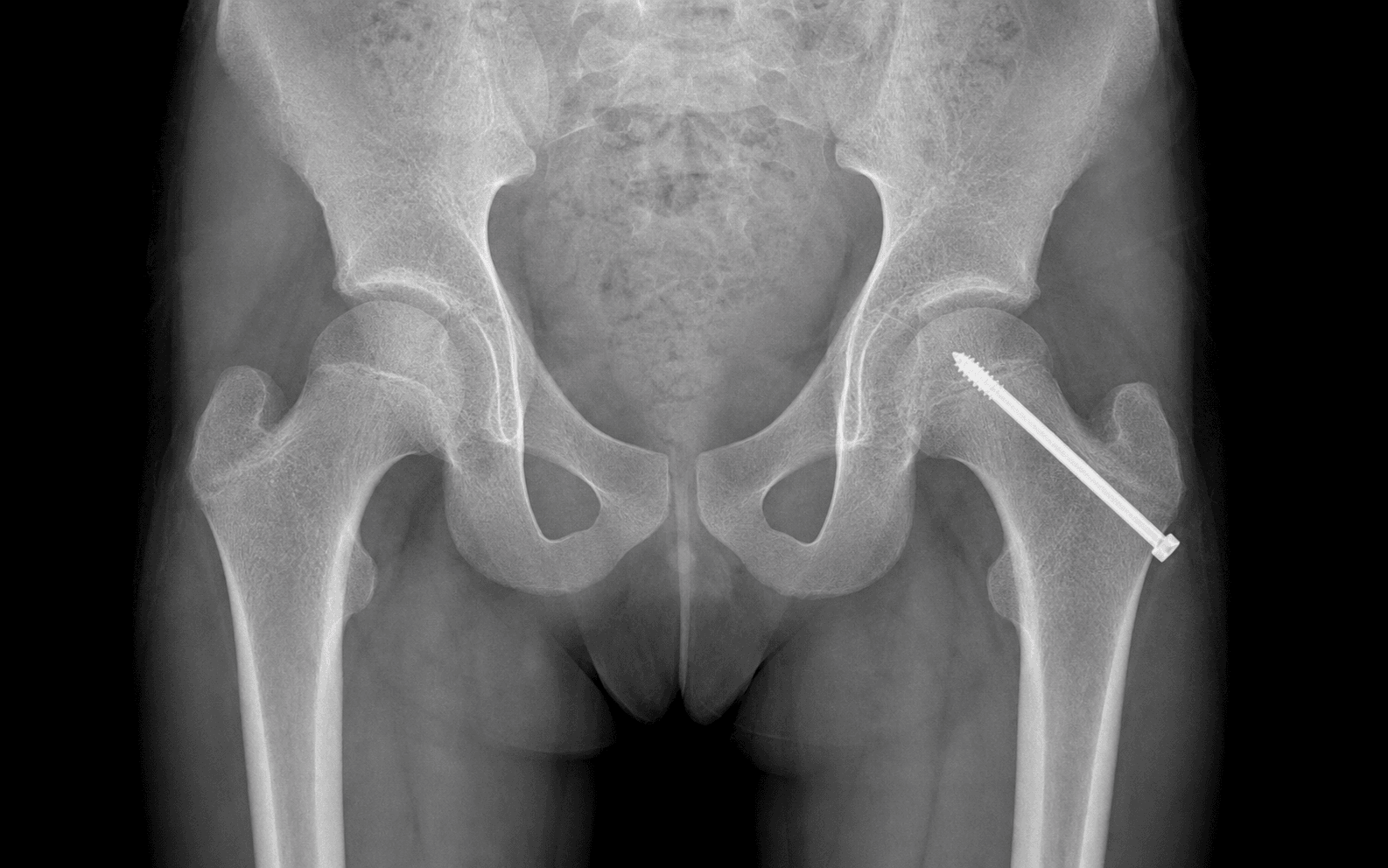
The goal is to stabilise the slipping epiphysis with a single partially-threaded cannulated screw placed exactly center-center, perpendicular to the physis, with every thread across the physis into the epiphysis and the tip 5mm from subchondral bone. This is a percutaneous procedure — the "exposure" is positioning on a fracture table and obtaining perfect biplanar fluoroscopy, then a short stab incision and blunt spread down to the anterolateral femoral neck. Do NOT reduce the slip; fix it where it lies.
Operative sequence
- Supine on a radiolucent fracture table (Jackson or OSI); affected leg in a traction boot, contralateral leg abducted widely in the scissor position for C-arm access.
- Apply GENTLE longitudinal traction through the boot only — never attempt forceful reduction (it propagates an unstable slip and shears the retinacular vessels, causing AVN).
- Hip position: 10-15 degrees flexion, 10-20 degrees abduction, neutral rotation (avoid internal rotation). Use a well-padded perineal post.
- C-arm positioned between the legs for biplanar imaging.
- CRITICAL: confirm a true AP (femoral neck perpendicular to the beam, lesser trochanter barely visible medially) and a true lateral (neck in profile, greater trochanter posterior) BEFORE prepping.
- AP view: identify the physis, confirm the Klein line abnormality, and plan the entry point on the anterolateral femoral neck 1-2cm distal to the vastus ridge.
- Lateral view: assess the severity of the posterior slip and plan a trajectory to the CENTER of the epiphysis, accounting for the posterior displacement.
- Lay a guidewire on the skin and adjust it until it overlies the planned entry point on BOTH views, then mark the skin.
- Estimate screw length from the entry point to the center of the epiphysis (typically 80-100mm in adolescents).
- Make a 1-2cm stab incision at the marked anterolateral entry point.
- Divide skin and subcutaneous tissue, then bluntly spread the vastus lateralis fibres with a haemostat down to the bone.
- Palpate the anterolateral surface of the femoral neck.
- LIMITED-OPEN ALTERNATIVE (obese patient, revision, or when an unstable hip needs aspiration): a 2-3cm longitudinal incision, incise the fascia lata, and split vastus lateralis (safe — the nerve enters posteriorly) for direct palpation of the entry point.
- Advance the 2.4mm or 2.8mm guidewire (matched to the screw system) under continuous biplanar fluoroscopy.
- Technique: start perpendicular to bone, angle toward the center of the epiphysis, advance 2-3mm then check AP, advance 2-3mm then check lateral, repeating iteratively across the physis into the epiphysis.
- Final position: center-center, perpendicular to the physis, tip 5mm from subchondral bone.
- Common errors: too posterior on the lateral view (highest AVN risk — redirect anteriorly); too anterior (anterior vessel injury); too superior or inferior (eccentric loading, early physeal closure); inadequate depth (threads will not engage).
- Slide the depth gauge over the guidewire until it seats against bone and read the calibrated marks.
- Select a partially threaded 7.0-7.3mm cannulated screw. The thread length MUST exceed the epiphyseal thickness (typically 16-32mm).
- If the bone is dense, cannulated-drill over the guidewire to 5-10mm short of the final length — never plunge into the epiphysis.
- Thread the screw over the guidewire; an assistant holds the wire stable (a haemostat on the wire prevents it advancing with the screw).
- Advance under fluoroscopy until ALL threads cross the physis into the epiphysis, then continue tightening to compress the physis. Avoid overtightening, which strips the soft epiphyseal bone.
- AP checklist: the screw bisects the center of the femoral head; all threads are across the physis in the epiphysis; the tip is 5mm from subchondral bone; no superior or inferior cortex penetration.
- Lateral checklist: the screw bisects the center of the head; it is perpendicular or minimally oblique to the physis; the tip is 5mm from subchondral bone; NO posterior cortex penetration (critical); no anterior cortex penetration.
- Dynamic test: gently internally rotate and flex the hip — the screw should remain stable with no toggling or backing out.
- Grasp the guidewire with a needle driver, steady the screw head to prevent backing out, withdraw it smoothly, and reconfirm screw position on fluoroscopy.
- Consider pinning the opposite hip if: age less than 10 years, an endocrine/metabolic cause, unreliable follow-up, a symptomatic contralateral hip, or physeal widening.
- If pinning: reposition the C-arm to the contralateral hip, use the identical technique (easier as the anatomy is normal), and complete one side fully before starting the other.
- Irrigate with saline.
- Percutaneous: skin closure only (3-0 or 4-0 absorbable subcuticular). Limited open: fascia lata (2-0 Vicryl), subcutaneous (3-0 Vicryl), skin.
- Apply a sterile dressing. Remove from the traction table with a log roll — avoid twisting.
- NEVER forcefully reduce a stable chronic slip.
- Gentle traction only for unstable acute slips.
- Use a cross-table (shoot-through) lateral for unstable SUFE — a frog-lateral risks further displacement.
- Confirm true AP and true lateral views BEFORE prepping.
- Protect the genitals from perineal-post pressure.
For SUFE, positioning is about visualisation, not reduction. Gentle traction only. Forceful manipulation propagates an unstable slip and shears the retinacular vessels, causing AVN. For an unstable acute slip use a cross-table lateral rather than a frog-lateral to avoid further displacement.
Center-center positioning is the single most important technical step. The screw must bisect the femoral head exactly in the center on BOTH AP and lateral. Posterior malposition carries the highest AVN risk (it injures the posterior retinacular vessels); anterior malposition injures the anterior retinacular vessels; superior or inferior malposition causes eccentric loading and early physeal closure.
Every screw thread must cross the physis into the epiphysis. If the smooth shank crosses the physis instead, there is no fixation of the epiphysis and the slip can progress. A partially threaded screw compresses the physis — the threads pull the epiphysis toward the metaphysis while the smooth shank slides through the cortex.
Each pass through the physis increases the risk of chondrolysis. Plan the trajectory, advance in small increments checking both views, hold the wire stable, and keep the tip 5mm from subchondral bone to avoid joint penetration.
The main blood supply to the femoral head, arising from the medial femoral circumflex artery and running along the posterior-superior femoral neck. Highest AVN risk if damaged by a posterior screw. Protect by verifying center-center on the lateral view and avoiding posterior cortex penetration.
Subchondral penetration causes chondrolysis (acute cartilage necrosis), presenting 2-12 months post-op with stiffness and joint-space narrowing. Protect by keeping the screw tip 5mm from subchondral bone on BOTH views.
Multiple passes increase trauma and chondrolysis risk; inadequate thread engagement allows continued slip. Protect with a single-pass technique, all threads across the physis, and a partially threaded screw for compression.
Emerges medial to the ASIS and supplies the anterolateral thigh; at risk with a lateral thigh incision. Protect by making the incision distal to the vastus ridge and using blunt dissection through muscle.
Aftercare & Complications
Immediate (24-48 hours). Regular neurovascular checks (femoral nerve palsy is rare and traction-related). Bed rest for an unstable SUFE to allow physeal stabilisation; mobilise the same day for a stable SUFE. Weight-bearing protocol. Touch weight-bearing with crutches for 6 weeks, progressing to full weight-bearing at 6 weeks if radiographs are stable. No running, jumping, or contact sports for 3-6 months. Follow-up schedule. | Timing | Assessment | |--------|------------| | 2 weeks | Wound check, x-ray both hips | | 6 weeks | X-ray; progress to full weight-bearing if stable | | 3 months | X-ray; expand activities | | Every 3-6 months | Until physeal closure (18-24 months) | | Annually | Until skeletal maturity | Screw removal. Performed 3-6 months AFTER complete physeal closure. Rationale: the femoral neck continues to grow in girth after physeal closure, so a retained screw tip progressively approaches and can enter the joint, causing chondrolysis. Technique: same positioning on the fracture table with biplanar fluoroscopy, percutaneous access over the screw head, unscrew and remove, then protected weight-bearing for 6 weeks if the screw is large or has been in situ a long time. Complications
- Recognition
- Pain and stiffness 6-12 months post-op; x-ray shows sclerosis, fragmentation, crescent sign, collapse; MRI is more sensitive for early detection
- Prevention
- Surgery within 24h for unstable SUFE; gentle positioning with no forceful reduction; center-center screw avoiding the posterior cortex; single-screw technique
- Management
- Protected weight-bearing, NSAIDs; core decompression is controversial; salvage by proximal femoral valgus osteotomy or arthroplasty if severe collapse
- Recognition
- Stiffness and pain 2-12 months post-op; loss of rotation and flexion; x-ray joint-space narrowing to less than 3mm (normal 4-7mm)
- Prevention
- Screw tip at least 5mm from subchondral bone on BOTH views; remove hardware if joint penetration is recognised; single-pass technique
- Management
- Remove a penetrating screw; physiotherapy maintaining ROM; NSAIDs, intra-articular steroid; most resolve over 12-24 months; 20-30% progress to early arthritis
- Recognition
- Intra-op: obvious on fluoroscopy. Post-op: groin pain, stiffness, clicking
- Prevention
- Biplanar fluoroscopy with the tip 5mm from subchondral on BOTH AP and lateral; measure length carefully; recheck after full seating
- Management
- Intra-op: remove and redirect. Post-op: urgent revision and monitor for chondrolysis
- Recognition
- New groin or thigh pain, limp, limited rotation of the other hip; x-ray shows a Klein line abnormality or physeal widening
- Prevention
- Prophylactic pinning if age less than 10, a metabolic cause, or unreliable follow-up; close surveillance every 3-6 months with bilateral imaging if not pinned
- Management
- Treat as a primary SUFE — classify and pin in situ; earlier detection means better outcomes
- Recognition
- Increasing Southwick angle on serial x-rays; pain and gait deterioration
- Prevention
- All threads across the physis; appropriate weight-bearing restrictions; serial radiographic monitoring
- Management
- Revise to a longer screw with better thread engagement; accept if near physeal closure
- Recognition
- Pain, clicking, loss of stability; x-ray shows the screw has backed out from its original position
- Prevention
- All threads must cross the physis; partially threaded screw for compression; weight-bearing restrictions
- Management
- Revise with a longer screw and better thread engagement; stricter weight-bearing restrictions
- Recognition
- Late teens to 30s: groin pain, limited flexion and internal rotation; positive impingement test; alpha angle greater than 55 degrees on x-ray/MRI
- Prevention
- Anatomic reduction if safe (modified Dunn for acute unstable severe); Imhauser osteotomy after physeal closure for chronic severe
- Management
- Conservative: activity modification, physio, NSAIDs. Surgical: hip arthroscopy (osteochondroplasty, labral repair) or open surgical dislocation; THA if advanced arthritis
- Recognition
- During or after screw removal; pain, deformity, inability to weight-bear
- Prevention
- Avoid excessive screw diameter; gentle technique during removal; consider protected weight-bearing for 6 weeks after removal
- Management
- ORIF with cannulated screws or DHS; non-weight-bearing 6-12 weeks; risk of AVN and nonunion
Viva & Exam Focus
SUFESUFE — risk factors and bilateral risk
Hook:20-40% develop bilateral SUFE — always image both hips at presentation and consider prophylactic pinning
CENTERCENTER — screw positioning principles
Hook:Posterior screw malposition risks injury to the posterior retinacular vessels — the main blood supply to the femoral head
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 13-year-old obese boy presents with 6 weeks of left groin and thigh pain. He walks with an antalgic gait and an externally rotated left leg. On examination he has limited hip internal rotation and obligate external rotation with hip flexion. How would you assess and manage this patient?”
“You are called to see a 12-year-old girl in ED who fell playing netball and now cannot weight-bear on her right hip. X-rays show a SUFE with a Southwick angle of 45 degrees. She has been in ED for 4 hours. How would you proceed?”
“A colleague asks your opinion on a 9-year-old boy with a mild unilateral SUFE (Southwick 25 degrees) who is stable and has no obvious endocrine cause. The parents want to know if prophylactic pinning of the other hip is necessary. What would you advise?”
Classification
- Loder: Stable (weight-bears) = less than 5% AVN; Unstable (cannot weight-bear) = 20-50% AVN
- Southwick (frog-lateral): Mild less than 30 degrees, Moderate 30-50 degrees, Severe greater than 50 degrees
- Temporal: Acute less than 3 weeks, Chronic greater than 3 weeks, Acute-on-chronic
- Klein line fails to intersect the lateral epiphysis on AP
Surgical principles
- Unstable SUFE = orthopaedic emergency, theatre within 24 hours
- In situ pinning — do NOT reduce a stable chronic slip
- Single central screw: center-center, perpendicular to physis, all threads across the physis
- Tip 5mm from subchondral bone on BOTH AP and lateral views
Critical danger zones
- Posterior retinacular vessels: main blood supply, highest AVN risk
- Subchondral bone: penetration causes chondrolysis
- Physis: multiple passes increase chondrolysis risk
- Posterior cortex penetration = AVN from retinacular vessel injury
Key complications
- AVN: 0.5-5% stable, 20-50% unstable — presents 6-12 months post-op
- Chondrolysis: 1-5% — joint stiffness, narrowing to less than 3mm
- Contralateral slip: 20-40% if not prophylactically pinned
- FAI: 30-70% (severity dependent) — late teens to 30s
Post-op protocol
- Touch weight-bearing with crutches for 6 weeks, then full if stable
- No running, jumping, or contact sports for 3-6 months
- Serial x-rays every 3-6 months until physeal closure (18-24 months)
- Screw removal 3-6 months after complete physeal closure
Prophylactic pinning
- Age less than 10 years (up to 60% bilateral risk)
- Hypothyroidism (50% bilateral), renal osteodystrophy (60% bilateral)
- Growth hormone deficiency, hypogonadism
- Unable to reliably follow up
Background & Evidence
Epidemiology. SUFE presents at a peak age of 10-16 years (boys 13-15, girls 11-13), with a male-to-female ratio of about 2:1; roughly 80% of affected children are obese (above the 95th percentile), and 20-40% are bilateral at presentation or on surveillance. US incidence is about 10.8 cases per 100,000 children aged 9-16 years, with a higher rate in black (3.94x) and Hispanic (2.53x) children than in white children. The bilateral risk is highest under age 10 and whenever an endocrine or metabolic cause is present. Pathoanatomy. The capital femoral epiphysis slips posteriorly and inferiorly relative to the metaphysis through the hypertrophic zone of the physis; because the epiphysis stays in the acetabulum, the limb externally rotates and the leg appears short and out-turned (the basis of the Drehmann sign). The femoral head is supplied by the retinacular vessels from the medial femoral circumflex artery running along the posterior-superior neck — the structure most at risk in unstable slips and in posterior screw malposition. Loder stability classification. Physeal stability (the ability to weight-bear) — not symptom duration — is the single most important prognostic factor for AVN and defines urgency.
- Definition
- Able to weight-bear, with or without crutches
- AVN risk
- Less than 5%
- Definition
- Unable to weight-bear at all
- AVN risk
- 20-50%
Southwick slip angle is measured on the frog-lateral as the difference between the affected and the normal side; it grades severity.
- Southwick angle
- Less than 30 degrees
- Notes
- Low AVN risk
- Southwick angle
- 30-50 degrees
- Notes
- Moderate risk
- Southwick angle
- Greater than 50 degrees
- Notes
- High risk; most still pin in situ
Temporal classification describes duration: acute (less than 3 weeks), chronic (greater than 3 weeks), or acute-on-chronic. On the AP view, the Klein line — a line drawn along the superior border of the femoral neck — normally intersects the lateral portion of the epiphysis; in SUFE it fails to do so, a quick screen that is pathognomonic when positive. Key evidence. Loder (1993) showed that physeal stability (weight-bearing ability) predicts AVN far better than symptom duration — the foundation of modern SUFE management. Aronsson (2006) established single-screw in situ fixation as the treatment of choice for stable SUFE. The modified Dunn capital realignment (Ziebarth 2009; Sankar 2013) can anatomically correct severe unstable deformity but carries a substantial osteonecrosis rate (about 26% in the multicentre series), which is why in situ pinning remains the default and the modified Dunn is reserved for experienced centres.
References
Acute slipped capital femoral epiphysis: the importance of physeal stability
- 55 hips reclassified by physeal stability (ability to weight-bear) rather than by symptom duration
- Avascular necrosis developed in 14 of 30 (47%) unstable hips versus 0 of 25 stable hips
- Satisfactory result in 96% of stable versus 47% of unstable hips
- No demonstrable association between early reduction and AVN
Slipped capital femoral epiphysis: current concepts
- Single-screw in situ fixation is the treatment of choice for stable SUFE, with high long-term success and minimal complications
- Posterior slip of the epiphysis is best appreciated on the lateral radiograph
- Unstable slips carry markedly higher complication risk and warrant urgent management
- Reported incidence ranges from 0.2 (Japan) to 10 per 100,000 internationally
The epidemiology of slipped capital femoral epiphysis: an update
- Overall US incidence 10.8 cases per 100,000 children aged 9-16 years
- Incidence 3.94x higher in black and 2.53x higher in Hispanic versus white children
- Higher in boys (13.35/100,000) than girls (8.07/100,000)
- Geographic, seasonal and racial variation imply both environmental and genetic contributors
The modified Dunn procedure for unstable slipped capital femoral epiphysis: a multicenter perspective
- 27 unstable hips treated with modified Dunn capital realignment, mean follow-up 22 months
- Osteonecrosis in 7 of 27 (26%); each of the 5 surgeons had at least one case
- Broken implants in 4 of 27 (15%) requiring revision fixation
- Mean final slip angle corrected to 6 degrees; AVN strongly predicted worse pain, satisfaction and function
Capital realignment for moderate and severe SCFE using a modified Dunn procedure
- 40 hips with moderate-to-severe SCFE treated via surgical dislocation and capital reorientation
- No patient developed osteonecrosis or chondrolysis at minimum 1-3 year follow-up
- Slip angle corrected to 4-8 degrees with mean post-correction alpha angle 40.6 degrees
- Articular cartilage damage and delamination frequently observed at surgery, especially in stable slips
Further reading 1. Southwick WO. Osteotomy through the lesser trochanter for slipped capital femoral epiphysis. J Bone Joint Surg Am. 1967;49(5):807-35. 2. Zaltz I, Baca G, Kim YJ, et al. Complications associated with the modified Dunn procedure for SCFE. J Pediatr Orthop. 2014;34(7):661-7. 3. Loder RT, Skopelja EN. The epidemiology and demographics of slipped capital femoral epiphysis. ISRN Orthop. 2011;2011:486512. 4. Imhäuser G. Late results of Imhäuser's osteotomy for slipped capital femoral epiphysis. Z Orthop Ihre Grenzgeb. 1977;115(5):716-25. 5. Kocher MS, Bishop JA, Weed B, et al. Delay in diagnosis of slipped capital femoral epiphysis. Pediatrics. 2004;113(4):e322-5.