Percutaneous Hoke triple hemisection, Vulpius V-Y gastrocnemius recession, or open Z-plasty for equinus contracture · Silfverskiold-guided selection
- Three distinct techniques target different anatomical levels: the Hoke triple hemisection (percutaneous, full tendon), the Vulpius V-Y recession (gastrocnemius aponeurosis only, spares soleus), and the open Z-plasty (full tendon, maximum lengthening 1–2 cm).
- The sural nerve runs 2–3 cm lateral to the Achilles tendon and must be identified and protected during open approaches; it is the structure at risk during the lateral hemisection of the Hoke technique.
- Over-lengthening is the most devastating complication — a permanent calcaneal or crouch gait with loss of push-off. Target dorsiflexion to neutral (0 degrees) with the knee extended, never beyond, and check the position after each cut.
- Tendo-Achilles lengthening is contraindicated in flaccid paralysis (polio, spinal cord injury) with an absent or weak triceps surae: lengthening an already powerless calf creates an irreversible calcaneal gait.
When & Why
Indication. Symptomatic equinus contracture that limits function and has failed non-operative management, where the underlying problem is overactivity or shortening of the gastrocnemius-soleus complex. Four clinical populations dominate:
Dynamic or fixed equinus limiting ambulation (GMFCS Levels I–III), having failed serial casting, botulinum toxin and physiotherapy. The Hoke triple hemisection is the workhorse. The Silfverskiold test decides whether a gastrocnemius-only release (Vulpius) is enough.
Residual or relapsed equinus after Ponseti casting, or equinus requiring correction for orthosis fitting. Open Z-plasty is preferred when precise, maximum lengthening is needed. Approximately 80 percent of idiopathic clubfeet need a percutaneous tendo-Achilles lengthening at the final Ponseti cast (Herzenberg, 2002).
Gastrocnemius-soleus tightness drives elevated forefoot plantar pressure and recurrent ulceration. Strong Level I evidence (Mueller, 2003) supports percutaneous TAL plus total contact casting. Indicated when passive dorsiflexion of 5 degrees or less accompanies a chronic or recurrent plantar forefoot ulcer.
An equinus component of the Charcot rocker-bottom foot adds instability. Open Z-plasty gives maximal, controlled lengthening and is usually combined with a midfoot osteotomy or fusion for comprehensive correction.
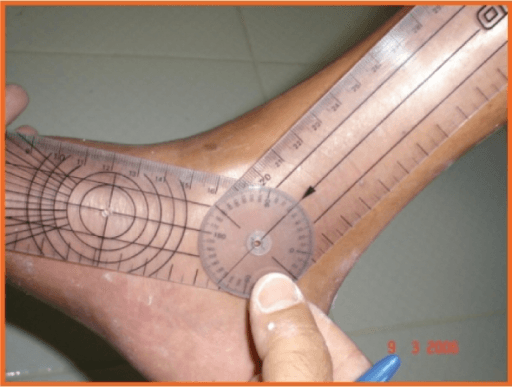
The Silfverskiold test decides the level. With the knee extended the gastrocnemius is tight; flexing the knee relaxes it. If the equinus corrects when the knee is flexed (a positive test), only the gastrocnemius is contracted and a gastrocnemius recession (Vulpius) is sufficient. If equinus persists with the knee flexed (a negative test), both gastrocnemius and soleus are contracted and a full-tendon lengthening (Hoke or Z-plasty) is required. DiGiovanni (2002) quantified this: knee-extended dorsiflexion averaged 4.5 degrees in symptomatic patients versus 13.1 degrees in controls, normalising when the knee was flexed.
- Anatomical level
- Full tendon (percutaneous)
- Silfverskiold
- Either — full-tendon
- Correction
- Moderate, about 10–15 degrees
- Typical use
- Spastic equinus — the workhorse
- Anatomical level
- Gastrocnemius aponeurosis only
- Silfverskiold
- Positive — gastrocnemius only
- Correction
- Moderate; spares soleus power
- Typical use
- Isolated gastrocnemius contracture
- Anatomical level
- Full tendon (open)
- Silfverskiold
- Negative — combined, or structural
- Correction
- Maximum, precise 1–2 cm
- Typical use
- Fixed structural equinus, clubfoot, Charcot
- Why
- Lengthening an already powerless calf creates an unresistable, irreversible calcaneal gait
- Why
- Further lengthening is catastrophic
- Why
- Absolute contraindication to elective surgery
- Why
- High wound-complication risk, especially across the watershed zone
- Why
- Healing and infection risk — optimise first or reconsider
Consent specifically for sural-nerve injury (lateral heel numbness or a painful neuroma), wound breakdown over the watershed zone (higher in diabetics), recurrence of equinus (about 20 percent in growing children with cerebral palsy), and over-lengthening into calcaneal gait — a permanent, disabling complication that is harder to treat than the original equinus. Setup. Prone with the ankle supported over a bolster so the foot can be passively dorsiflexed and plantarflexed freely to check correction intra-operatively. Mark the course of the sural nerve and the lateral border of the Achilles before skin preparation. A tourniquet is optional for the percutaneous Hoke and recommended for the open Vulpius and Z-plasty. General or spinal/regional anaesthesia; avoid local infiltration for open cases so post-operative wound vascularity can be assessed.
The Operation
The goal is to lengthen the gastrocnemius-soleus complex enough to restore a heel-toe gait and neutral dorsiflexion, at the anatomical level dictated by the Silfverskiold test, while protecting the sural nerve and never over-correcting. The relevant anatomy and all three techniques are laid out in the operative sequence below.

Anatomy that governs every step. The Achilles spirals about 90 degrees from proximal to distal: gastrocnemius fibres (about 75 percent of the tendon) run lateral proximally and rotate to insert medially and posteriorly, while soleus fibres (about 25 percent) lie anteriorly and insert centrally. The Hoke alternating medial/lateral/medial hemisections exploit this spiral so the tendon slides in a controlled fashion. The segment 2–6 cm above the calcaneal insertion is the avascular watershed zone (fed by the mesotenon from the posterior tibial artery) — the zone of greatest wound-healing risk, worse in diabetics. The sural nerve lies 2–3 cm lateral to the tendon throughout, and the thin plantaris (present in about 90 percent, 2–4 mm) runs medially. The broad gastrocnemius aponeurosis becomes a distinct layer separate from soleus 8–12 cm above the insertion — the level the Vulpius recession targets.
Operative sequence
- Prone with the ankle over a bolster so the foot moves freely; confirm you can dorsiflex and plantarflex without obstruction.
- Mark the lateral border of the Achilles and the course of the sural nerve before skin preparation.
- Tourniquet optional for Hoke; recommended for the open Vulpius and Z-plasty.
- Confirm the level of contracture with the knee extended and flexed, and confirm the planned technique.
- For Hoke, mark all three stab sites before any incision.
- Distal incision 2 cm above the insertion — medial hemisection.
- Middle incision 5 cm above the insertion — lateral hemisection (sural nerve at risk).
- Proximal incision 8 cm above the insertion — medial hemisection.
- Three cuts at roughly 3 cm intervals, each transecting half the tendon, alternating medial/lateral/medial.
- Stab incision with a No. 15 blade medially through the paratenon; advance the blade flat against the tendon, cutting the medial half only.
- Confirm by palpation that the lateral half remains intact.
- Stab incision laterally, transecting the lateral half of the tendon.
- Direct the blade with its flat surface toward the sural nerve (2–3 cm lateral); palpate that the medial half remains intact.
- Stab incision medially, transecting the medial half.
- Identify the thin medial plantaris cord and confirm the blade has engaged the main tendon bulk, not the plantaris alone.
- With all three cuts complete, slowly dorsiflex the ankle to neutral (0 degrees) with the knee extended.
- The tendon slides over the three levels, lengthening it; palpate that it remains a continuous cord.
- Never force dorsiflexion beyond neutral — over-lengthening is irreversible.
- Close the stab wounds with steri-strips or a single 3-0 nylon stitch.
- Below-knee cast with the ankle in neutral; weight-bearing as tolerated in most cases.
- Posterior midline incision 6–10 cm long, centred 8–12 cm above the insertion.
- Expose the gastrocnemius aponeurosis and identify the distinct layer where it overlies — but is separate from — the soleus.
- Mark an inverted-V with the apex pointing proximally, its base spanning the full width of the gastrocnemius aponeurosis.
- Cut the aponeurosis only and confirm soleus is visible and intact beneath; the V slides distally into a Y as the foot is dorsiflexed.
- Passively dorsiflex the ankle to neutral with the knee extended; the aponeurosis slides and the V closes into a Y — no suture repair is needed as the slide is self-stabilising.
- Close in layers; below-knee cast in neutral, non-weight-bearing for 4–6 weeks.
- Posteromedial incision 6–8 cm; identify and protect the sural nerve laterally.
- Incise the paratenon longitudinally and preserve it for later closure over the repair.
- Central longitudinal cut along the tendon for about 4 cm at the mid-tendon level; proximal horizontal limb toward medial, distal horizontal limb toward lateral, creating two overlapping flaps.
- Complete the Z cuts under direct vision, leaving the tendon in two flaps; place the ankle at the desired position (neutral with the knee extended).
- Overlap and suture the two flaps with heavy absorbable suture (No. 1-0 PDS or Vicryl) in a Bunnell or Kessler configuration.
- Tension is critical: too tight under-corrects, too loose over-lengthens; neutral dorsiflexion should need only gentle force.
- Close the paratenon over the repair — important for healing and vascularity — then close the skin in layers without tension.
- Below-knee cast in neutral with strict non-weight-bearing for 6 weeks; the fully divided tendon relies entirely on the repair.
Protect the sural nerve: it lies 2–3 cm lateral to the tendon and is most at risk at the lateral Hoke hemisection and during open dissection — keep the blade flat toward the nerve and identify it directly in open cases. Prevent over-lengthening: target neutral dorsiflexion (0 degrees) with the knee extended only, check the position after each cut, and never force dorsiflexion. Over-lengthening produces a permanent calcaneal or crouch gait that is far harder to correct than the original equinus, and is most common after percutaneous TAL in young diplegic children (up to 36 percent calcaneus in the Borton series).
A positive test (equinus corrects with knee flexion) means isolated gastrocnemius tightness — a Vulpius recession is enough and spares soleus power. A negative test (equinus persists with the knee flexed) means combined gastrocnemius-soleus contracture — a full-tendon Hoke or Z-plasty is required. Matching the level of lengthening to the level of contracture is the central principle of this operation.
Borton (2001) found percutaneous TAL in diplegia was the least predictable technique — only 38 percent satisfactory, with a high rate of calcaneus (over-lengthening). In young diplegic children, prefer an aponeurotic (Vulpius or Strayer) lengthening and reserve the percutaneous Hoke for clearly indicated cases.
Aftercare & Complications
Rehabilitation by technique | Technique | Immobilisation | Weight-bearing | Key milestone | |-----------|----------------|-----------------|---------------| | Hoke | Below-knee cast or boot in neutral | Weight-bearing as tolerated | Begin physiotherapy at 2–4 weeks | | Vulpius | Below-knee cast or boot in neutral | Non-weight-bearing 4–6 weeks | Aponeurosis must heal before loading | | Open Z-plasty | Below-knee cast in neutral | Strict non-weight-bearing 6 weeks | Transition to a boot at 6 weeks | Pain control is multimodal (paracetamol and NSAIDs) with strict elevation, as swelling over the tendon raises wound-healing risk. The first dressing change and wound review is at 10–14 days (10 days for diabetics). Physiotherapy from week 6 builds gastrocnemius-soleus strength (heel raises, single-leg balance, proprioception) and re-educates a heel-toe gait; running is held until 12 weeks and cutting or jumping sports until 16–20 weeks. Recovery by population. In spastic equinus (cerebral palsy, CVA) gait improvement is visible by 3 months with maximum benefit at 6–12 months alongside therapy; recurrence is common in growing children (about 20 percent recurrent equinus, Borton 2001) and may need a repeat procedure, while over-lengthening into calcaneus is also common (up to 36 percent in that series, highest after percutaneous TAL in young diplegics). In diabetic equinus the plantar-pressure benefit is immediate, wound healing is typically complete by 12–16 weeks, and a lifelong foot-care programme is essential. In clubfoot the Ponseti bracing protocol continues for 12 months; recurrence in idiopathic clubfoot runs 15–20 percent and depends on brace compliance. Complications
- Recognition
- Intra-operative dorsiflexion beyond neutral; post-operatively cannot push off or perform a single-leg heel rise; a heel-heavy slapping gait
- Prevention
- Target neutral (0 degrees) only; check after each cut; never force dorsiflexion; favour aponeurotic lengthening in young diplegics
- Management
- Physiotherapy and an AFO first; surgical reconstruction (Z-shortening or peroneus-brevis transfer) is technically demanding with poor, unpredictable results — prevention is essential
- Recognition
- Lateral heel numbness or paraesthesiae; a tender Tinel sign at the scar
- Prevention
- Identify and protect the nerve in open cases; at the lateral Hoke incision keep the blade flat toward the nerve
- Management
- Neuropraxia resolves in 6–12 weeks; transection — primary neurorrhaphy with 8-0 nylon; a persistent neuroma — excision and proximal burial in muscle
- Recognition
- Dehiscence or skin-edge necrosis over the watershed zone; exposed paratenon or tendon
- Prevention
- Handle skin with hooks not forceps; close the paratenon as a separate layer; offset the incision off the tendon; optimise HbA1c
- Management
- Local wound care and dressings for minor breakdown; VAC for moderate; a plastic-surgery flap for exposed tendon; debridement and IV antibiotics if infected
- Recognition
- Sudden pain with a palpable defect; cannot plantar-flex against gravity; positive Thompson (Simmonds) squeeze test
- Prevention
- Strict non-weight-bearing 6 weeks after Z-plasty; a strong No. 1-0 repair; avoid early aggressive physiotherapy
- Management
- Acute (under 6 weeks): re-exploration and repair; delayed: reconstruction with transfer or allograft; non-operative (unfit): equinus cast then an AFO
- Recognition
- Persistent equinus post-operatively; toe-only foot strike; a Hoke cut that failed to slide from an incomplete hemisection
- Prevention
- Confirm each Hoke cut engages a full half-circumference; verify neutral dorsiflexion before casting
- Management
- Mild: serial casting and physiotherapy; significant: repeat TAL or upgrade to open Z-plasty; address any spasticity contributing
Diabetic patients — special considerations. Optimise pre-operatively (HbA1c under 8 percent, check the ABPI and vascular status). Use a total contact cast rather than a boot post-operatively to reduce inadvertent weight-bearing in the neuropathic limb, with a mandatory wound check at 2 weeks and twice-weekly monitoring for at-risk feet. If peripheral vascular disease is present, obtain a vascular opinion before elective TAL. Diabetic foot management is never single-surgeon — coordinate with podiatry, vascular surgery, orthotics and the diabetic foot team.
Viva & Exam Focus
HVZHVZ — three techniques in order of power
SCANSCAN — contraindications to tendo-Achilles lengthening
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 7-year-old with spastic diplegic cerebral palsy (GMFCS Level II) has progressive bilateral equinus. Botulinum toxin was effective for 2 years but now gives less than 3 months of benefit. Examination shows 20 degrees of fixed equinus bilaterally with the knee extended, correcting to 5 degrees equinus with the knee flexed. His gait video shows toe-walking. What is your surgical plan?”
“A 58-year-old diabetic man has a recurrent plantar first metatarsal head ulcer (Wagner Grade 2). Total contact casting has healed the ulcer three times but it has recurred each time. His HbA1c is 7.4 percent, ABPI 1.1, and examination shows 10 degrees of fixed equinus with the knee extended. What is the role of TAL and how would you perform it?”
“A patient returns 3 months after a Hoke TAL for spastic equinus with a new gait problem. Instead of toe-walking they now have a flat-footed slapping gait with the heel hitting the ground hard and the forefoot elevated in early stance. They complain of calf weakness and cannot perform a single-leg heel rise. What has happened and how do you manage it?”
Three techniques — know when to choose
- Hoke triple hemisection (percutaneous): workhorse for spastic equinus (CP, CVA, TBI); three stab incisions alternating medial/lateral/medial; about 10–15 degrees of correction
- Vulpius V-Y recession: a positive Silfverskiold (equinus corrects with knee flexion) means isolated gastrocnemius; cuts the gastrocnemius aponeurosis only and spares soleus power
- Open Z-plasty: fixed structural equinus (clubfoot relapse, Charcot, myelomeningocele); maximum lengthening 1–2 cm; full-tendon division and suture repair; strict non-weight-bearing 6 weeks
- The Silfverskiold test is the key selector: positive = Vulpius adequate; negative (persists with knee flexed) = full-tendon TAL required
Critical anatomy
- Sural nerve: 2–3 cm lateral to the Achilles; at risk at the lateral (middle) Hoke incision; protect by directing the blade medially with its flat surface toward the nerve
- Plantaris: medial to the Achilles, a thin 2–4 mm cord, present in about 90 percent; do not mistake it for the Achilles at the proximal medial incision
- Tendon spiral: gastrocnemius (about 75 percent) lateral-to-medial; soleus (about 25 percent) anterior; alternating cuts exploit the spiral for controlled sliding
- Watershed zone: 2–6 cm above the insertion is most avascular — the highest wound-breakdown risk, critical in diabetics
Hoke technique — step by step
- Mark three levels: distal 2 cm (medial), middle 5 cm (lateral), proximal 8 cm (medial) above the insertion
- Each stab incision cuts half the tendon circumference only; confirm the intact contralateral half by palpation
- Middle lateral incision: direct the blade medially, flat surface toward the sural nerve (2–3 cm lateral)
- Proximal medial incision: identify and avoid the medial plantaris cord; confirm the blade is in the main tendon bulk
- After all three cuts: slowly dorsiflex to neutral (0 degrees) only; feel the tendon slide, do not force
- Palpate a continuous tendon cord throughout — confirming interdigitation rather than rupture
Over-lengthening — the critical complication
- Result: calcaneal or crouch gait — prominent heel strike, forefoot elevation in stance, absent push-off, cannot perform a heel rise
- Mechanism: the tendon is too long for effective plantar flexion and operates on a flat length-tension curve
- Prevention: target neutral (0 degrees) only; check after each Hoke cut before the next; never force dorsiflexion
- Management: physiotherapy and an AFO first; surgical reconstruction (Z-shortening, tendon transfer) has poor outcomes
- Counsel pre-operatively: over-lengthening (5–10 percent with Hoke; up to 36 percent calcaneus in CP) is a permanent disability worse than the original equinus
Diabetic equinus — key evidence
- Mueller RCT (2003, JBJS Am): percutaneous TAL plus TCC versus TCC alone; recurrence 15 percent versus 59 percent at 7 months (p=0.001) and 38 percent versus 81 percent at 2 years (p=0.002)
- Indication: equinus contracture (5 degrees or less passive dorsiflexion, knee extended) with a recurrent or chronic diabetic forefoot ulcer
- Preferred technique: Hoke percutaneous — avoids an open wound in a high wound-healing-risk diabetic patient
- Post-op: a total contact cast is preferred over a boot to prevent inadvertent weight-bearing in the neuropathic limb
- MDT essential: podiatry, vascular, orthotics and the diabetic foot team — never single-surgeon management
Contraindications — never perform TAL in
- Flaccid paralysis or absent triceps surae (polio, spinal cord injury, peripheral nerve palsy) — creates irreversible calcaneal gait
- Pre-existing calcaneal gait or calcaneovalgus — further lengthening is catastrophic
- Active local infection — absolute contraindication
- Critical limb ischaemia (ABPI under 0.5) — adequate perfusion is mandatory for healing
Post-operative immobilisation by technique
- Hoke: below-knee cast or boot in neutral; weight-bearing as tolerated in most patients
- Vulpius: non-weight-bearing cast for 4–6 weeks; the aponeurosis must heal before loading
- Z-plasty: strict non-weight-bearing cast for 6 weeks; the full-tendon repair needs complete protection
- Diabetic patients: a total contact cast is preferred regardless of technique; wound review is mandatory at 10 days
- Cerebral palsy: a post-operative AFO programme reduces spastic recurrence; annual review for recurrence during growth
High-yield exam tips
- Always cite the Silfverskiold test — it distinguishes gastrocnemius-only from combined contracture and drives technique selection
- The Mueller RCT is mandatory knowledge — know recurrence 59 percent to 15 percent at 7 months and 81 percent to 38 percent at 2 years
- Over-lengthening equals calcaneal gait equals permanent disability — show you understand it is worse than under-correction
- Sural nerve at the lateral incision and plantaris at the proximal incision are the two most commonly examined danger-zone facts
- Flaccid paralysis is an absolute contraindication — a completely different situation to spastic equinus
- Both the diabetic foot and cerebral-palsy equinus require multidisciplinary management; examiners test systems thinking
Background & Evidence
Why equinus matters, by population. In cerebral palsy, overactivity and shortening of the gastrocnemius-soleus produce a dynamic and then fixed equinus that drives a toe-walking gait, limits community ambulation (GMFCS I–III) and impairs brace fit; botulinum toxin, serial casting and therapy are tried first, with surgery reserved for fixed contracture. In the diabetic foot, isolated gastrocnemius or combined equinus increases plantar-flexor moment and peak forefoot pressure, contributing to neuropathic ulceration and recurrence; correcting the equinus offloads the forefoot at its mechanical source. In clubfoot, residual equinus after Ponseti casting (a TAL is performed at the final cast in about 80 percent of idiopathic feet, Herzenberg 2002) and in Charcot rocker-bottom deformity both need structural correction, where the open Z-plasty gives precise, maximum lengthening. The shared principle — established classically by Sharrard and Bernstein (1972), who compared tendo-calcaneus elongation with gastrocnemius recession in cerebral palsy — is to match the level of lengthening to the level of contracture. The landmark evidence. Three studies anchor modern practice. Mueller and colleagues (2003) provided the Level I evidence that percutaneous TAL plus total contact casting cuts diabetic forefoot ulcer recurrence from 59 percent to 15 percent at 7 months and from 81 percent to 38 percent at 2 years — frequently and incorrectly attributed to Armstrong, whose 1999 paper was a 10-patient gait-laboratory study showing peak forefoot pressure fell from 86 to 63 N/cm² and dorsiflexion rose from 0 to 9 degrees (the biomechanical rationale the RCT later proved). DiGiovanni and colleagues (2002) quantified isolated gastrocnemius tightness (knee-extended dorsiflexion 4.5 versus 13.1 degrees in controls, normalising with the knee flexed), validating the knee-position-dependent examination that selects patients for a gastrocnemius-only recession. Borton and colleagues (2001) analysed 195 calf-lengthening procedures in 134 children with cerebral palsy and showed that over-lengthening into calcaneus is common (36 percent) and that percutaneous TAL in diplegia is the least predictable (38 percent satisfactory) — the evidence to prefer aponeurotic lengthening in young diplegics.
- Design
- RCT, 64 diabetic patients
- Key result
- Ulcer recurrence 15 percent versus 59 percent at 7 months (p=0.001); 38 percent versus 81 percent at 2 years (p=0.002)
- What it changes
- Level I basis for percutaneous TAL plus total contact casting in the diabetic foot
- Design
- Prospective gait study, 10 patients
- Key result
- Peak forefoot pressure 86 to 63 N/cm²; dorsiflexion 0 to 9 degrees
- What it changes
- Biomechanical rationale — not the RCT, despite common misattribution
- Design
- Case-control, 34 versus 34
- Key result
- Knee-extended dorsiflexion 4.5 versus 13.1 degrees; normalises with knee flexed
- What it changes
- Validates the Silfverskiold-guided choice of a gastrocnemius-only recession
- Design
- Case series, 195 procedures in 134 children with CP
- Key result
- 36 percent calcaneus (over-lengthening); percutaneous TAL in diplegia only 38 percent satisfactory
- What it changes
- Prefer aponeurotic lengthening in young diplegics; over-lengthening is common
References
Effect of Achilles tendon lengthening on neuropathic plantar ulcers: a randomized clinical trial
- 64 diabetic patients with a neuropathic forefoot ulcer and dorsiflexion of 5 degrees or less, randomised to total contact casting alone versus casting plus percutaneous TAL
- Ulcer recurrence at 7 months: 15 percent (TAL) versus 59 percent (casting alone), p=0.001
- Recurrence at 2 years: 38 percent (TAL) versus 81 percent (casting alone), p=0.002 — a 52 percent relative risk reduction
- All TAL ulcers healed; dorsiflexion increased and peak forefoot pressure decreased after TAL
Lengthening of the Achilles tendon in diabetic patients who are at high risk for ulceration of the foot
- Prospective repeated-measures gait study in 10 diabetic patients with prior neuropathic forefoot ulceration (not a randomised trial)
- Peak forefoot plantar pressure fell from 86 to 63 N/cm² eight weeks after percutaneous TAL, p less than 0.001
- Ankle dorsiflexion increased from 0 to 9 degrees, p less than 0.001
Isolated calf lengthening in cerebral palsy: outcome analysis of risk factors
- 195 isolated calf-lengthening procedures (percutaneous TAL, open Z-lengthening, gastrosoleus aponeurotic) in 134 children with cerebral palsy
- At medium-term follow-up: 42 percent satisfactory, 22 percent recurrent equinus, 36 percent calcaneus (over-lengthening)
- Percutaneous TAL in diplegia was least predictable (38 percent satisfactory); risk factors for calcaneus were severe involvement, female sex, surgery before age 8, and percutaneous TAL
Isolated gastrocnemius tightness
- Prospective case-control study (34 patients with forefoot or midfoot pain versus 34 controls) using an electrogoniometer
- Knee-extended dorsiflexion averaged 4.5 degrees in patients versus 13.1 degrees in controls, p less than 0.001
- With the knee flexed 90 degrees the difference disappeared (17.9 versus 22.3 degrees, p=0.09), confirming isolated gastrocnemius tightness
Equinus deformity in cerebral palsy: a comparison between elongation of the tendo calcaneus and gastrocnemius recession
- Comparative study of full tendo calcaneus elongation versus gastrocnemius recession for spastic equinus in cerebral palsy
- Full-tendon lengthening carried a higher rate of over-correction (calcaneus) and recurrence than selective gastrocnemius recession
- Established the principle of matching the level of lengthening to the level of contracture
Foundational technique references 1. Hoke M. An operation for the correction of extremely relaxed flat feet. J Bone Joint Surg Am. 1931;13:773–783. Original description of the triple-hemisection percutaneous technique — the most widely used tendo-Achilles lengthening worldwide. 2. Vulpius O, Stoffel A. Orthopaedische Operationslehre. Stuttgart: Ferdinand Enke; 1913. Original description of the inverted-V (V-Y) aponeurotic gastrocnemius lengthening for equinus deformity. 3. Silfverskiold N. Reduction of the uncrossed two-joints muscles of the leg to one-joint muscles in spastic conditions. Acta Chir Scand. 1923–1924;56:315–330. Original description of the clinical test distinguishing isolated gastrocnemius from combined gastrocnemius-soleus contracture. 4. Herzenberg JE, Radler C, Bor N. Ponseti versus traditional methods of casting for idiopathic clubfoot. J Pediatr Orthop. 2002;22(4):517–521. Evidence supporting the Ponseti casting protocol including percutaneous TAL at the final casting stage; approximately 80 percent of idiopathic clubfeet require a TAL. 5. Rosenthal RK. The use of orthotics in foot and ankle problems in cerebral palsy. Foot Ankle. 1984;4(4):195–200. Foundational reference on the relationship between equinus management and orthotic outcomes in cerebral palsy, establishing the role of TAL within a comprehensive programme.