Fusion of the thumb MCP joint for painful arthritis, chronic instability, post-traumatic destruction or rheumatoid Z-collapse | advanced
- Functional fusion position: 10-15 degrees of MCP flexion with slight pronation (radial deviation) — this optimises pulp-to-pulp pinch strength by approximating the thumb and index finger pads in the neutral rotation plane.
- The thumb MCP joint sacrifices only 5-10 degrees of useful flexion in the fusion; the dominant thumb motion comes from the CMC joint (opposition, circumduction) and the IP joint (flexion for tip pinch). Fusion of the MCP stabilises the column without eliminating the key arcs above and below.
- Nonunion is the principal failure mode (reported 5-15% across series) — meticulous preparation of flat, bleeding cancellous surfaces on both sides of the joint with stable compression fixation and at least 4-6 weeks of protected immobilisation are the foundations of union.
- The dorsal approach runs between the extensor pollicis brevis (EPB) and extensor pollicis longus (EPL) — the radial digital nerve crosses the operative field in the proximal wound and must be identified and protected before deepening the dissection.
- “The ulnar collateral ligament of the thumb MCP is the primary restraint to valgus stress during pinch — chronic insufficiency leads to a progressive volar subluxation of the proximal phalanx and pinch instability. Fusion is the salvage when reconstruction has failed or the ligament remnants are non-reconstructable.
- “In rheumatoid disease the MCP is the middle link of the Z-collapse: CMC dorsoradial subluxation plus MCP volar subluxation plus IP hyperextension produces the zigzag collapse pattern. Fusion of the MCP stabilises the middle link and is often combined with CMC arthroplasty and IP joint soft-tissue balancing.
- “Headless compression screws (Acutrak or Herbert-type) provide excellent compression and avoid dorsal hardware prominence — but they demand good bone stock and accurate trajectory. In osteoporotic rheumatoid bone, a dorsal mini-plate or tension band wiring may be more reliable.
- “Post-operative immobilisation in a thumb spica cast or splint for 4-6 weeks is standard. Immobilisation beyond 8 weeks increases stiffness and does not improve union rates. Early protected IP and CMC motion within the thumb spica is encouraged.
When & Why
A salvage operation that trades a little motion for a stable, painless column. Thumb MCP arthrodesis eliminates pain at the MCP and converts an unstable link into a rigid strut, at the cost of only the small MCP flexion arc (the CMC and IP provide the dominant thumb motion). It is reserved for situations where motion-preserving options have failed or are not viable. Absolute indications - Chronic ulnar collateral ligament (UCL) insufficiency not amenable to reconstruction — gross instability with volar subluxation during pinch, a failed prior UCL repair, or a failed graft reconstruction.
- Post-traumatic MCP joint destruction with combined arthritis and instability where motion-preserving procedures (arthroplasty, osteotomy) are not viable.
- Rheumatoid Z-collapse deformity with painful MCP volar subluxation as part of the zigzag collapse pattern — fusion stabilises the middle link of the collapse. Relative indications - Primary MCP osteoarthritis (uncommon in isolation — more often part of pan-trapezial arthritis) causing pain and functional loss refractory to non-operative treatment for greater than 6 months.
- MCP instability after infection or tumour resection where joint reconstruction is not possible.
- Failed MCP arthroplasty (silicone or pyrocarbon) with painful instability or loosening — revision to fusion.
- Salvage after failed external fixation or failed dynamic external fixation for complex MCP peri-articular fractures. Contraindications. Absolute: active infection at or adjacent to the MCP joint; an uncorrectable soft-tissue deficit precluding wound closure over the fixation hardware. Relative: symptomatic CMC arthritis that should be addressed first (staged before MCP fusion or simultaneously); pre-existing IP joint arthritis (fusion at MCP may overload the IP — consider whether IP fusion alone would suffice); and a patient whose occupation requires a full MCP flexion arc (some musicians, specialised manual workers) who should be counselled thoroughly. Try non-operative treatment first. A resting thumb spica splint reduces MCP loading and gives symptomatic relief in early disease; static splinting at 10-15 degrees of flexion can reduce pain during activities of daily living. The evidence is largely case series and expert opinion — no RCTs specifically compare splinting with surgery for MCP arthritis. An intra-articular corticosteroid injection gives temporary relief (weeks to months), mainly in inflammatory arthritis; in primary OA the small capsule makes injection inconsistent, though it can serve as a diagnostic test confirming the MCP as the pain source before committing to surgery. Arthroplasty or arthrodesis? MCP arthroplasty (silicone, pyrocarbon, or interposition) is an option for patients who wish to retain MCP motion, but silicone implants carry synovitis, implant fracture and subsidence over time, and pyrocarbon and resurfacing implants have shorter follow-up and higher revision rates than fusion. Arthrodesis gives a predictable, permanent and painless solution at the cost of MCP motion, and the bulk of evidence supports fusion as the gold standard for young, active, high-demand patients. Key decision points - Young, active patient with good bone stock and UCL insufficiency — headless compression screw: the best balance of compression, low profile and no routine hardware removal.
- Rheumatoid patient with osteoporotic bone — dorsal mini-plate: the most rigid fixation in poor-quality bone; accept the higher rate of hardware removal.
- Low-resource or cost-sensitive setting — tension band wiring with K-wires: reliable and inexpensive; plan for hardware removal at 4-6 weeks.
- Concomitant CMC disease — address the CMC first (trapeziectomy and LRTI), then reassess the MCP; some patients no longer need MCP fusion after CMC stabilisation.
- IP joint arthritis present — if mild, proceed with MCP fusion and monitor the IP; if severe, consider IP fusion alone (which eliminates tip pinch) or staged procedures. Consent specifically for nonunion (5-15%), malposition requiring revision, hardware prominence and possible removal (10-20% with a plate), infection (less than 1%), IP joint overload, CMC overload, and the certainty of permanent loss of MCP motion.
The Operation
The goal is to expose the joint through the dorsal approach, protect the radial digital nerve, prepare two flat bleeding cancellous surfaces, fix the joint at 10-15 degrees of flexion with slight pronation, and splint the thumb in the functional position. The dorsal exposure between EPB and EPL — with the radial digital nerve identified and protected — is the heart of the operation and is laid out step by step below.
Operative sequence
- Supine, arm abducted 90 degrees on a hand table, forearm in full supination. A forearm tourniquet at 200-250 mmHg is applied but may not need inflation if WALANT is used.
- Anaesthesia: general, regional (brachial plexus block), or WALANT. WALANT lets you check pinch position before committing to fixation — inject 3-5 mL of 1% lidocaine with 1:100,000 epinephrine along the planned incision 15-20 minutes beforehand.
- Exsanguinate with an Esmarch bandage; limit total tourniquet time to less than 90 minutes.
- Position the mini C-arm for AP and lateral thumb MCP views without moving the hand; drape the intensifier and confirm the screen is visible.
- Loupe magnification (2.5x minimum); confirm the headless screw, plate, or tension-band set is available before draping.
- Palpate the metacarpal head and the MCP flexion crease to mark the joint (the crease lies slightly distal to the joint itself).
- Mark a longitudinal or gently curving dorsal incision centred on the MCP, about 3-4 cm long, running from the proximal phalanx mid-shaft to the distal metacarpal shaft.
- Plan the incision slightly ulnar to the midline — this avoids the radial digital nerve, which crosses into the dorsal field proximally.
- An incision that is too short limits exposure for plate placement and joint preparation.
- Incise skin sharply with a number 15 blade and elevate thin skin flaps carefully in the subcutaneous plane.
- Identify the radial digital nerve in the proximal fat pad — a small white cord running from volar to dorsal — and protect it with a vessel loop before deepening the dissection. This is the single most important structure to protect in this approach.
- Do not confuse it with a small dorsal sensory branch: the digital nerve is larger and runs a predictable volar-to-dorsal course.
- Avoid excessive skin-flap elevation, which devascularises the thin dorsal skin.
- Identify EPB (radial) and EPL (ulnar) proximal to the MCP joint. Confirm EPB by traction — it inserts on the proximal phalanx base, whereas APL inserts on the metacarpal base.
- Develop the interval between EPB and EPL sharply; retract EPB radially and EPL ulnarly. This interval opens directly onto the MCP capsule.
- This dorsal interval keeps you away from the volar neurovascular structures and is the standard approach for MCP fusion.
- Make a longitudinal capsular incision in the midline from proximal to distal, with small releasing incisions at the corners for exposure.
- Preserve as much capsule as possible for later closure over the fusion site.
- Flex and extend the MCP to visualise the full articular surface.
- Resect the metacarpal head articular surface to flat, bleeding cancellous bone with a small oscillating saw, flat osteotome or burr; resect the proximal phalanx base to match.
- Resect until you see punctate bleeding from cancellous bone — if the surface is still sclerotic, take more. Good bleeding bone is the foundation of union.
- Aim for two flat, parallel surfaces with maximal cancellous contact; a cup-and-cone (convex metacarpal, concave phalanx) or fish-mouth (step-cut) configuration increases contact area but needs more precision.
- Avoid excessive resection, which shortens the thumb and weakens pinch, and avoid eccentric resection, which produces malalignment.
- Hold the provisional reduction with a single 1.0 mm K-wire at 10-15 degrees of MCP flexion with slight pronation.
- Check clinically: the thumb pulp should approximate the index finger pad in a comfortable pinch posture; the thumb should be neither hyperextended nor over-flexed.
- Confirm the alignment on AP and lateral fluoroscopy and adjust the K-wire until both clinical and radiographic alignment are satisfactory before any definitive fixation.
- Headless compression screw (good bone stock): from the dorsal cortex of the proximal phalanx base, drive a guide wire across the fusion site into the metacarpal shaft; confirm trajectory on fluoroscopy, measure, overdrill the near cortex, and seat an Acutrak mini or Herbert-type screw for compression.
- Dorsal mini-plate (osteoporotic or rheumatoid bone): a 2.0 or 2.4 mm T-plate or straight plate (4-6 holes) contoured to the dorsal metacarpal neck and proximal phalanx base, fixed with 2-3 screws each side, placed just ulnar to the EPL to reduce tendon irritation; apply compression through the plate or with a separate lag screw.
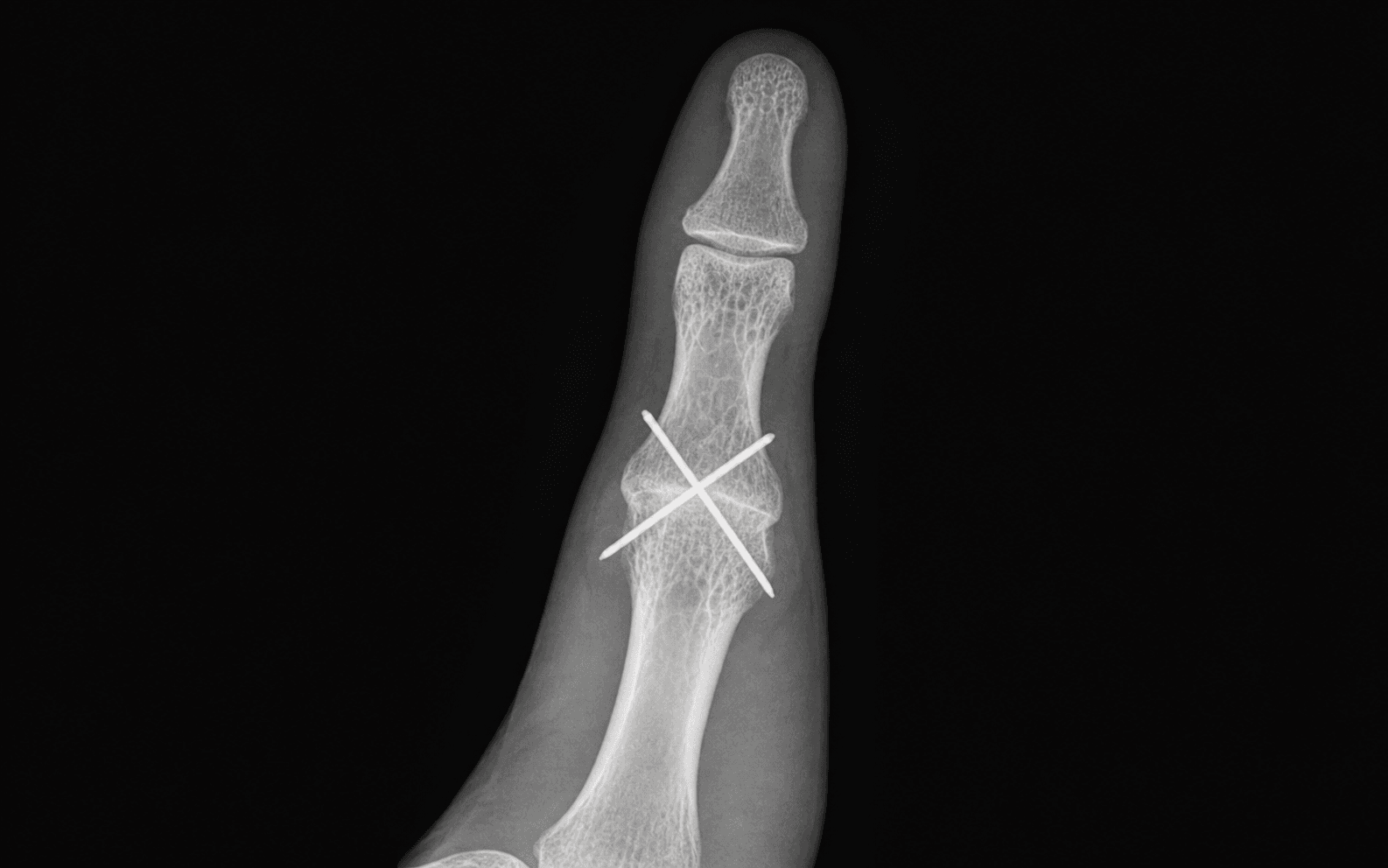
- Tension band wiring (low cost): two parallel 1.0-1.2 mm K-wires across the fusion plus a 0.8-1.0 mm cerclage wire in a figure-of-eight over the K-wire ends and through a transverse drill hole distal to the fusion, tightened to generate compression; bend and bury the K-wire ends.
- Check fixation stability by gentle manual stressing; take final AP and lateral fluoroscopic images to confirm position, alignment and hardware.
- If a bone defect remains after resection, pack morsellised autograft from the resected articular fragments into the gap before final compression.
- Irrigate thoroughly; close the joint capsule with 3-0 or 4-0 absorbable suture and repair the extensor interval between EPB and EPL if needed.
- Close subcutaneous tissue with 4-0 absorbable sutures and skin with 4-0 non-absorbable interrupted sutures.
- Apply a well-padded thumb spica splint or short-arm thumb spica cast with the MCP in the fusion position, the IP free, and the wrist in neutral — the plaster must not extend beyond the IP joint so IP motion can begin immediately.
The radial digital nerve of the thumb runs in the volar subcutaneous tissue and crosses into the dorsal wound in the proximal portion of the incision, lying superficial to the extensor tendons. Identify it in the proximal fat pad and protect it with a vessel loop before deepening the dissection between EPB and EPL. A transection produces a painful neuroma and loss of radial pulp sensibility. If it is injured intra-operatively, repair it primarily under loupe magnification.
Fusing the MCP straight or hyperextended eliminates effective pulp-to-pulp pinch because the thumb tip cannot reach the index pad; fusing in excessive flexion (greater than 20 degrees) shortens the pinch distance and weakens grip. The correct position is 10-15 degrees of flexion with slight pronation. Use a temporary K-wire to hold it, then check pinch against the contralateral hand before committing to the screw or plate, and confirm the angle on fluoroscopy.
In a young patient with good bone, a headless compression screw gives excellent compression, sits within the bone, and avoids hardware removal. In rheumatoid or osteoporotic bone, switch to a dorsal mini-plate — the most rigid construct and the highest union rate — contouring it to sit just ulnar to the EPL to reduce tendon irritation. For a low-resource or cost-sensitive setting, tension band wiring is reliable and inexpensive, with planned hardware removal at 4-6 weeks.
Inadequate removal of sclerotic subchondral bone leaves two hard, avascular surfaces that cannot consolidate — the commonest cause of nonunion. Resect both the metacarpal head and the proximal phalanx base down to punctate bleeding cancellous bone, maximise contact area with flat or cup-and-cone surfaces, and apply stable compression. Smoking, diabetes and rheumatoid osteopenia are the most consistent patient-side risk factors — optimise them pre-operatively.
- Union rate
- 90-97%
- Advantages
- Compression across the fusion site; no hardware removal in most cases; low profile; good bone-to-bone contact
- Disadvantages
- Demands good bone stock; technically demanding trajectory; difficult to revise if malpositioned; cost
- Union rate
- 95-100%
- Advantages
- Most rigid fixation; highest union rate; allows early mobilisation if bone quality permits; can correct malalignment
- Disadvantages
- Hardware prominence requiring removal (10-20%); EPL irritation; most expensive; bulk under thin dorsal skin
- Union rate
- 85-95%
- Advantages
- Low cost; familiar technique; good compression; hardware removed at 4-6 weeks
- Disadvantages
- K-wire migration and infection risk; requires hardware removal; less rigid than a plate; wire breakage possible
- Union rate
- 80-90%
- Advantages
- Simple; low cost; no plate prominence
- Disadvantages
- Least rigid fixation; no compression across the fusion site; higher nonunion rate; does not control rotation well
Aftercare & Complications
Rehabilitation | Phase | Timing | Immobilisation | Therapy | |-------|--------|----------------|---------| | 1 | 0-4 weeks | Thumb spica cast/splint, MCP in the fusion position, IP free | Active IP flexion/extension from day 1; gentle CMC opposition within the cast; elevation for 48 hours | | 2 | 4-6 weeks | Removable thumb spica splint (after 4-week X-ray shows early bridging) | Gentle IP and CMC motion; light lateral and pulp pinch; scar massage from 6 weeks | | 3 | 6-8 weeks | Splint for heavy tasks only | Progressive pinch and grip strengthening with therapy putty; splint weaning | | 4 | 8-12 weeks | Night splint only | Full activity; non-contact sport; contact sport and heavy manual work at 3-4 months | Sutures are removed at 10-14 days. Radiographs are taken at 4 and 8 weeks to track bridging trabeculae across the fusion site. Most patients return to desk work by 8-12 weeks and heavy manual work by 3-4 months, and driving once they can comfortably grip the wheel and perform an emergency stop (usually 6-8 weeks). If a plate was used, discuss planned removal after confirmed union at 4-6 months. Key rehabilitation principle — IP motion from day 1. The IP joint compensates for the lost MCP arc and must stay supple; a stiff IP after MCP fusion is a poor functional result. Encourage gentle CMC opposition even during immobilisation, and retrain pinch with a hand therapist, since the thumb now works as a single unit from CMC to IP with the MCP fixed. Expected outcomes. Union is achieved in 85-95% across all fixation methods (highest with a plate, lowest with K-wires alone), typically over 8-14 weeks (longer in smokers, diabetics and rheumatoid bone). Pain relief is reported by 85-95%, patient satisfaction by 80-95%, and grip and pinch strength are maintained or improved — particularly where instability was the pre-operative problem. Complications
- Incidence
- 5-15%
- Recognition
- Persistent pain at the fusion site 3-4 months post-operatively; no bridging trabeculae on serial radiographs; hardware loosening or breakage; palpable motion
- Prevention and management
- Prevention: meticulous resection to bleeding cancellous bone; stable compression fixation; 4-6 weeks protected immobilisation; smoking cessation and diabetic optimisation. Management: continue immobilisation if early with no hardware failure (some delayed unions consolidate by 6 months); revision fixation with bone graft for established nonunion
- Incidence
- 3-8%
- Recognition
- Thumb in a poor pinch position — the tip cannot reach the index pad; fusion angle excessive (extension or flexion) or in wrong rotation
- Prevention and management
- Prevention: temporary K-wire and clinical pinch check before definitive fixation; fluoroscopy before final hardware. Management: early revision with osteotomy of the fusion mass and re-fixation in the correct position; delays beyond 3 months may need bone graft
- Incidence
- 5-20% (plate highest)
- Recognition
- Painful dorsal bump; EPL tendon irritation or triggering; skin breakdown over the plate
- Prevention and management
- Prevention: headless screw when bone allows; contour the plate and place it ulnar to the EPL. Management: hardware removal once union is confirmed (usually 4-6 months); warn the patient pre-operatively
- Incidence
- less than 1% (deep)
- Recognition
- Erythema, warmth, swelling, wound discharge; fever; deep infection may present as hardware loosening or a draining sinus
- Prevention and management
- Prevention: sterile technique; perioperative antibiotics; haemostasis; careful soft-tissue handling. Management: superficial — oral antibiotics and wound care; deep — surgical washout, debridement and culture-directed IV antibiotics; hardware removal only if infection persists
- Incidence
- 5-10% (progressive)
- Recognition
- Progressive IP joint pain and stiffness after MCP fusion; loss of IP flexion; radiographic IP joint-space narrowing
- Prevention and management
- Prevention: screen for pre-existing IP arthritis and counsel the patient; avoid forceful tip-pinch loading early. Management: non-operative (splinting, injection, activity modification); IP fusion if severe and refractory
- Incidence
- Variable (common if pre-existing disease)
- Recognition
- Basal thumb pain after MCP fusion; positive grind test; radiographic CMC joint-space narrowing or subluxation
- Prevention and management
- Prevention: examine and image the CMC pre-operatively; address CMC disease simultaneously or stage CMC arthroplasty first. Management: CMC arthroplasty (trapeziectomy with LRTI) if symptomatic and refractory
- Incidence
- 1-3% (dorsal approach)
- Recognition
- Numbness over the radial thumb pulp; painful neuroma; positive Tinel sign at the approach site
- Prevention and management
- Prevention: identify the radial digital nerve in the proximal wound before deepening; protect with a vessel loop. Management: if recognised intra-operatively, repair primarily; if delayed, explore and manage the neuroma (excision and burial or nerve repair/graft)
- Incidence
- 1-5% (plate fixation)
- Recognition
- Painful triggering or snapping of the EPL over the plate; loss of IP extension; palpable gap in EPL continuity
- Prevention and management
- Prevention: place the plate ulnar to the EPL; use a low-profile plate; interpose soft tissue. Management: EPL rupture — reconstruct with a tendon transfer (EIP to EPL) and remove the plate; prominence without rupture — plate removal if symptomatic
Viva & Exam Focus
FUSIONFUSION — indications for thumb MCP arthrodesis
POSITIONPOSITION — fusion angle and key technical points
Clinical Decision Scenarios
Practise clinical reasoning and management decisions out loud
“A 58-year-old manual labourer presents with a painful, unstable right thumb MCP joint. He sustained a gamekeeper's thumb injury 3 years ago, had a UCL reconstruction using a palmaris longus graft 2 years ago, and now has recurrent valgus instability with pain during pinch grip. Radiographs show MCP joint space narrowing and volar subluxation of the proximal phalanx. How do you proceed?”
“A 52-year-old woman with longstanding rheumatoid arthritis presents with a Z-collapse deformity of the right thumb. She has dorsal subluxation at the CMC joint, volar subluxation and adduction at the MCP joint, and a mild hyperextension deformity at the IP joint. Her main complaints are pain and inability to grip objects. Describe your surgical plan.”
“You are performing a thumb MCP arthrodesis with a headless compression screw on a 42-year-old carpenter with post-traumatic MCP arthritis. Intra-operatively, after resecting the articular surfaces and positioning the temporary K-wire, you notice that the fusion surfaces are not perfectly congruent — there is a small gap on the ulnar side. What do you do?”
Key diagnosis points
- Primary MCP arthritis is uncommon — more often post-traumatic or rheumatoid; CMC arthritis is far more prevalent in isolation
- Chronic UCL insufficiency: valgus stress test in 30 degrees MCP flexion isolates the proper UCL; volar subluxation indicates a complete tear
- Stener lesion: UCL displaced superficial to the adductor aponeurosis — cannot heal, requires acute repair; a chronic failed repair leads to fusion
- Z-collapse (rheumatoid): CMC dorsoradial subluxation plus MCP volar subluxation plus IP hyperextension — a three-link deformity
- Screen the CMC and IP joints before MCP fusion — untreated coexistent pathology is the commonest reason for persistent symptoms
Surgical anatomy
- The MCP is a condyloid joint: biconvex metacarpal head, biconcave proximal phalanx base; collateral ligaments taut in flexion
- Dorsal approach: between EPB (radial) and EPL (ulnar); the radial digital nerve crosses into the dorsal wound proximally — identify and protect
- Proper UCL: origin at the metacarpal dorsal tubercle to the volar edge; insertion at the proximal phalanx base; the primary valgus restraint
- MCP flexion-extension arc: 5 degrees extension to 60 degrees flexion; the useful arc is 5-20 degrees, so fusion at 10-15 degrees sacrifices little
- The CMC provides opposition and circumduction; the IP provides tip flexion — these are the dominant functional arcs above and below the MCP
Indications
- Chronic UCL insufficiency with instability and secondary arthritis, or a failed prior reconstruction — the primary indication
- Post-traumatic MCP destruction with combined arthritis and instability
- Rheumatoid Z-collapse: MCP arthrodesis stabilises the middle link, combined with CMC LRTI
- Primary MCP osteoarthritis refractory to non-operative treatment for greater than 6 months (uncommon in isolation)
- Failed MCP arthroplasty (silicone or pyrocarbon) — salvage to fusion
Operative technique — key steps
- Longitudinal dorsal incision centred on the MCP, slightly ulnar to avoid the radial digital nerve
- Identify the radial digital nerve in the proximal wound and protect it with a vessel loop throughout
- Develop the interval between EPB (radial) and EPL (ulnar) — it opens directly onto the MCP capsule
- Longitudinal capsulotomy, preserving capsular tissue for closure
- Resect the metacarpal head and proximal phalanx base to flat, bleeding cancellous bone
- Place a temporary K-wire at 10-15 degrees flexion with slight pronation — check pinch clinically and on fluoroscopy
- Definitive fixation: headless screw (good bone), plate (poor bone or rheumatoid), or tension band (low cost)
- Close the capsule, extensor interval, subcutaneous tissue and skin — thumb spica cast with the IP free
Fixation options
- Headless compression screw: best for good bone stock; compression across the fusion site; no hardware removal needed; 90-97% union
- Dorsal mini-plate: most rigid fixation; highest union rate (95-100%); best for osteoporotic bone; 10-20% hardware removal rate
- Tension band wiring: low cost; 85-95% union; requires hardware removal at 4-6 weeks; K-wire migration risk
- Crossed K-wires alone: least rigid; 80-90% union; no compression; reserve for very low-resource settings
Fusion position
- 10-15 degrees MCP flexion — reproduces the natural thumb resting posture
- Slight pronation (radial deviation) — aligns the thumb pulp opposite the index pad for pulp-to-pulp pinch
- Fusing in excessive extension eliminates effective pinch; fusing in excessive flexion shortens the pinch distance
- Confirm the position clinically (thumb pulp meets the index pad) AND on fluoroscopy before definitive fixation
- Use a temporary K-wire to hold the position while checking — adjust before committing to a screw or plate
Danger zones
- Radial digital nerve: crosses into the dorsal wound proximally — identify before skin-flap elevation; injury causes neuroma and pulp numbness
- Sclerotic bone surface: inadequate resection is the commonest cause of nonunion — resect to bleeding cancellous bone
- EPL tendon: plate or K-wire irritation can cause triggering or rupture — place the plate ulnar to the EPL; use low-profile implants
- CMC joint: failure to address coexistent CMC arthritis leaves persistent basal thumb pain
- IP joint: pre-existing IP arthritis may worsen after MCP fusion due to compensatory overload
Complications
- Nonunion: 5-15%; risk factors — smoking, diabetes, osteoporosis, inadequate bone preparation, poor fixation
- Malunion or malposition: 3-8%; prevent with a temporary K-wire and a clinical pinch check before definitive fixation
- Hardware prominence: 5-20% (plate highest); counsel pre-operatively; plan removal after confirmed union
- IP overload: 5-10% progressive over years; screen pre-operatively; manage with splinting, injection or IP fusion
- Infection: less than 1% deep; radial digital nerve injury 1-3%; EPL irritation 1-5% (plate)
Post-operative protocol
- Thumb spica cast or splint for 4-6 weeks with the IP joint free — active IP motion from day 1
- X-rays at 4 and 8 weeks to assess union progression
- Protective splint weaning from 6-8 weeks; strengthening from 8-12 weeks
- Return to light work 8-12 weeks; heavy manual work 3-4 months; driving when safe (6-8 weeks)
- Hardware removal (plate) after confirmed union at 4-6 months if symptomatic
Background & Evidence
Functional anatomy. The thumb MCP is a condyloid joint with a biconcave proximal phalanx base articulating with a biconvex metacarpal head. The metacarpal head is wider volarly than dorsally, which contributes to the natural slight flexion of the resting thumb. The collateral ligaments are eccentrically attached — taut in flexion and lax in extension — which is why the UCL is examined with the MCP in flexion. The capsule is thin dorsally (allowing surgical access) and reinforced volarly by the volar plate. Why fusion at 10-15 degrees sacrifices little. The total MCP flexion-extension arc is only 5-10 degrees of extension to 50-60 degrees of flexion, and most thumb function (pinch, grip, opposition) occurs with the MCP between 5 and 20 degrees of flexion. The CMC joint provides the majority of opposition and circumduction, and the IP joint provides tip flexion for fine pinch — so fusing the MCP at 10-15 degrees removes relatively little useful motion. Collateral ligament complex and the unstable MCP. The proper ulnar collateral ligament runs from the ulnar side of the metacarpal head (dorsal tubercle to volar edge) to the base of the proximal phalanx and is the primary restraint to valgus (radial deviation) stress during pinch, preventing volar subluxation of the proximal phalanx. It is tested by applying valgus stress with the MCP in 30 degrees of flexion, which tightens the proper UCL and isolates it from the accessory ligament. A Stener lesion — the UCL torn and displaced superficial to the adductor aponeurosis — cannot heal and requires acute repair; chronic insufficiency after a failed repair is a classic route to MCP fusion. The accessory UCL (from the volar metacarpal neck to the volar plate and ulnar sesamoid) stabilises the volar plate and is taut in extension. The radial collateral ligament restrains varus stress and rarely needs reconstruction in isolation. Extensor tendons and the dorsal interval. The EPL passes over Lister's tubercle at the wrist and crosses dorsally to insert on the distal phalanx base; at the MCP level it is the most ulnar dorsal extensor and forms the ulnar boundary of the approach interval. The EPB inserts on the proximal phalanx base (dorsal and slightly radial) and forms the radial boundary; it may be absent or fused with APL in up to 30% of individuals. APL lies radial to EPB, inserting on the first metacarpal base, and is not routinely encountered unless the incision is extended proximally. The standard dorsal approach proceeds between EPB (radial) and EPL (ulnar), identified proximal to the MCP and developed distally onto the capsule. Neurovascular structures at risk. The radial digital nerve runs volar to the extensor tendons, crossing into the dorsal plane in the proximal wound, where it lies superficially in the subcutaneous fat and is vulnerable during skin-flap elevation — it must be identified and protected before the interval is developed. The ulnar digital nerve lies volar-ulnarly and is not routinely encountered unless dissection extends volarly. Small dorsal sensory branches from the superficial radial nerve supply the MCP dorsum and are transected during the skin incision (warn the patient about a small area of numbness). The volar blood supply is dominant, so avoid excessive dorsal periosteal stripping to preserve cancellous vascularity for fusion healing. Epidemiology and outcomes. Primary MCP osteoarthritis is uncommon in isolation and is more often post-traumatic or part of pan-trapezial disease; rheumatoid disease is a major driver through the Z-collapse pattern. Across published series, thumb MCP arthrodesis reliably eliminates MCP pain and provides a stable platform for pinch and grip, with union in 85-95%, significant pain relief in 85-95%, and patient satisfaction of 80-95%. Fixation-method studies consistently show that all techniques achieve acceptably high union rates and that functional outcomes are determined primarily by fusion position, bone preparation and rehabilitation rather than by the specific device — hardware-related complications (especially plate prominence and removal) are the main differentiator between methods.
References
Union Rates and Complications After Thumb Metacarpophalangeal Fusion
- Comparative evaluation study of thumb MCP fusion outcomes across multiple fixation methods in a large cohort
- Reported overall high union rates consistent with published literature; identified fixation-specific trends in complication profiles
- Nonunion and hardware-related complications were the most frequent reasons for reoperation
Arthrodesis of the metacarpophalangeal joint of the thumb using a Herbert screw
- Described the Herbert headless compression screw technique for thumb MCP arthrodesis with step-by-step operative details
- Achieved reliable union with the compression screw approach, confirming its suitability as a low-profile fixation option
- Emphasised accurate screw trajectory and adequate bone stock as prerequisites for success with this technique
Comparison of Fusion Rates/Complications Between Different Types of Thumb Metacarpophalangeal Fusion Techniques
- Directly compared fusion rates and complication profiles between screw, plate, tension band and intramedullary fixation for thumb MCP arthrodesis
- All fixation methods achieved acceptably high union rates; no single technique was clearly superior for all outcome measures
- Hardware-related complications varied by method — plate fixation had the highest rate of hardware removal, screw fixation the lowest
Complications and Unplanned Reoperation After Thumb Metacarpophalangeal Arthrodesis
- Large series identifying the incidence and risk factors for complications and unplanned reoperations after thumb MCP arthrodesis
- Nonunion and symptomatic hardware were the leading causes of reoperation; plate fixation was associated with the highest hardware removal rate
- Smoking and poor bone quality were identified as significant modifiable risk factors for nonunion
Fixation method does not influence functional outcomes after thumb metacarpophalangeal arthrodesis
- Compared patient-reported functional outcomes across different fixation methods for thumb MCP arthrodesis in a multicentre cohort
- Found no significant difference in grip strength, pinch strength, or patient-reported outcome scores between fixation techniques
- Union rates were comparable across methods when bone preparation and post-operative protocol were standardised